
case Report | DOI: https://doi.org/10.31579/2690-4861/647
1 Dipartment II clinica Sport Istituto Ortopedico Rizzoli, Bologna, Italy.
2 Dipartment Rizzoli-Argenta Istituto Ortopedico Rizzoli, Argenta, Italy.
3 Clinical Trial Center, IRCCS Istituto Ortopedico Rizzoli, Bologna, Italy.
*Corresponding Author: Tosca Cerasoli, Dipartment II clinica Sport Istituto Ortopedico Rizzoli, Bologna, Italy.
Citation: Tosca Cerasoli, Marco Zaffagnini, Vito Coco, Costanza Musiani, Loredana Mavilla, et al, (2024), Innovative Custom-Made hip Resurfacing to Treat Osteoarthritis in the Presence of Retained Femoral Hardware: a Case Report, International Journal of Clinical Case Reports and Reviews, 20(5); DOI:10.31579/2690-4861/647
Copyright: © 2024, Tosca Cerasoli. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 09 December 2024 | Accepted: 19 December 2024 | Published: 30 December 2024
Keywords: THA; resurfacing hip arthroplasty; custom made prosthesis; 3D THA; hip; retained hardware; custom-made hip resurfacing
Background
Treating hip osteoarthritis in the presence of retained proximal femoral hardware presents significant challenges. Conventional total hip arthroplasty techniques require hardware removal, which increases surgical complexity and risks and may not always be feasible, with reported success rate ranging from 85% and 95%. This case describes the innovative use of a custom-made hip resurfacing prosthesis combined with 3D-printed cutting guides to address the challenges posed by the non-removable hip screw plate.
Case Presentation
A 68-year-old female presented with advanced hip osteoarthritis and a retained hip screw plate that could not be removed due to extensive osseointegration. Conventional implants were not feasible as the plate and screw occupied the intramedullary space. A custom-made hip resurfacing prosthesis was designed to bypass the hardware entirely. 3D-printed cutting guides were utilized to ensure precise preparation of the femoral head surface, which enabled accurate implant placement to avoid the screw. Although an early postoperative infection occurred, it was successfully managed, and the patient achieved excellent functional recovery.
Discussion
This case highlights the limitations of existing solutions for managing retained hardware during total hip arthroplasty. While cutting guides are widely used in other orthopedic fields, their application in hip resurfacing with non-removable hardware is novel. These 3D-printed cutting guides, which are typically employed to enhance surgical precision in other procedures, were instrumental in ensuring accurate femoral head preparation and implant alignment in this case, thus reducing surgical risks and optimizing outcomes. This case demonstrates how the use of custom-made resurfacing implants and 3D-printed guides can address complex surgical challenges that conventional techniques cannot resolve, and, to the best of the authors’ knowledge, it is the first reported case that utilized a custom-made resurfacing prosthesis combined with 3D-printed cutting guides.
The treatment of hip osteoarthritis (OA) in the presence of retained hardware poses a significant challenge for orthopedic surgeons. While cases of total hip arthroplasty (THA) with retained hardware have been described in the literature [1], these typically allow the use of standard resurfacing implants. Reported success rates for THA with retained hardware range between 85% and 95%, depending on the complexity of the case and the implant used [8-9]. However, these procedures are associated with increased risks of complications, including infection and implant instability, particularly when hardware removal is performed concurrently or in a staged manner [12-13]. Additionally, the presence of hardware often limits implant choice and may necessitate complex preoperative planning to achieve optimal outcomes [15-16]. In our case, the proximal femoral screw precluded the use of any stem, which necessitated a custom-made approach.
Custom-made prostheses are primarily utilized in cases involving substantial bone defects, which are often found in oncology or severe femoral deformities [2-4]. Additionally, 3D technologies, such a custom-made implant and cutting guides, have been used successfully to assist osteotomies or address extensive bone loss [5-7]. Recent advancements in 3D planning and patient-specific implants have demonstrated improved outcomes in cases of severe femoral deformities or medullary canal obstruction [11-15]. Despite these advancements, there is a paucity of literature addressing the management of cases where standard femoral resurfacing implants cannot be utilized due to non-removable hardware.
This case report details the innovative use of a custom-made hip resurfacing prosthesis, supported by 3D-printed guides, in a patient with advanced hip OA and an irremovable hip screw plate. To the best of the authors’ knowledge, this is the first reported case that utilized a custom-made resurfacing prosthesis combined with 3D-printed cutting guides to address the challenges of hip resurfacing in the presence of a non-removable hip screw.
A 68-year-old female patient presented with progressive left hip pain and limited mobility, particularly during flexion and external rotation. Her medical history included a left femoral neck fracture that was treated in 1979 with a hip screw plate as well as comorbidities, such as gastroesophageal reflux disease, type 2 diabetes mellitus, ischemic heart disease, and hypertension. Imaging revealed severe left hip OA with marked joint space narrowing and femoral head deformity (Figure 1).
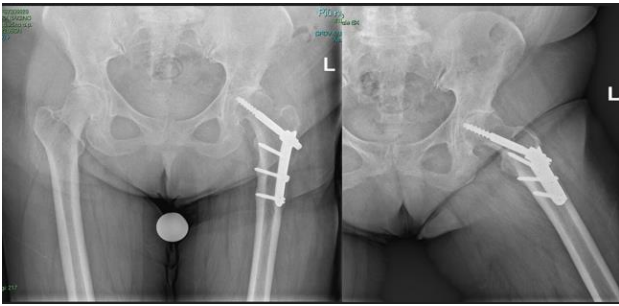
Figure 1: Preoperative X-ray showing the fixation devices and severe osteoarthritis.
The patient initially underwent conservative treatment, including pain management and physiotherapy. However, her symptoms worsened, which led to the decision to perform THA. A preparatory attempt to remove the internal fixation hardware was unsuccessful due to severe osseointegration. Because the position of the femoral screw prevented the placement of any stem, including that of a simple resurfacing prosthesis, the use of a custom-made implant was necessary (Figure 2).

Figure 2: Custom-made instruments: cutting guides, custom-made femoral head, and custom-made acetabular cup with polyethylene liner.
To address this challenging case, a custom-designed femoral head resurfacing prosthesis with a small peg was employed. The implant and the patient-specific cutting guides were designed based on the patient’s CT scans. The primary difficulty involved the precise positioning of the guide wire, the reaming of the femoral head, and the placement of the implant while avoiding interference between the stem and the retained cephalic screw. An additional challenge was the unusually small size of the femoral head (42 mm).
Because no standard resurfacing cup of this size was available, a custom-made implant was also developed for the acetabulum. A hemispherical cup with a cross-linked polyethylene liner pre-assembled within an ultra-thin, 3D-printed metal shell was designed. This approach allowed the outer diameter of the cup to be maintained at 50 mm. The implants and their corresponding disposable instruments were designed in collaboration with Adler Ortho (Cormano, Italy).
In March 2023, the patient underwent resurfacing THA using a direct lateral approach. The incision was made along the previous surgical scar, and the soft tissues were meticulously dissected to expose the femoral head (Figure 3).
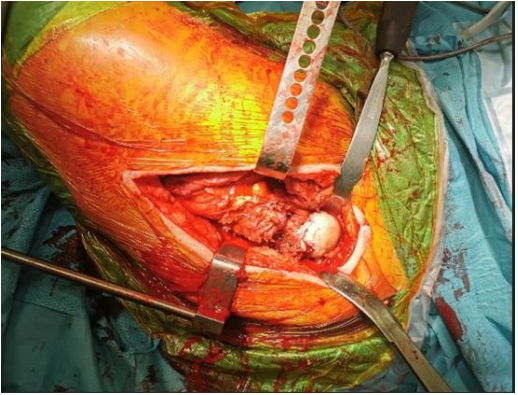
Figure 3: Intraoperative image of the proximal femur
Partial detachment of the gluteal muscles provided sufficient access to the hip joint. Custom-made cutting guides, tailored to the unique anatomy of the femoral head, were positioned directly on the bone surface (Figure 4).

Figure 4: Steps for the preparation of the femoral head: placement of the custom-made guide, reaming of the femoral head using appropriately sized reamers in progressively larger diameters, and the femoral head prepared for implant placement.
These guides facilitated the precise resection of the external portion of the femoral head and allowed the prosthesis stem to avoid interference with the cephalic screw.
The acetabulum was prepared using standard reamers of progressively larger sizes. The femoral head prosthesis, which was coated with titanium nitride to enhance biocompatibility, was cemented onto the femoral surface, thus achieving an optimal articulation (Figure 5).

Figure 5: Intraoperative image showing the femoral implant, the acetabular implant, and their articulation.
Fluoroscopic imaging was used to confirm proper alignment of the components (Figure 6). The procedure was completed with layered closure and the placement of a surgical drain.

Figure 6: Intraoperative radiological assessment of the positioning of the acetabular component and the femoral head.
Initially, the patient mobilized with two crutches while bearing partial weight on the operated limb. However, the surgical wound failed to heal properly, which prompted cultures that revealed a superficial infection with methicillin-resistant Staphylococcus aureus. Surgical debridement was performed in May 2023. Vacuum-assisted closure therapy was applied for ten days, followed by a seven-week course of targeted antibiotics. Repeat cultures and imaging confirmed the resolution of the infection.
Rehabilitation resumed with steady progress. By June 2023, the patient walked with one crutch and demonstrated improved strength and
mobility. At her September 2023 follow-up, she was walking independently without aids, with a range of motion (ROM) of 0–90° flexion and 0–30° abduction. By December 2023, the patient reported no pain, with ROM exceeding 90° and unrestricted rotation. At her latest follow-up in March 2024, she demonstrated excellent functional outcomes, including pain-free ambulation, independent stair climbing, and the resumption of daily activities (Figure 7). Occasional mild discomfort related to weather changes was her only residual symptom.
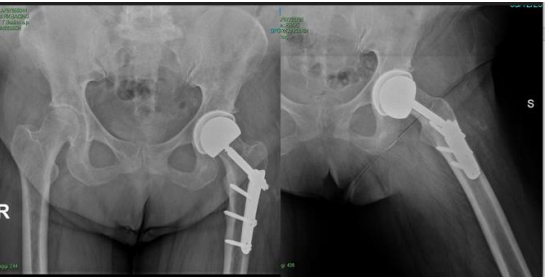
Figure 7: One-year postoperative follow-up showing proper prosthesis positioning and no interference with the fixation devices.
The management of hip OA in the presence of retained proximal femoral hardware is a significant challenge in orthopedic surgery. Non-removable hardware, such as intramedullary nails or femoral screws, complicates the surgical approach and restricts implant options. In this case, the retained proximal femoral screw prevented the use of even the small central peg typically required for hip resurfacing implants, which necessitated an innovative approach to achieve stable fixation and precise femoral preparation [8,9].
Custom-made implants have been extensively utilized for cases involving severe bone loss, complex deformities, or oncological resections [3,4,10]. However, their application in the context of hip resurfacing with retained hardware remains a novel solution. Our approach involved designing a prosthesis that bypassed the anatomical constraints imposed by the screws and allowed for secure fixation and optimal load distribution without the need for intramedullary support. Additionally, a unique innovation in this case was the use of 3D-printed cutting guides to prepare the femoral head surface. While 3D cutting guides have been widely employed in other orthopedic fields, such as tumor resections and deformity corrections [5,11], their use for resurfacing prostheses in the presence of retained hardware represents a significant advancement.
Complications are a well-recognized concern in THA following internal fixation, with studies demonstrating an increased risk of adverse events, including infections and hardware-related issues [12,13]. In our case, an early superficial infection caused by methicillin-resistant Staphylococcus aureus (MRSA) was successfully managed with surgical debridement, vacuum-assisted closure therapy, and targeted antibiotics. This complication aligns with the literature that reported higher infection rates in cases involving retained hardware, which further underscores the importance of meticulous surgical planning and postoperative management [13].
The efficacy of resurfacing implants in posttraumatic OA is well supported by the literature, with studies highlighting the favorable outcomes of cemented prostheses in such cases [14,15]. Similarly, large studies have demonstrated that resurfacing implants maintains good functional results even in the presence of retained hardware, although these cases typically rely on standard designs and do not involve patient-specific customizations [8,9,16]. Our case demonstrates how a fully custom-made approach, combined with cutting guides, can expand the applicability of resurfacing to more complex scenarios.
This case also highlights the broader potential of cutting guides and custom-made implants in addressing anatomical and technical challenges that conventional methods cannot overcome. However, limitations persist, including the time and resources required for designing and manufacturing custom implants, as well as the limited availability of advanced imaging and 3D printing technology in certain settings. Long-term outcome data for such innovative solutions remain scarce, which necessitates further research to validate their durability, cost-effectiveness, and broader applicability.
This case demonstrates how the integration of custom-made implants and 3D-printed guides can address complex surgical challenges that conventional techniques cannot resolve. The approach employed here not only highlights the potential of these technologies but also underscores their ability to expand the indications for hip resurfacing arthroplasty in the presence of retained hardware. Further studies are warranted to evaluate the reproducibility, cost-effectiveness, and long-term outcomes of such innovative solutions.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
