
Case Report | DOI: https://doi.org/10.31579/2690-4861/153
1Department of Radiology, Apollo Hospitals International Limited, Ahmedabad, Gujarat, India.
2Department of Surgical Oncology, Apollo Hospitals International Limited & Apollo Comprehensive Blood & Cancer Center, Ahmedabad, Gujarat, India.
*Corresponding Author: Jitendra Parmar, Department of Radiology, Apollo Hospitals International Limited, Ahmedabad, India.
Citation: J Parmar, A Zope, T Patel, S Choudhary, B Angirish. (2021). Inflammatory Breast Carcinoma in a Pre-existing Mammary Hamartoma: A rare case report and Review of Literature. International Journal of Clinical Case Reports and Reviews. 8(3); DOI:10.31579/2690-4861/153
Copyright: © 2021 Jitendra Parmar, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 30 June 2021 | Accepted: 01 September 2021 | Published: 07 September 2021
Keywords: breast; mammary hamartoma; inflammatory breast carcinoma; mammography
Mammary hamartoma is uncommon typically non-malignant benign breast lesion, comprising varying amounts of fatty, fibrous connective tissue and glandular elements. The co-existence of hamartomas and malignancy is very rare and it has no special propensity to undergo malignant transformation. We present a case report of a 66-year-old patient diagnosed with Inflammatory Breast Carcinoma within a previously diagnosed mammary hamartoma in the right breast. The comprehensive work-up with mammography, ultrasound, Positron Emission Tomography – Computed Tomography (PET-CT) and ultrasound-guided biopsy confirmed invasive ductal carcinoma within the hamartoma. Although malignancy arising within hamartoma is an extremely rare entity, the radiologist should be aware and prudent of the atypical as well as suspicious features within hamartoma during interpretation of imaging modalities and should thoroughly investigate any architectural distortion or microcalcifications within an otherwise typical hamartoma. No case has been reported for inflammatory breast carcinoma in mammary hamartoma as per our best of knowledge.
Mammary hamartoma, also known as fibroadenolipoma is uncommon typically non-malignant benign breast lesion, comprising varying amounts of fatty, fibrous connective tissue and glandular elements. The first reported case of mammary hamartoma was in 1971 by Arrigoni et al. who described it as a well circumscribed lesions comprising varying amount of benign fat and fibro glandular tissue [1]. The typical benign features are described subsequently on mammography [2], ultrasound [3], and MRI [4]. The co-existence of hamartomas and malignancy is very rare and it has no special propensity to undergo malignant transformation. Very few cases of malignancy in mammary hamartoma have been reported previously in the literature [5-9]. No case has been reported for inflammatory breast carcinoma in mammary hamartoma as per our best of knowledge.
We present a case report of a 66-year-old patient diagnosed with Inflammatory Breast Carcinoma within a previously diagnosed mammary hamartoma in the right breast. The comprehensive work up with mammography, ultrasound, Positron Emission Tomography – Computed Tomography (PET-CT) and ultrasound-guided biopsy confirmed invasive ductal carcinoma within the hamartoma. This case report illustrates the importance of atypical and suspicious radiological findings in otherwise typical hamartoma that may help in the diagnosis of malignancy.
A 66-year-old female patient was presented in our outpatient department with history of increase in the size of previously documented lump in right breast for 10-15 days. The patient had a history of swelling in right breast for 20 years, and it was diagnosed as hamartoma on previous ultrasound and mammography. The patient was non-alcoholic and non-smoker. The patient was hypertensive and had history of ischemic heart disease and hypothyroidism. The patient had a positive family history for breast cancer in three siblings and one sister with no history of breast cancer died of non-cancerous pathology at 35 years of age. Clinically the right breast was red and swollen with diffuse erythema and edema (peau d’orange) involving more than a third of the skin of the breast with retraction of nipple. However, the breast was non-tender. Two lymph nodes were palpable in right axillary region and they were hard.
Based on her present history & positive family history as well as clinical examination, she was referred to radiology department for mammography and ultrasound to rule out malignancy.
Mammography was performed with standard Mediolateral Oblique (MLO) and Cranio-Caudal (CC) view and supplemented with spot magnification view of mass and microcalcifications (Figure 1). It revealed overall increase in density and trabecular thickening of right breast with architectural distortion and diffuse skin thickening as well as mild nipple retraction. A well-circumscribed lesion, showing mixed fibro-glandular tissue was seen in right breast, which was giving breast within breast appearance, suggestive of hamartoma. In addition to hamartoma, an ill-defined iso to high density lesion with indistinct margins and mild architectural distortion was also seen within the hamartoma. Moreover, multiple fine pleomorphic microcalcifications were seen in segmental distribution in outer lower quadrant within the hamartoma on spot magnification view. Enlarged dense lymph nodes with loss of fatty hilum were present in right axillary region.

On ultrasound (Figure 2), a well-defined and well-circumscribed area of fibro-glandular tissue same as rest of breast parenchyma was seen in outer quadrant of right breast (Figure 3A). Within this area, poorly appreciated, an ill-defined hypoechoic lesion was noted, which was associated with architectural distortion (Figure 3B), and diffuse overlying skin thickening involving more than 1/3rd of breast. Two well-defined sub-centimeter sized skin nodules were also noted in lower outer quadrant. Few enlarged round and oval shaped hypoechoic lymph nodes were also present in right axillary and infra-clavicular region.
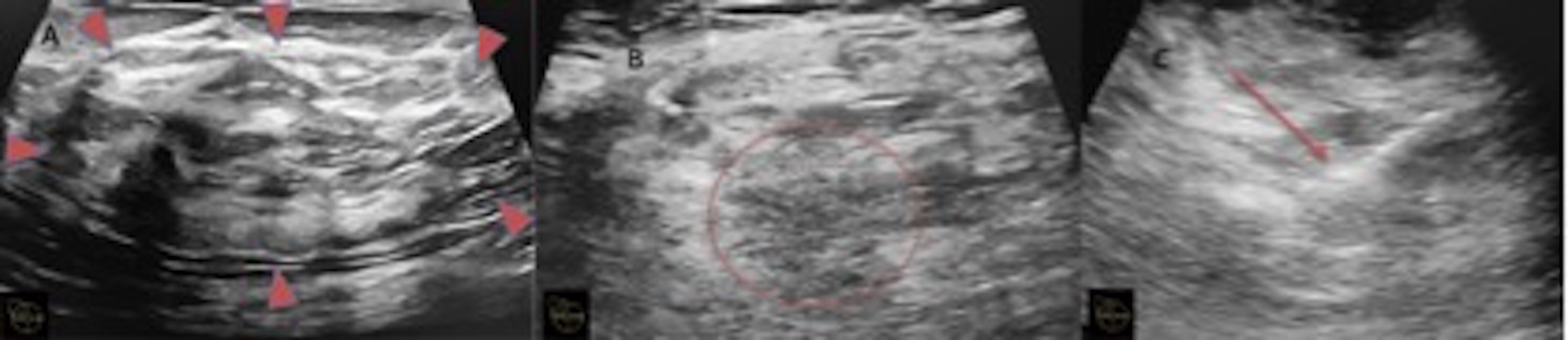
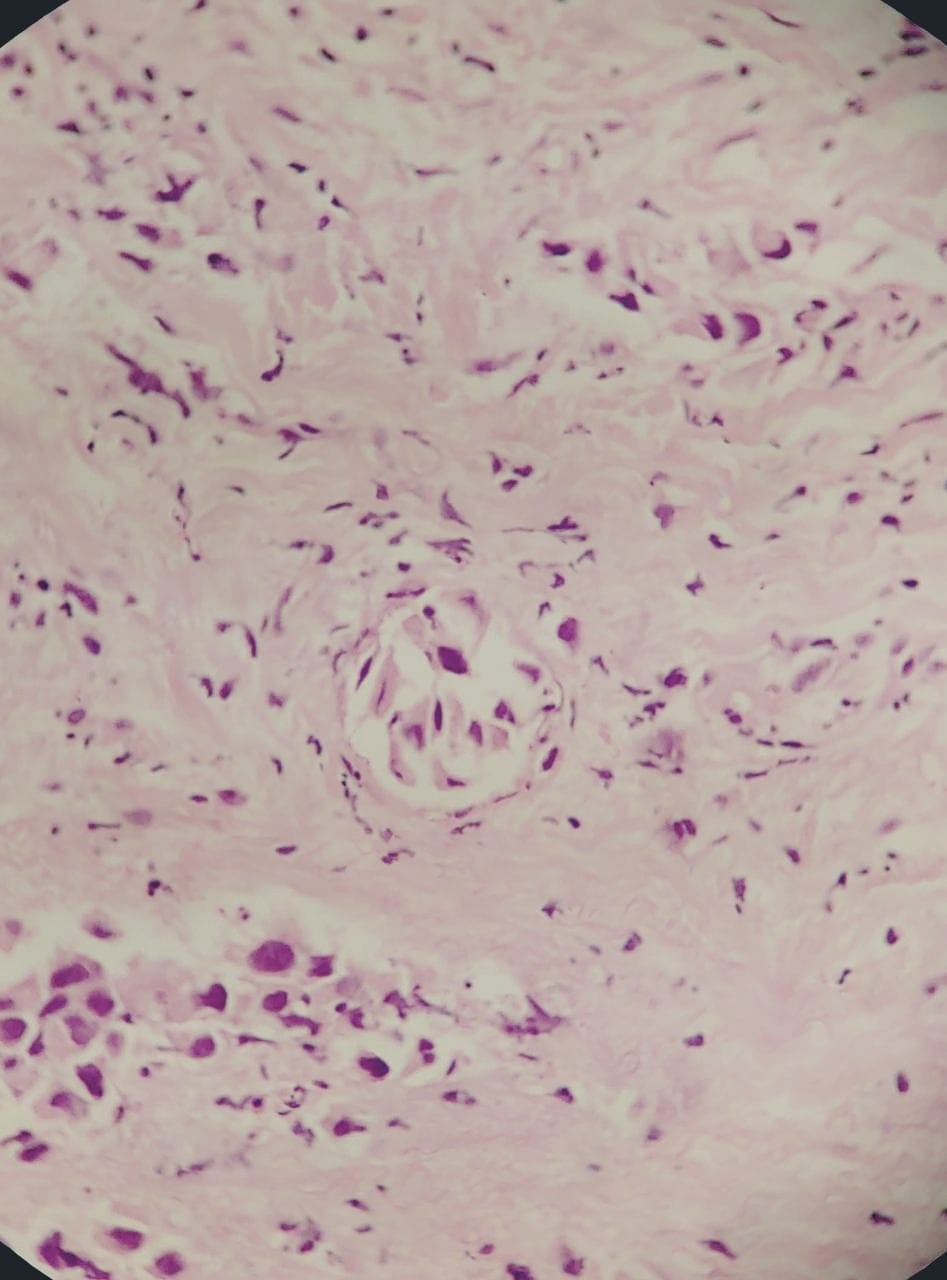
Based on clinical, mammography and ultrasonography findings, the patient was classified as Inflammatory Breast Carcinoma, Breast Imaging Reporting and Data System (BI-RADS) V. The patient underwent ultrasound guided tru-cut biopsy (Figure 3C) for grading characterization and immunohistochemical markers. On histopathology (Figure 4), the patient was confirmed with invasive ductal carcinoma of histological grade III and was negative for Estrogen, Progesterone and Human Epidermal Growth Factor Receptor 2 (HER2) immunohistochemical markers.
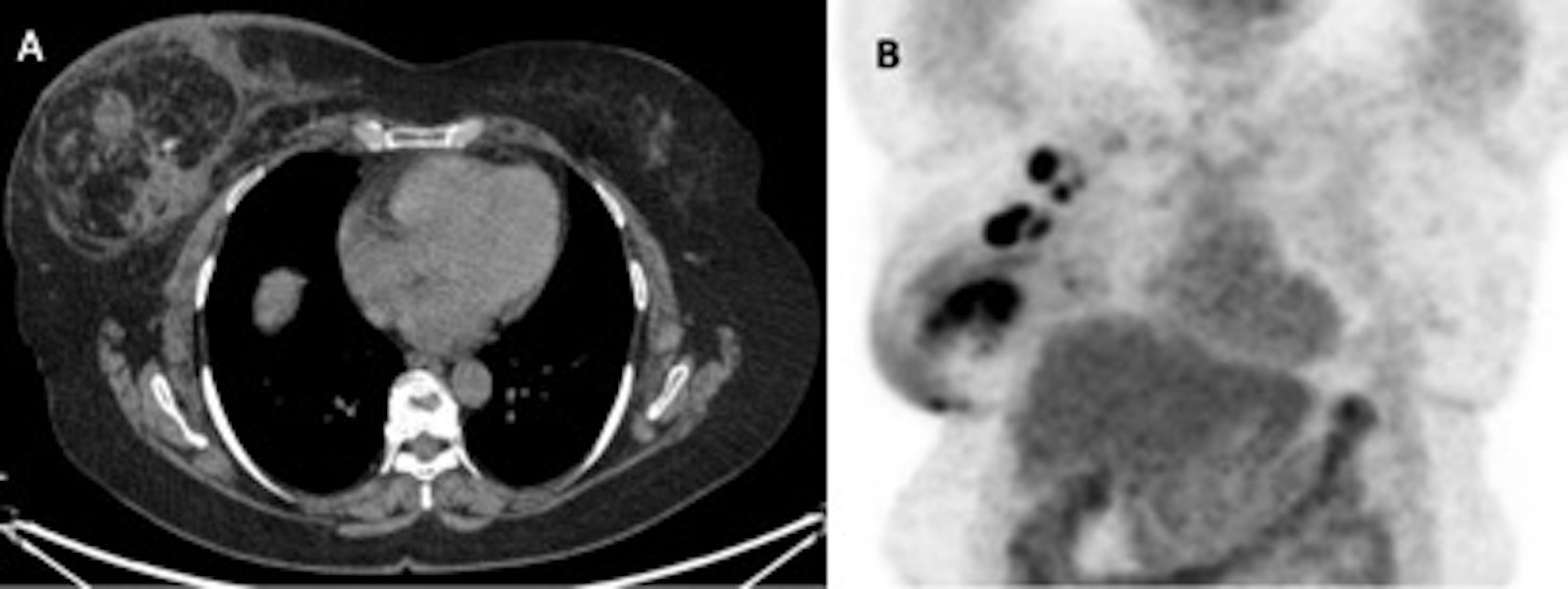
PET-CT (Figure 3) was done for staging, which shows mild increased uptake in entire right breast (as compared to left breast) with diffuse overlying skin thickening (more than 1/3rd of the skin of the breast) and nipple retraction. It also confirmed a well-defined encapsulated fibro glandular tissue same as breast with classical appearance of “Breast within Breast”, suggestive of breast hamartoma (Figure 3A). Within this lesion, two heterogeneously enhancing hyper-metabolic soft tissue lesions were noted, measuring 4.2 x 3.8 x 2.1 cm and 4.1 x 2.9 x 2.5 cm showing intense Fluorodeoxyglucose (FDG) uptake with the maximum standardized uptake value (SUVmax) of 12.8. Two hypermetabolic skin nodules were also confirmed. Few heterogeneously enhancing hypermetabolic lymph nodes were present in right axilla at level I, II and IIIa (Figure 3B). The clinical Tumor-Node-Metastasis (cTNM) scoring system classified as cT4 (m) N3M0 (m-modifier), that corresponds to stage IIIc according to 8th edition of American Joint Committee on Cancer (AJCC) staging system. The patient refused for genetic testing for Breast Cancer gene 1 and 2 (BRCA1, and BRCA2) for hereditary breast and ovarian cancer in spite of genetic counselling. The case was discussed in multidisciplinary meeting and advised to have neoadjuvant chemotherapy (Docetaxel, Anthracycline and Cyclophosphamide) for 6 cycles followed by surgery and radiation if required.
Arrigoni et al. reported mammary hamartoma first time in 1971 as a well circumscribed lesions comprising varying amount of benign fat and fibro glandular tissue [1]. He described a classical mammographic findings of a well circumscribed lesion comprising soft tissue density and fat surrounded by a pseudo capsule, which gives a “breast within a breast” or a “cut sausage” appearance [1,2]. Mammary hamartomas are well circumscribed, ‘wider than tall’ lesions with mixed echogenic internal echotexture without any microcalcifications or retro tumour acoustic shadowing on ultrasonography [3]. On Magnetic Resonance Imaging (MRI), a hamartoma is an encapsulated mass with mixed fat and fibro-glandular signal intensity with some contrast enhancement of fibro-glandular elements [4].
The incidence of malignancy within hamartomas is extremely rare. Very few case reports have described different types of malignancy including both invasive and non-invasive malignancies arising within hamartomas [5-9]. Therefore, the finding of breast hamartoma does not completely exclude the possibility of malignancy originating from benign lesion. Forte et al. in 2019 described invasive carcinoma arising from hamartoma or fibroadenolipoma [9]. Most of the reported cases were of invasive ductal carcinoma as in our case, however, few cases were also of lobular carcinoma and in situ carcinoma [7].
We are in agreement with Lee et al [10]. That any lesion that grows, or shows radiologic features atypical for a hamartoma, a histopathological diagnosis should be warranted. Atypical radiological features, which should raise suspicion of possible malignancy developing within hamartoma, includes suspicious additional mass that shows discriminating imaging features from the hamartoma or development of microcalcifications or increase in size of the mass during follow up.
In conclusion, although malignancy arising within hamartoma is an extremely rare entity, the radiologist should be aware and prudent of the atypical as well as suspicious features within hamartoma during interpretation of imaging modalities and should thoroughly investigate any architectural distortion or microcalcifications within an otherwise typical hamartoma.
We are very thankful of the medical oncology department and patient for their unconditional help while preparing this manuscript.
This case report did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
The authors declare that they have no competing interests and all authors have approved the manuscript for submission.
The content of the manuscript has not been published or submitted for publication elsewhere.
The patient reported had signed a written informed consent form, in which the patient was informed that they may be subjects of scientific publication and is informed of the ethical codes of conducts.
All data is available based on a reasonable request.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
