
Review Article | DOI: https://doi.org/10.31579/2692-9392/147
1College of Medicine, University of Florida.
*Corresponding Author: Brandon Lucke-Wold, Department of Neurosurgery, University of Florida, Gainesville.
Citation: Elizabeth Klaas, Shahd Mohamed, Jordan Poe, Ramya Reddy, Abeer Dagra and Brandon Lucke-Wold, (2022) Innovative Approaches for Breast Cancer Metastasis to the Brain. J. Archives of Medical Case Reports and Case Study, Doi:6(4); DOI:10.31579/2692-9392/147
Copyright: © 2022 Brandon Lucke-Wold, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 22 August 2022 | Accepted: 03 September 2022 | Published: 22 September 2022
Keywords: breast cancer; brain metastasis; emerging treatments; surgery; pre-clinical data
Breast cancer metastasis is a continued concern for patients with recent development in our understanding of disease progression. In this paper, we highlight the pathophysiology behind breast cancer metastasis. Blood brain barrier disruption plays a critical component in progression. We then investigate the current treatment strategies and recommended guidelines. This focuses on radiation and medical management. Finally, we address the role of surgical intervention. The data is organized into tables and figures to highlight key components. Finally, we address emerging treatments and pre-clinical data. The paper will serve as a user-friendly guide for clinicians and researchers to help formulate a strategy to manage breast cancer metastasis patients sufficiently.
Breast cancer is among the most commonly diagnosed cancers globally, and 10-15% of women with stage IV breast cancer are estimated to have metastasis to the brain [1]. Younger age at the time of breast cancer diagnosis, tumor size, nodal involvement, histological grade, and aggressive breast cancer subtypes, including human epidermal growth factor receptor 2 (HER 2) positive breast cancer and triple negative breast cancer, are risk factors associated with breast cancer metastasis to the brain [2,3].
Brain metastasis is a multi-step, highly dynamic process, and many aspects of the pathophysiology of breast cancer metastasis to the brain are still unknown. Similar to breast cancer metastasis to other sites, including bone, liver, and lungs, a series of key steps are involved including local invasion from the primary tumor, intravasation, and survival of tumor cells in circulation to the escape of cells from the circulatory system, extravasation, and formation of metastatic lesion following adaptation to the local microenvironment [4].
However, the brain blood barrier (BBB), a selective diffusion barrier characterized by non-fenestrated epithelium and tight junctions, is a distinct feature of brain metastasis. Key molecular features that mediate extravasation across BBB play a key role in metastasis. Cyclooxygenase 2, α2,6-sialyltransferase ST6GALNAC5, and the epidermal growth factor (EGFR) ligand HBEGF have been identified as mediators of extravasation as well as VEGF and CXCR4/CXCL12 [4,5]. Tumor cells also interact with supporting cells in the CNS microenvironment, including glial cells, microglia, and astrocytes, and activate pathways that create a favorable microenvironment for colonization [6].
Although advances in breast cancer diagnosis and treatment have increased life expectancy among patients, the incidence of breast cancer brain metastasis (BCBM) continues to rise resulting in poorer prognosis, lower quality of life, and shorter survival. A multidisciplinary, individualized approach that involves systemic and local treatment options or a combination of therapies is necessary. However, limited penetration of therapeutic agents through the blood brain barrier further complicates treatment [7].
Surgery, stereotactic radiosurgery, and whole brain radiotherapy are current mainstays in local management of intracranial disease. Systemic treatments may include targeted therapy, immunotherapy, and chemotherapy. Hormone therapy may also be used to treat hormone receptor positive breast cancer metastasis [8].

Figure 1: Breast cancer may metastasize to other organs mostly via hematogenous spread. Metastasis to brain require intravasation to blood vessels and extravasation through the BBB mediated by various molecular markers. [Adapted from “Breast Cancer to Brain Metastasis”, by BioRender.com (2022). Retrieved from https://app.biorender.com/biorender-templates]
Current treatment modalities
Breast cancer accounts for at least 30% of cancers in females, occurring in approximately 12.8% of the female population, or about 1 in every 8 women [9]. In late stages of the disease, tumors can metastasize in the lungs, liver, bone, and brain. Breast cancer brain metastasis (BCBM) is the most fatal of metastatic breast cancer and occurs in between 10-30% of metastatic breast cancer cases [6,10]. Breast cancer metastasis detection largely relies on clinical manifestations of disease spreading to other organs, including biopsies, imaging, and serum tumor markers. Earlier diagnosis usually gives a better survival rate for the patient as the disease can be treated faster, but current diagnostic tools are unable to detect the earliest stage of metastasis- when tumor cells are circulating in the bloodstream [10]. This makes predictions of disease progression difficult and can affect the outcome of the patient’s survival. Once lesions are detected, current therapeutic options are largely limited to chemotherapy, radiation therapy, or surgical intervention. However, these interventions leave a lot to be desired in terms of increasing life expectancy in patients with brain metastases due to the limiting blood-brain barrier that prevents chemical agents from reaching the brain and increases resistance to treatment.
Radiation
Radiation therapy works by radiating the DNA of tumor cells, breaking the DNA, and preventing cell replication and further tumor progression and growth. These cells die and result in shrinking of tumor size [11]. Patients who receive radiation therapy may receive it in combination with surgery or chemotherapy, or as a standalone treatment. Radiation for brain metastases is typically given via external beam radiation therapy. This means there is an instrument that sits outside of the patient’s body and delivers a beam of radiation to the designated treatment area [6]. There are a few types of external radiation therapy, but the most commonly used are stereotactic radiosurgery (SRS) and whole brain radiation therapy (WBRT).
There are three types of radiation beams that may be used, including photon, particle, and electron beam therapy [11]. Photon beam radiation therapy is the same type of radiation that is used when x-ray imaging is taken but at a higher concentration. This type of radiation is beneficial for its ability to reach deeper in the body, but also has higher potential for damaging healthy tissue surrounding the tumors. Both particle beams and electron beams are separate units of energy that are released in a stream of high-energy particles. These beams can travel deep into the body and release the radiation energy at a calculated distance. This results in delivering more precise radiation to tumors with minimal effect on normal tissue surrounding it. Both stereotactic radiosurgery and whole brain radiation therapy use photon beams to apply radiation from various angles to the metastases [11].
Patients with limited metastases in the brain can be treated with stereotactic radiosurgery, but it is standard practice if a patient has greater than 4 lesions then whole brain radiation therapy is recommended [12]. Whole brain radiation is used to deliver a uniform dose of radiation to the entire brain, with a typical minimum of at least 10 daily treatments [12].
Whole brain radiation therapy was first found to be efficacious in a study performed by Chao et al in the 1950s, who found that 63% of patients who received therapy had alleviated symptoms. They also found that there was no difference in response to the therapy for tumors stemming from radiosensitive tumors to radioresistant tumors, and that there was minimal toxicity and decreased morbidity associated with radiation therapy [13]. This study set the foundation for WBRT being implemented for treatment of brain metastases and becoming the gold standard therapy by the 1970s. Whole brain radiation therapy is currently used as a monotherapy for brain metastases, when best suited for the patient based on the number of lesions and location within the brain, or if SRS or surgery interventions are not sufficient [9]. One major drawback to this approach is that WBRT tends to have a higher risk for neurodegenerative effects, including decreased cognitive capabilities in patients [12].
Adverse effects of WBRT may be present in both the short term and the long term. Some acute toxicity effects include fatigue, decreased appetite, nausea, radiation-induced alopecia, and cerebral edema [8]. These symptoms may present within a few days after radiation therapy, but generally are self-limiting and resolve with minimal intervention or with the use of corticosteroids in the case of cerebral edema. Some delayed or long-term toxicities may include behavioral changes, memory loss, and other degenerative neurocognitive effects, which may resolve over time or may become permanent effects of radiation therapy. One study found that at one year post WBRT treatment, 48-89% of patients showed a decline in neurocognitive function [14]. Another study by Kocher et al showed that patients who receive WBRT after SRS or surgery have reduced relapse rate compared to an observed group of patients post SRS or surgery (59 to 27%). The risk of neurological decline must be considered while also considering that WBRT can reduce intracranial failure and neurological death by more than 15% [15].
Stereotactic radiosurgery uses targeted doses of high radiation to individually focus on each lesion. The center of each metastasis can receive up to twice the prescription dose given when given at a low isodose surface. This means that the center of the beam has the highest concentration of radiation and can be calculated to reach the center of a lesion to give the greatest dose possible while the outer edges receive a less concentrated amount. The benefit of using SRS is that normal brain tissue receives minimal radiation, up to 50% less than the prescribed dose. However, the greater number of lesions that are present in the brain also means more normal healthy tissue will be receiving radiation as well. This becomes a concern as healthy tissue may receive overlapping doses of radiation if the metastases are in close range of each other, compared to a single uniform dosage that is given with WBRT [12].
A study comparing dosimetry data in 5 patients with brain metastases who received radiation treatment showed that the biologically effective dose for SRS was around 3 times higher than for WBRT [12]. The average effective dose for normal tissue was lower in SRS (1.3-34.3%) than WBRT (<10>
Radiation may be used in combination with surgery to shrink the tumor to a reasonable size for surgical removal [11]. Regardless of the type of radiation therapy strategy that is used, this form of treatment has proven to be effective in treating brain metastases no matter the histology of the primary tumor and its radiosensitivity status [17]. This makes radiation therapy unique and especially useful in treating the disease, reducing symptoms caused by the tumors present in the brain, and increasing chances of survival as well as quality of life.
Chemotherapy
Chemotherapy is a longstanding systemic treatment for various cancers. While systemic therapy is not the initial choice for brain metastases, chemotherapy may be used if the primary tumors of the cancer are sensitive to it [16]. Another consideration of systemic treatment is the ability of the chemotherapeutic agent to cross the blood brain barrier (BBB). Both factors are important when contemplating chemotherapy as a treatment for brain metastases stemming from breast cancer.
The blood brain barrier is always a consideration when it comes to using chemical compounds as therapeutics in the brain. The BBB consists of 3 key components: a layer of endothelial cells, astrocytes, and pericytes. There are also tight junctions, upregulated by factors secreted by the astrocytes, embedded in the endothelial cell layer to create a diffusion barrier to prevent most substances from reaching the brain [18]. Pericytes compliment the endothelial cell layer, further regulating permeability of the BBB [19].
In brain metastases, it is possible that the tumors cause a degree of BBB breakdown (Figure 1), which can be detected via MRI imaging with contrast dye [16]. This breakdown occurs by breaking the tight junctions, making permeabilization of the endothelial layer possible [19]. While this disruption of the BBB allows for malignant cells to circulate in the vasculature of the brain to metastasize, it can also make it difficult to accurately predict drug concentrations that will pass the barrier to reach the tumors in the brain. Even some water-soluble drugs have been able to pass the BBB when normally they are incapable of doing so in a healthy person [16]. Some of these compounds include cisplatin and etoposide, which have been proven to be effective against metastases stemming from breast cancer [13]. In some cases where the drug may not be able to pass the BBB, a catheter may be surgically inserted for direct delivery to the brain [7].
Once the drug passes the BBB, it must still reach the tumor site to be effective. Transmembrane efflux pumps and high interstitial fluid pressures will affect the drug’s ability to reach the target [20]. Some experimental approaches have been tested to directly deliver the therapeutic to the tumor by using stereotactically placed catheters and hydrostatic pressure.
Current chemotherapeutic agents include cytotoxic drugs such as anthracyclines, taxanes, and 5-fluorouracil [10]. However, recent studies by Von Hoff et al. have found anthracycline to be associated with cardiac dysfunction21. Recently in 2010, epothilones and ixabepilone were implemented as new cytotoxic agents that are efficacious against metastatic breast cancer in patients that previously received anthracyclines and taxanes [10]. Other cytotoxic agents that have been shown to have activity against brain metastases include high-dose intravenous methotrexate and temozolomide [22]. Breast cancer metastases are best treated when considering the molecular subtype of the primary tumor. More aggressive subtypes like HER2- or triple negative cancers will respond well to temozolomide or capecitabine. Less aggressive subtypes like luminal A or luminal B breast cancer are more likely to respond better with hormonal therapy, so cytotoxic agents may not be the best choice for treatment [20].
It is possible that using primary tumors to predict susceptibility of brain metastases to chemotherapy is not the most reliable method. This is due to the possibility of the metastases mutating to have significant genetic differences from the original tumor, potentially causing them to be resistant to chemotherapy [16]. Chemotherapeutic options are best chosen when considering the primary tumor, as BBB penetration is a lesser concern if it is disrupted. When considering the nature of the primary tumor, it is important to consider not only the type of cancer and how aggressive it is, but also what the microenvironment of the tumor is. The process of cancer metastasizing to the brain requires the primary tumor to invade local tissue, which leads to malignant cells circulating throughout the bloodstream to reach further sites in the body [23]. This means that other normal organ-specific tissues and cells in the brain, such as stromal and immune cells, interact with the cancerous cells, creating a tumor microenvironment. The microenvironment of the cancer malignancies is what regulates the tumor’s biology and therefore it’s susceptibility to specific therapeutics.
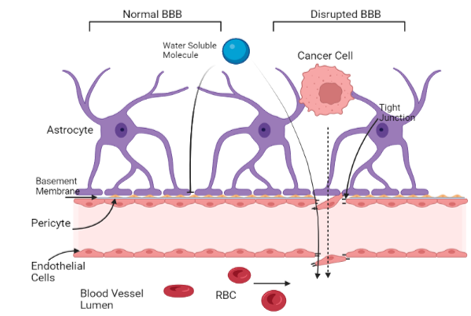
Figure 2. Malignant cancer cells alter the blood brain barrier to reach circulation in the vasculature of the brain. The disrupted BBB allows for more water-soluble molecules and cytotoxic agents to breach the barrier and reach the tumor site. [Adapted from “Breast Cancer to Brain Metastasis”, by BioRender.com (2022). Retrieved from https://app.biorender.com/biorender-templates]
Recent studies have also found that tumor-infiltrating lymphocytes can be used as a reliable and independent prediction of how the malignancies in the brain will respond to chemotherapy [23]. One study by Duchnowska et al. found that these lymphocytes were present in over 90% of breast cancer brain metastases [24]. This further strengthens the theory behind how cytotoxic agents are effective in the brain and can successfully treat metastatic tumors when the microenvironment of the primary tumor is considered.
Surgical Considerations
Surgical intervention is an approach used on patients that have few isolated and more easily accessible tumors. Tumors that produce clinical symptoms for the patient are also considered for surgical removal. Technological advances have minimized how invasive surgery may need to be to safely remove the tumor. Intraoperative imaging-guided neuro-navigation and brain mapping have allowed surgeons to safely remove tumors and resection where needed at even deeper and more delicate areas of the brain than previously possible.
In addition to imaging, advances in methods of tumor removal have advanced. Now, only a small burr hole through the skull is necessary instead of larger incisions, where a laser catheter is inserted for pinpoint stereotactic laser ablation or laser interstitial thermal therapy7. These techniques are useful for tumors that are not easily accessible or in patients who previously received radiation and have experienced toxicities associated with it. Other minimally invasive techniques involve a ‘keyhole’ approach, where the incision site is a fraction of what was previously used and only requires a small keyhole craniotomy20. These new advances minimize risk of exposure to infection, subsequently making recovery after surgery much faster with fewer side effects.
Surgery can be used as the primary treatment followed by other therapies or can be used after them if the tumor reaches a smaller size suitable for removal. When surgery is implemented following radiation therapy, patients are more likely to show improved symptoms and higher survival rates compared to patients who only receive radiation treatment. On the other hand, if surgical intervention is the primary treatment, patients will still need either radiation or chemotherapeutic treatment to eliminate potential remaining or circulating malignant cells [25]. A study performed by Patchell et al. showed that patients who received WBRT after initial surgical intervention had a significantly reduced recurrence rate from 46% to 10% [26].
Removal of the tumors also allows for better analysis of the genetic profile of the malignancies [20]. The histopathology of the malignancies may be studied and used to create a more personal therapeutic approach for the patient. This additional diagnostic method is beneficial since it may not only alleviate symptoms caused by the tumor, but it also provides insight into which therapy would be best suited for treatment on a molecular level.
The future of treatment for brain metastases from breast cancer is rapidly expanding in development of new approaches. Potential new pathways such as molecular targeted therapy, immune checkpoint therapy, or using novel targets for therapeutic drugs are closer to implementation with every clinical trial.

Emerging Approaches for Breast Cancer Metastasis to the Brain
Medical management of breast cancer brain metastasis (BCBM) is a challenging task and further compounded by the genetic heterogeneity of breast cancer (BC), which limits viable treatment options. The probability of developing a brain metastasis (BM) varies with the BC’s molecular expression pattern [27]. which is not always identical to cells of the metastatic tumor [27-29]. It is well established that patients with human epidermal growth factor receptor-2 positive (HER2+) and triple negative (TNBC) breast cancers are more likely to develop BCBMs compared to other subtypes [30]. Despite advances in our understanding of BC subtypes and their varying probabilities of metastasizing to the brain, current guidelines discourage MRI screening of asymptomatic BC patients for BMs [Lewin]. Screening for advanced disease is one of the earliest modifiable approaches to treating BC. There is a growing body of evidence that may support earlier BM imaging in patients with certain subtypes of BC, potentially at the time of their initial diagnosis if other metastases are present [3,31,32]. However, further evidence is needed to justify MRIs imaging based on tumor subtype, as MRIs are
expensive and expose patients to possibly unnecessary radiation.
Research has identified several potential biomarkers associated with BCBM, and their quantification may be a reliable indicator to assess the appropriateness of MRI imaging in BC patients with asymptomatic BM [33-35]. Beyond imaging, these biomarkers are increasingly being implicated in a wide array of diagnostic, prognostic, and therapeutic applications, constituting an exciting new realm of opportunity for the earlier detection and treatment of BCBM [36,37]. Circulating tumor cell (CTC)-specific nucleic acids, particularly single-stranded, noncoding RNA molecules known as microRNAs (miRNAs), have been the subject of several investigations looking for predictable molecular patterns in BC that could be used for earlier brain metastasis detection [38-40]. Other studies have examined differentially expressed genes between primary BC tumors and BCBMs; one bioinformatics study demonstrated critical involvement and prognostic value of the ANLN, BUB1, TTK, and SKA3 genes in the progression of BCBM [41]. A 2017 study found a long noncoding RNA (termed Lnc-BM) associated with enhanced progression of BCBM via overactivation of the tyrosine kinase JAK2 signaling pathway [36].
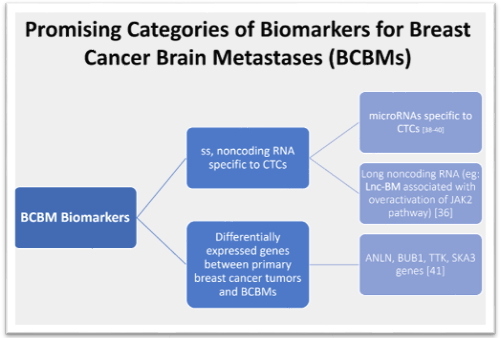
Figure 3: This figure shows the broad categories of potential biomarkers that are being further studied for therapeutic and prognostic use for BCBMs.
A long-standing barrier to treating BCBMs is the impermeability of the blood-brain barrier (BBB) to most drug therapies, which becomes the blood-tumor barrier (BTB) following metastasis [42]. The BBB acts as a physical and metabolic barrier between systemic circulation and the brain, and infiltration is a crucial step for circulating tumor cells to establish a metastatic lesion in the brain. This is a complex and multistep process that has been well described, although significant unknowns remain [43,44]. The previous belief that the BBB was completely impermeable led to the exclusion of BC patients with BMs from clinical trials for many years, resulting in a knowledge gap in the treatment of BCBMs. The composition of the BBB and later BTB have since been examined, and a 2016 study identified desmin-overexpressing pericytes and laminin alpha-2 as potential targets to alter permeability [45]. Some later studies of xenograft mouse models reported success in coupling chemotherapeutics with novel therapies aimed at manipulating the BTB’s permeability to increase the available concentration of the drug in the brain [46,47]. Other drugs designed specifically to penetrate the BBB have demonstrated promise in treating BCBMs [48]. Drugs aimed at preserving the integrity of the BBB by inhibiting its interactions with CTCs are a promising model for preventing metastasis to the brain altogether.
Discoveries about the BTB and differential expression patterns of BCBMs have resulted in numerous avenues to develop novel therapies, as well as improve upon pre-existing ones. The monoclonal antibody trastuzumab has been a longstanding treatment option for HER2+ metastatic breast cancer, but its capacity to cross the BBB alone is poor [49,50]. Antibody-drug conjugates like trastuzumab deruxtecan (T-DXd) have demonstrated increased efficacy and enhanced patient outcomes [51]. Other targeted therapy options for HER2+ BCBM have appeared over the years, far outpacing the number of available treatments for the TNBC BM subtype. Research studies examining the efficacy of novel therapies in patients with TNBC BM are urgently needed, as this subtype has the worst overall prognosis.
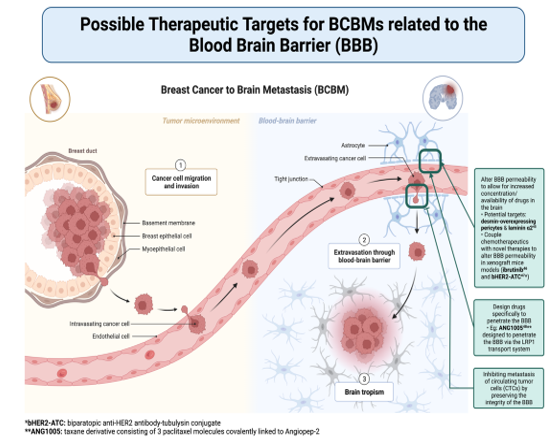
Figure 4: Figure 4. This figure shows a general overview schematic of how breast cancer can metastasize to the brain. It further highlights broad categories of therapeutic targets for BCBMs based on the role of the blood-brain barrier in metastasis. [Adapted from “Breast Cancer to Brain Metastasis”, by BioRender.com (2022). Retrieved from https://app.biorender.com/biorender-templates]
Breast cancer brain metastasis (BCBM) continues to contribute towards the poor prognosis for many patients with breast cancer. However, the further understanding and identification of the pathologic progression along with advancement in more-precisely targeted therapeutic modalities offer a gateway for improved outcomes in this population as well. Local therapies such as surgery and radiotherapy are becoming less invasive, which allows for improved outcomes by improving retention of cognitive function and hence patient quality of life. With new treatment trials seeking to examine the survival benefit in these individuals as well, immunotherapy and newer drug delivery systems (nanoparticles) may enable enhanced therapeutic efficacy. Numerous clinical trials are now underway and are anticipated to improve patient survival in the future for those who have BCBMs. Additionally, gathering more information on the receptor status and genomic profiling of the brain metastasis may be beneficial in identifying potential novel therapeutic targets for patients with treatment resistant BCBMs and would facilitate personalized therapy. Further research on various molecular processes, including as lncRNA, miRNA, and ctDNA, have recently been understood in the context of BCBM environment and are currently being explored to discover effective therapeutic targets as we understand the significance of the roles that they play in improving future diagnosis and treatment.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
