
Research Article | DOI: https://doi.org/10.31579/2578-8868/349
1 Faculty of Computer Science, Professorship of Business Information Systems, especially Multimedia Market-ing, Schmalkalden University of Applied Sciences, Germany
2 COVID-19 Aftercare Center with Training Outpatient Clinic and Training Center for Internet and Mobile-Based Intervention (IMI) the Brandenburg Technical University Cottbus-Senftenberg (BTU), Institute for Medical Informatics, Germany
3 Brandenburg University of Technology Cottbus-Senftenberg, Institute of Medical Technology, Germany
*Corresponding Author: Thomas Urban, Faculty of Computer Science, Professorship of Business Information Systems, especially Multimedia Marketing, Schmalkalden University of Applied Sciences, Germany.
Citation: Thomas Urban, Peter Lohse, Fritjof Reinhardt, (2025), Influence of Post-COVID-19 and a doctor-led Blended Therapy on health behavior and the health action of patients, J. Neuroscience and Neurological Surgery, 17(1); DOI: 10.31579/2578-8868/349
Copyright: ©, 2025, Thomas Urban. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 06 December 2024 | Accepted: 18 December 2024 | Published: 06 January 2025
Keywords: Post-COVID-19 syndrome, fatigue, blended therapy, health action, health psychology
Background: With the SARS-CoV-2 pandemic and the possibility of developing Post-COVID-19 syndrome, health issues have become more dominant. Post-COVID-19, stress reactions of a somatic, cognitive and emotional nature triggered by performance requirements often occur even with low objective stress. As part of an intervention and observation study, stress-controlled standardized training therapy and intensified cognitive behavioral therapy in the form of blended therapy were implemented at the Post-COVID-19 Center (PCZ) Lausitz (Senftenberg) for patients with the leading syndromes fatigue and sensorimotor instability. From this, parame-ters influencing the individual phase-specific health behavior of the patient were derived.
Materials and Methods: The aim was to derive an explanation and prediction of health behavior and to find ways of influencing patients' health actions by doctors and therapists to alleviate symptoms and avoid chronicity of the Post-COVID-19 key symptoms of fatigue and sensorimotor instability. For this purpose, the Health Action Process Approach (HAPA)-model, which has a high level of resonance in health psychology, was used. The HAPA-model was specified with the results of a guide-line-supported expert interview that took place in the form of an observational study in Q3-2023 and Q4-2023 with 46 patients from a previous blended therapy interven-tion study (78 patients) on post-COVID-19 Center (PCZ) Lausitz (Senftenberg).
Results: Factors influencing the motivational and volitional phase of health action for post-COVID-19 patients with fatigue and sensorymotor instability were derived. To this end, five specific research questions were answered using a guided expert interview and the results were integrated into the Health Action Process Approach (HAPA)-model. The specified HAPA model also provides doctors and therapists with recommendations for action in order to positively influence therapy behavior in a phase-specific manner and thus also the outcome.
Conclusion: The specified Health Action Process Approach (HAPA)-model for Post-COVID-19 patients with fatigue and sensorimotor instability allows for the representation of intervention-specific influencing factors on the health behavior and health-related actions of patients. This gives doctors and therapists the opportunity to shape patients' therapeutic behavior in a positive way.
Since the beginning of the SARS-CoV-2 pandemic, by the end of November 2024, over 770 million people worldwide have been infected with an immunogenic virus [33], which causes (long-term) health consequences of varying severity and duration (Figure. 1). Following a SARS-CoV-2 infection, similar to other infectious diseases, persistent symptoms can occur in various organ systems (lungs, heart, brain, gastro-enterone and other secondary organs) and/or different new symptoms can arise that persist over a longer period of time [9, 19, 30, 31].
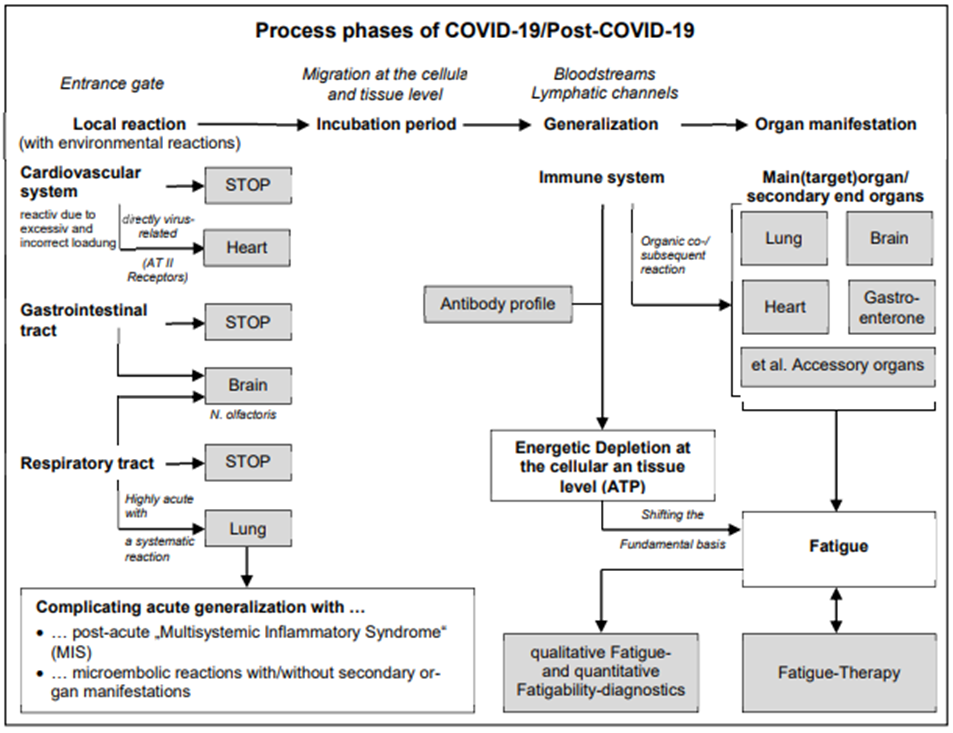
Figure. 1: Process phases COVID-19/Post-COVID-19
In the specialist literature, the term Post-COVID-19 syndrome (PCS) has become established for symptoms that occur or persist twelve weeks after a SARS-CoV-2 infection [2, 3, 4]. The frequency of occurrence of PCS is between 10 and 35%. Using the Delphi consensus method, the WHO defined PCS as follows [22, 31, 34]:
In patients with Post-COVID-19, the stress reactions of a somatic, cognitive and emotional nature, which are often triggered by performance demands even at low objective stress, the extent of which is often not foreseeable in advance for the person affected (crash or post-exertional malaise: PEM), influence on individual health behavior. Health behavior is the subject of health psychology and can be discussed from different perspectives. The pathogenesis perspective looks at behavior to prevent disease and focuses more on avoiding risk factors [26, 27]. The focus of salute genesis is on promoting health. It also includes all health-related behaviors in the sense of preventative health behavior, such as a healthy diet or medical checkups [11, 24]. SCHWARZER defines health behavior as a preventative lifestyle that prevents damage, improves fitness and helps to extend life expectancy [29]. KASL and COBB also address the preventive intention in the definition of health behavior as “that activity of a person who feels healthy that is intended to prevent illnesses or to detect them in a phase that is not yet symptomatic” [16]. FALTENMEIER points out that there is not only expert knowledge of doctors or other specialists on health behavior, but also lay knowledge among the population that maintains behavior for health [11].
Health psychology as well as social science health research are concerned with the investigation of conditions and factors influencing health behavior. As can be seen in Table 1, a distinction is essentially made between two model groups: Linear models (motivational models and volitional models) Stage models (pure stage models and integrated models) [14].
The group of linear models assumes that a person's health promoting behavior is influenced by certain influencing factors (e.g. attitude, motivation, behavior). Most linear models are motivational and consider how individuals develop the intention to behave in a more health-conscious manner. Risk communication (e.g. fear appeals about the consequences of a SARS-CoV-2 infection) is intended to motivate recipients to adopt healthier behavior (e.g. hand hygiene, keeping their distance, wearing a face mask). Volitional models, on the other hand, depict the processes responsible for an individual (not) putting an intention into action [20, 21, 29].
Stage models are based on the assumption that an intended health-conscious action goes through several chronological stages that differ qualitatively. The social-cognitive phase model of health action, the Health Action Process Approach (HAPA)-model, differentiates between the motivation and the volition phase (implementation phase) and brings both aspects together in a dynamic stage model. The motivational phase distinguishes between three self-beliefs: the risk perception, the action result and the self-efficacy expectation. The stronger these self-beliefs are, the higher the motivation for health. Within the volitional phase, the concrete planning, execution and maintenance of the desired behavior is considered [18, 29].
| Models of health behavior | |||
| Linear Model | Stage Models | ||
| Health Belief Model (HBM) | Precaution Adoption Process-Model (PAPM) | Health Action Process Approach (HAPA) | Transtheoretical Model (TTM) |
|
|
|
|
Table 1: Models of health behavior [11, 14, 24, 29]
To explain and predict the health behavior of the patient group under consideration, the Health Action Process Approach (HAPA) model is used based on the following characteristics [11, 14, 26]:
The specification of the Health Action Process Approach (HAPA)-model was based on an observation study carried out in Q3-2023 and Q4-2023 at the Post-COVID-19 Center (PCZ) Lausitz (Senftenberg) with a guideline-supported expert interview. Patients who had carried out stress-controlled training therapy in the form of blended therapy to treat the leading syndromes “fatigue” and “sensorimotor instability” at the PCZ during the period from Q1-2021-Q2-2023 as part of an intervention study took part.
In the PCZ, a monocentric stress-controlled training therapy in the form of a blended therapy (analog and digital intervention) was implemented to treat the key syndromes “fatigue” and “sensorimotor instability”. At the same time, a secondary psychosomatic treatment need that often arises in the Post-COVID-19 course with fatigue was carried out with an intervention study and observational study from Q1-2021 to Q2-2024. As part of blended therapy, digital intervention options were used to supplement analogue forms of therapy [1]. The combination of analog and digital forms of therapy achieves a high degree of flexibility in therapy design as well as better patient adherence [7, 8, 10]. Furthermore, patient groups with little mobility or at great geographical distances can be reached, service providers can be integrated at a central and peripheral level, and the patient's treatment plan can be coordinated through shared data use.
In Q3-2023 and Q4-2023, a guide-based expert interview was carried out to evaluate the influence of the Post-COVID-19-disease and blended therapy on the health behavior of patients. Of the participants from the blended therapy (78 patients, with M = 37, W = 41), 46 study participants (M = 22; W = 24) were willing to take part in the guideline-based expert interview.
Methodological framework of the guideline-supported expert interview
A qualitative, guideline-supported expert interview represents a systematic and theory driven process of data collection by interviewing people with exclusive knowledge [Kaiser 2014]. As an expert, the specific role of the interview partner is seen as a source of specialized knowledge [13]. The patients received this knowledge through stress-controlled training therapy and, if necessary, intensive cognitive behavioral therapy.
The behavior of patients during therapy is determined by various influencing factors [17]:
Research questions of the guideline-supported expert interview
With the guide-supported expert interview, information on health behavior in the context of stress-controlled multimodal blended therapy was generated using five specific research questions that would otherwise not be obtainable [15]. The interview structure followed the standard structure of opening/warm-up questions, main part and conclusion with thanks [23]. The aim was to derive factors influencing health behavior in the motivation and volition phase of health action for Post-COVID-19-patients with fatigue and sensory motor instability. These factors were then integrated into the Health Action Process Approach (HAPA)-model. The result presents possibilities for doctors and therapists to influence health behavior.
The following five specific research questions were answered with the guide-supported expert interview:
The results of the guideline-supported expert interview were integrated into the Health Action Process Approach (HAPA)-model to explain health-promoting and health-damaging behaviors. As can be seen in Fig. 2, the trusting doctor-therapist-patient relationship as well as a central contact person or guide for all topics of the recovery process form the bracket around the motivational and volitional phase. From the expert interview, the following key points for establishing and maintaining a trusting doctor-therapist-patient relationship can be summarized:
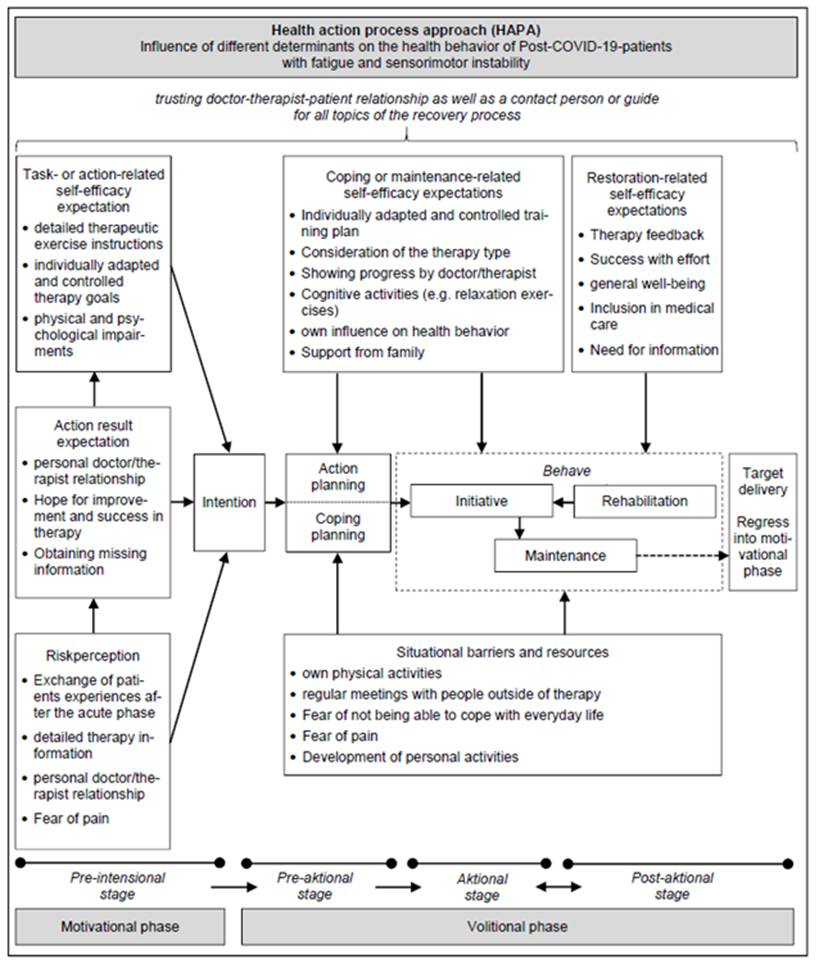
Figure 2: Health action process approach (HAPA)-model specified for Post-COVID-19-Patients with fatigue and sensorimotor instability; Own representation, based on [14, 20, 25, 29]
Motivational phase
In the motivational phase, the respective factors influencing risk perception, action outcome expectations and self-efficacy expectations of patients with post-COVID-19 as well as fatigue and sensorimotor instability are summarized. Risk perception includes the individual perception and subjective assessment of the severity of the disease as well as one's own vulnerability [6, 9]. The following parameters can be identified from the interviews, which are incorporated into the individual risk as-sessment:
In order for blended therapy to be implemented, behavioral-/action alternatives must be known to reduce perceived risks. Action outcome expectations are the most important beliefs, since the presence of alternatives with the weighing of the pros and cons is a necessary condition for behavior change. The following components influence this:
Perceived self-efficacy is the patient's subjective belief that they can carry out new behaviors based on their existing competence. The following moderating variables influence self-efficacy in the pre-intentional stage:
The individual assessment of risk perception, expected action results and self-efficacy expectations flow into the patient's goal intention and complete the pre-intentional stage. The stronger this intention is, the more likely it is that behavioral changes will occur in the sense of a quick start to the stress-controlled training therapy [14, 29].
Volitional phase
The volitional phase begins with action and coping planning, where the patient decides on the framework conditions for the desired behavior. In the pre-actional stage, this concerns the planning of the start and the regular implementation of the stress-controlled training therapy (when, where and how), but also the development of personal activities [14, 26]. As can be seen in Fig. 2, the following points influence self-efficacy expectations and thus action planning and subsequent therapy behavior:
Coping planning and therapy behavior are influenced by situational barriers and resources. This concerns:
In the actional stage, therapy is carried out and maintained. The extent of self-efficacy expectations affects the intensity and persistence of goal pursuit. Optimistic attitudes promote persistent goal pursuit even in the face of setbacks (e.g. being ex-hausted by successes with effort). In the therapy implementation phase, there is a constant monitoring of the execution of actions in the sense of recovery-related self-efficacy expectations, which is guided by the following points:
In the final post-actional phase, the patient evaluates the action in terms of the success/failure of the therapy. In order to be successful in the volitional phase, the treatment plans must therefore be planned constructively together with the doctor/therapist in order to set achievable goals, create rewards as success and regulate unpleasant emotions (e.g. depressive and helpless moods).
A possible disengagement, i.e. the therapy is discontinued, can be due to a lack of volitional strength and indicate self-regulation errors. It is simply not possible to change the patient's health behavior.
The COVID-19-pandemic has shown that medical management functions stably, even with a large number of patients, if it can rely on established structures that are stably networked in routine operations. For example, specific treatment resources were available for stroke care in Germany, which linked the medical practice with the local university structures and could be used immediately for pandemic care. This was the reason for the initially implemented monocentric design of the intervention study. This must be seen as a limitation for the overall conclusion of the study.
As part of the implemented intervention and observation study, it has been shown that in patients with Post-COVID-19, on the one hand, the stress reactions of a somatic, cognitive and emotional nature, which are often triggered by performance requirements even at low objective stress, have an influence on health behavior. On the other hand, the exercise-controlled blended therapy helps to positively influence the recovery process and thus also health-related actions.
The digital interventions integrated into blended therapy in the form of a computer-supported training system and a mobile application support physical health. They improve the ability to maintain everyday activities and are independent of the location and time of the provision of analogue therapies by medical providers. At the same time, they prove to be particularly effective in dealing with fatigue symptoms. In order to increase adherence and effect strength among patients, digital therapy of-fers must be individually tailored to patients and their symptoms [5, 6, 20, 22, 28, 32].
With the results of the guideline-supported expert interview, the Health Action Process Approach (HAPA) model was specified for post-COVID-19 patients with fatigue and sensorimotor instability. The basis for health-promoting action is a trusting doctor-therapist-patient relationship.
The motivational phase with the individual assessment of risk perception, the expec-tation of action results and the expectation of self-efficacy is primarily influenced by the opportunities for exchange with other patients after the acute phase of COVID-19, the hope for improvement and success in therapy as well as the implementation of individually tailored and controlled therapy goals. In particular, a controlled implementation of the therapy goals through stress control during training therapy is necessary so that patients do not get into a crash situation and thus possibly end the therapy prematurely.
In the volitional phase it became apparent that at the beginning of therapy, self-efficacy expectations in the form of one's own ability to influence one's state of health, the stress-controlled training plan or support from families determine behavior. Patients' situational barriers and resources, such as fear of pain, personal activities or social contacts, affect coping planning and therapy behavior. Strong communicative interactions with the doctor/therapist, success through the efforts in therapy or general well-being during training therapy characterize the actional stage. Here the patient compares his expectations of self-efficacy in the blended therapy with the results of the individual recovery process. Goals that are only achievable and planned together with the doctor/therapist do not lead to an exit from therapy. The results of the guideline-supported expert interview were also used to derive recommendations for doctors and therapists in order to positively influence the therapy behavior and thus the outcome of the patients.
All authors declare that they have no conflict of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
