
Case Report | DOI: https://doi.org/10.31579/2690-8808/258
1 Faculty of Medicine and Pharmacy of Laayoune, Ibnou Zohr Agadir University. Laayoune-Morocco.
2 Faculty of Medicine and Pharmacy of Guelmim - Ibnou Zohr Agadir University. Guelmim- Morocco.
*Corresponding Author: Imane Boujguenna, Faculty of Medicine and Pharmacy of Guelmim - Ibnou Zohr Agadir University. Guelmim- Morocco.
Citation: Abbas Riyad, Ghita El Baroudi, Imane Boujguenna, (2025), Inguino-Ureteral Hernia: A Rare Diagnostic Challenge, J, Clinical Case Reports and Studies, 6(5); DOI:10.31579/2690-8808/258
Copyright: ©, 2025, Imane Boujguenna. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 26 May 2025 | Accepted: 03 June 2025 | Published: 10 June 2025
Keywords: hernia; ureter; extraperitoneal; paraperitoneal
Inguino-ureteral hernia is an extremely rare condition that is difficult to diagnose and often identified intraoperatively. There are two anatomopathological types: extraperitoneal and paraperitoneal. When symptomatic, treatment is based on relieving the obstruction, either endoscopically or surgically.
We report the case of a 73-year-old male patient admitted to the emergency department for right renal colic. Clinical examination revealed a strangulated right inguinoscrotal hernia. Contrast-enhanced abdominal CT scan showed the aforementioned hernia along with mild ureterohydronephrosis, likely due to ureteral entrapment within the hernia. Surgical management consisted of the reduction of the herniated viscera, including the ureter, followed by hernia repair using the Lichtenstein technique.
Our aim is to shed light on this under-recognized entity and to recommend cross-sectional imaging when upper urinary tract symptoms are associated with an inguinal hernia.
An inguinal hernia is defined as the protrusion of part of the abdominal organs through a natural area of weakness. Commonly herniated structures include the omentum, small intestine, appendix, and colon. In contrast, the ureter is very rarely found within a hernia sac. This unusual situation can be perplexing for clinicians and should be suspected and investigated whenever upper urinary tract symptoms are associated with an inguinal hernia
A 73-year-old male patient with a history of type II diabetes managed with insulin was admitted to the emergency department for a first episode of right-sided non-obstructive renal colic. Clinical examination revealed a conscious and hemodynamically stable patient with tenderness in the right lumbar fossa, abdominal distension, and a strangulated-appearing right inguinoscrotal hernia. Laboratory tests were unremarkable.
A contrast-enhanced abdominopelvic CT scan was performed, revealing mild small bowel distension upstream of a right inguinal hernia with signs of mild ureterohydronephrosis, likely due to intra-hernial ureteral entrapment.
Given the digestive emergency, the patient was taken to the operating room. Under spinal anaesthesia, a right low inguinal incision was made. Surgical exploration revealed a strangulated right indirect inguinoscrotal hernia containing suffering but viable small bowel. Notably, the ureter was identified on the posterolateral aspect of the hernia sac, confirming a diagnosis of paraperitoneal inguino-ureteral hernia (Figure 1).
The surgical procedure involved reduction of the herniated contents, careful repositioning and reduction of the ureter, and hernia repair using the Lichtenstein technique with No. 3 round needle mersuture.
Postoperative recovery was uneventful, with resolution of right flank pain. The patient was discharged on postoperative day 3.
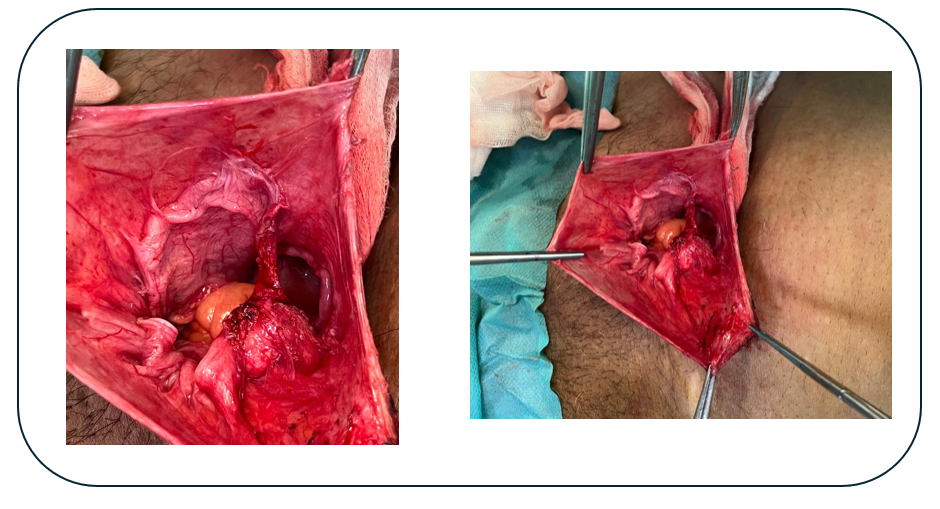
Figure 1: Intraoperative view of the inguino-ureteral hernia showing the stretched ureter adherent to the hernia sac.
The ureter can be found in various hernial orifices, including inguinal, femoral, sciatic, and even diaphragmatic openings [1]. This is a rare condition, with only about 150 cases reported up to 2017 [2]. The first known case was discovered during autopsy by Leroux in 1880, followed by the first intraoperative identification by Reichel and the first preoperative diagnosis by Doumarshkin in 1937 [3].
Two anatomopathological types of inguino-ureteral hernias have been described. The paraperitoneal type, accounting for 80% of cases, involves stretching of the ureter, which adheres to the posterolateral portion of the hernia sac [4]. In 20% of cases, the extraperitoneal type is present, where retroperitoneal fat slides into the hernia, dragging the ureter and spermatic cord with it, without a true hernia sac [5]. In 80% of cases, inguino-ureteral hernias are indirect inguinal hernias [6].
Clinically, this condition typically presents as renal colic and, if left untreated, can progress to sepsis [7]. Preoperative diagnosis is crucial to avoid surgical complications due to unawareness of this entity. Diagnosis is based on clinical suspicion and imaging, especially abdominal CT scanning.
The surgical approach should be conservative, and the procedure may be performed via laparotomy (the traditional approach), laparoscopy, or, more recently, robotic surgery [2,8]. Treatment consists of surgical repositioning of the ureter, provided there is no irreversible damage [5]. In some cases, ureteral reconstruction is necessary, involving segmental resection and end-to-end anastomosis or ureterovesical reimplantation [9].
Although extremely rare, the association of urinary symptoms with an inguinal hernia should raise suspicion for an inguino-ureteral hernia. Recognizing this condition preoperatively is essential to avoid unexpected findings and complications during surgical repair.
To anyone who has participated in the care of this patient directly or indirectly
None declared.
No funding sources
ethics approval was not required for this study
"Written informed consent was obtained from the patient for publication of this case report and any accompanying images".
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
