
Research Article | DOI: https://doi.org/10.31579/2690-1919/170
1 Bait Balev Nesher, Department of Rehabilitation.
2 Bait Balev Nesher, Department of Rehabilitation.
3 Bait Balev Nesher, Department of Rehabilitation.
4 Bait Balev Nesher and The Ruth and Bruce Rappaport Faculty of Medicine, Technion, Israel Institute of Technology, Haifa, Israel.
*Corresponding Author: Jochanan E. Naschitz, Bait Balev Nesher and The Ruth and Bruce Rappaport Faculty of Medicine, Technion, Israel Institute of Technology, Haifa, Israel.
Citation: Zalyesov O., Badarny M., Zaygraykin N., Jochanan E. Naschitz (2021). Inpatient Rehabilitation after Hip Fracture: Predicting Success in Rehabilitation based on Preliminary FIM. J Clinical Research and Reports, 8(1); DOI:10.31579/2690-1919/170
Copyright: © 2021 Jochanan E. Naschitz, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 06 May 2021 | Accepted: 13 May 2021 | Published: 21 May 2021
Keywords: hip fracture; rehabilitation; functional independence measure; FIM
Background: Predicting success of inpatient rehabilitation after hip fracture is an unmet challenge
Objective: To assess whether a first impression Functional Independence Measure (FIM) before comprehensive evaluation may be useful to predict success in rehabilitation
Setting: Geriatric rehabilitation center.
Design: Retrospective observational study
Subjects: 42 consecutive elderly patients with proximal hip fracture.
Methods: The Functional Independence Measure (FIM) was assessed on the day of admission by a nurse (PreFIM), on day 3-5 by a multidisciplinary team (FimAdm) and on the day before discharge by the same multidisciplinary team (FIMDis). The potential of motor PreFIM to predict rehabilitation success, corresponding to motor FIMDis >58, was assessed, along with the length of stay in rehabilitation (LOS).
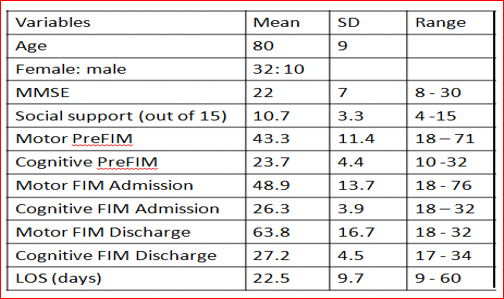
Results: The mean motor PreFIM was 43.3 (SD 11.4), motor FIMAdm 48.9 (SD 13.7), motor FIMDis 63.8 (SD 16.7), LOS 22.5 days (SD 9.7). Motor PreFIM predicted motor FIM discharge >58, the surrogate measure for success of rehabilitation, with 76.7% sensitivity and 83.3% specificity. Motor PreFIM relation to LOS was statistically insignificant.
Conclusions: In a population of disabled elderlies, the motor PreFIM on admission-day was helpful to predict success in rehabilitation after hip fracture, but not the necessary duration of rehabilitation. Large prospective studies are needed to validate this data.
Numerous factors affect the outcomes of rehabilitation in patients with hip fractures, including age, sex, pre-fracture functional ability and frailty, cognitive status, affective status, patient motivation and preferences, comorbidity, the number of treatments, as well as family and social support [1-5]. It would be important for clinicians to predict success of rehabilitation better than clinical judgment alone. The aim of the present study was to find an instrument, which is generally available, quick and easy to use, and might enhance the clinician’s judgment in defining situations when rehabilitation is futile. The candidate was the Functional Independence Measure (FIM) assessed on the admission-day by a nurse (PreFIM) before rehabilitation is started.
The Institutional Review Board approved this retrospective observational study and waived the need for obtaining informed consent. The study was performed in a 40 bed rehabilitation department that admits mainly orthopedic patients. Included were consecutive patients aged 65 years or older transferred from orthopedic surgery to the geriatric rehabilitation ward. Excluded were non-cooperative subjects, as well as patients having an infected operation site, and those temporarily prohibited to tread. The following variables were appraised: demographic data, mini mental state examination of Folstein [6], social support [7], and functional independence measure [8].
The Functional Independence Measure (FIM) is a tool used explore an individual's physical, psychological, and social functions and to monitor the progress under rehabilitation. The FIM has two subscales: the motor subscale, consisting of 13 items related to self-care, transfers, and locomotion, and the cognitive subscale, consisting of 5 items related to comprehension, expression, and memory. Each item is assigned a rating of 1–7, where 1 denotes the necessity for assistance and 7 denotes complete independence [8]. The preliminary FIM (PreFIM) was administered on the day of admission by a specifically initiated and experienced nurse before rehabilitation was begun. Admission FIM (FIMAdm) was provided by corroboration of a multidisciplinary teem 3-5 days after admission, having already qualified the patient's abilities over a few days of rehabilitation. FIM on the wake of discharge from rehabilitation (FIMDis) was provided by the same multidisciplinary team including physicians, occupational therapists, physical therapists, social workers, speech and language therapists, dietitians, and nurses. The following variables were calculated: motor PreFIM, motor FIMAdm, motor FIMDis, motor FIMDis >58 indicating that usually a person may be discharged to the community [9], the absolute motor functional gain (i.e. motor FIMDis minus motor FIMAdm), the length of stay (LOS), and the motor PreFIM sensitivity and specificity in predicting motor FIMDis >58.
Rehabilitation involved the diagnosis of a person’s problems and needs, defining rehabilitation goals, and therapeutic interventions. Rehabilitation was provided by the multidisciplinary team consisting of physicians, occupational therapists, physical therapists, social workers, speech and language therapists, dietitians, and nurses. The patients received 5 days per week standard physical therapy (i.e., walking, climbing stairs, balance, muscle strength, and range of motion) and occupational therapy (i.e., basic ADL, instrumental ADL, and environment advice).
Statistical analysis used descriptive statistics, Student’s t test, Pearson’s correlation, Receiver Operating Characteristic curve, as appropriate. P < 0.05 was considered significant.
The data of 47 consecutive patients who met the inclusion criteria were reviewed. Five patients could not complete the rehabilitation because of intercurrent illness needing hospitalization and were excluded from the analysis. Patient demographics, FIM scores at different times, the LOS and ΔFIM/LOS are shown in Table 1.
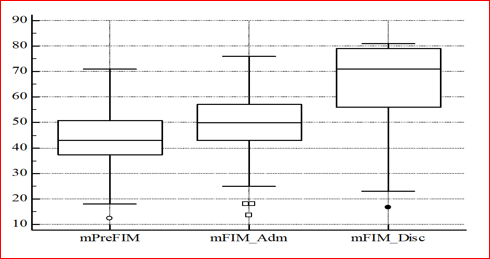
Motor FIM changes from admission to discharge are shown in Figure 1.
Motor FIM Discharge >58 was found in 28 patients. The total FIM (motor and cognitive) improvement from admission to discharge was by 16.6 points (SD 9.9). The mean functional gain per day, i.e. total FIM at the time of discharge – total FIM on admission was of 0.8 points (SD 0.6). Prediction of rehabilitation outcome by motor Pre FIM, the sensitivity and specificity in relative to motor FIM Discharge >58, are shown in Figure 2.
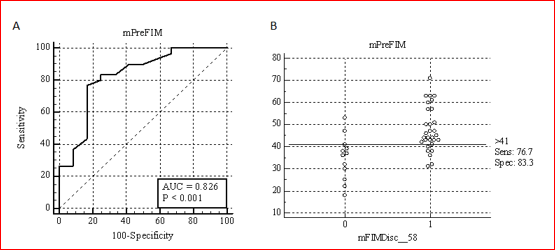
According to cutoff motor PreFIM >41, 24 cases were true positive, 9 true true negative, 3 false positive and 6 false negative, accuracy 77%.
The correlation between motor PreFIM and the daily functional gain, i.e. progress in rehabilitation (Figure 3), was calculated according to the equation:
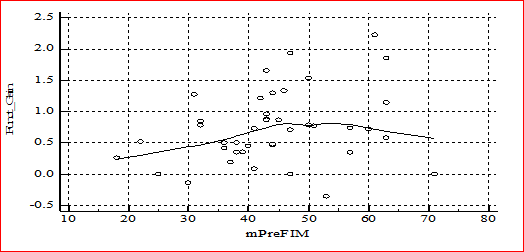
Daily motor functional gain = (motor FIM Discharge – motor FIM Admission)/LOS.
ROC curve analysis confronting LOS with FIM Discharge >41 was also insignificant statistically.
In this cohort of elderly patients assigned for inpatient rehabilitation after hip fracture, the motor PreFIM assessed by a nurse on admission day, proved to have 77% accuracy in predicting rehabilitation success, the latter corresponding to motor FIM discharge >58.
The validity of FIM instrument for determining outcomes of rehabilitation has been in a study of 117.168 Medicare beneficiaries receiving inpatient rehabilitation for hip fracture in 2007-2009. A discharge motor FIM score of 58 yielded the best balance in sensitivity and specificity for classifying patients by discharge setting. FIM motor was equally effective as FIM total and more effective than FIM cognition in discriminating patients discharged to the community from those discharged to an institution. Moreover, FIM motor ratings alone were as effective as a multivariable model in discriminating patients discharged to the community from those discharged to an institution [9]. Indeed, from a clinical perspective, a diagnostic tool based on a single standard measure and a defined threshold of success is more practical and meaningful than values obtained from a composite model [9, 10]. This understanding was echoed in a survey of consultant members of the British Society of Rehabilitation Medicine [11].
Beyond commonsense used for the first triage, the preliminary FIM assessed by a nurse on admission-day was a valuable instrument to predict success in rehabilitation but not the pace of recovery. As shown in Figure 2, the motor PreFIM did not correlate with the daily motor functional gain. For the disadvantaged, a longer stay in rehabilitation compensated for slow improvement (Figure 3), also indicated by the lack of correlation between LOS and motor FIM discharge >41. Indeed, predicting success of inpatient rehabilitation after hip fracture is challenging because the outcome is affected by numerous factors in addition to treatment, including demographics, family and social support, patient motivation and preferences, which are beyond the control of rehabilitation facilities [12]. In practice, the use of one representative predictor of outcome, e.g. motor FIM discharge, is a necessary compromise.
Whether as simple a tool as the motor PreFIM can be an aid to predict when rehabilitation is futile remains to be answered by larger studies, combining the experience of different institutions in different populations. Data of the present study suggest that this might be possible.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
