
Case Report | DOI: https://doi.org/10.31579/2692-9759/003
1 Head of Department at Cardiology Dow University of Health Sciences
2 Sir Syed University of Engineering & Technology, Karachi, Pakistan
*Corresponding Author: Khalida Soomro, Head of Department at Cardiology Dow University of Health Sciences.
Citation: Soomro K, Muhammad A Soomro (2020) Infectious Aneurysm Formation after Coronary Stent Implantation. Journal of Cardiology Research and Reports, 2(1): 10.31579/2692-9759/003
Copyright: © 2020, Khalida Soomro, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 20 February 2020 | Accepted: 02 March 2020 | Published: 04 March 2020
Keywords: coronary stent infections, complications/diagnosis/therapy, stents/adverse effects, staphylococcus aureus
The formation of coronary artery aneurysm (CAA) is one of the critical complications after percutaneous coronary intervention (PCI). The most common aetiologies and aggravating factors for aneurysmal dilatation are acquired, such as atherosclerosis, Kawasaki disease, Takayasu disease, connective tissue disease, trauma after percutaneous coronary intervention (PCI) and infections. Cardiac catheterization itself carries a negligible bacteremic risk. We present the case of a patient who had infective coronary artery aneurysms that developed after PCI. A 63 years old male who had ST-T MI 1 month back and underwent primary percutaneous coronary intervention with deployment of 1 Des stent in Mid left anterior polymer-based paclitaxel-eluting stent 63 years having primary PCI for LAD 1 month back in the left anterior descending artery and A large aneurysm developed MID DES. The patient had C/O high grade fever only since 3 weeks remained asymptomatic then had angina at rest for 4 days. An aneurysm was diagnosed at middle of DES on repeat coronary angiography. Intravascular ultrasound demonstrated a true aneurysm about 5.6 mm in diameter. We will review the literature and discuss the causes specially infectious aneurysm and treatment option of aneurysm with stent usually detected at the time of repeat angiography for recurrent symptoms or as apart of the routine angiographic follow up [1].
Formation of coronary aneurysm is a rare complication after implantation of bare metal stents (BMS), even in the drug-eluting stent (DES) era the incidence of such complication is still unknown [6, 7, 8, 9, and 10]. The prevalence of coronary artery aneurysms after PCI ranges from 0.2% to 10.5% [2, 3]. The true incidence, clinical course and treatment of coronary artery infectious aneurysm after stent implantation remain largely unknown as occurrence is very rare [4, 5]. As percutaneous coronary intervention has a greater bacteremic potential, presumably due to the prolonged procedural time and the repeated insertion of interventional devices into the vascular system, in apparent bacteraemia occurs frequently (in approximately 30% of cases) after complex percutaneous coronary intervention (PCI); however, clinical sequelae of aneurysm formation rarely occurs. When this septic complication occurs after PCI, morbidity and death often result. [11] Early evaluation is necessary to avoid complications. Dieter’s criteria are often helpful for diagnosis. Such criteria which should have been present either placement of a coronary stent within the previous 4 weeks,h/o multiple repeated procedures performed through the same arterial sheath, presence of bacteremia, significant fever, or leucocytosis with no other cause; H/O acute coronary syndrome,or positive cardiac imaging. Definitive diagnosis is made by autopsy or examination of surgical material here [12, 13]. We are presenting the case of a patient having infective coronary artery aneurysm diagnosed 4 weeks after PCI, to review of literature the possible contributing causes and diagnostic factors.
Case Report
A 65 -year-old male with a history of hypertension, hypercholesterolemia and diabetes mellitus admitted with diagnosis of acute coronary syndrome with ST-segment elevation in Anterior Leads of EKG, The following drugs were administered in the emergency department: Aspirin, 300 mg; tricagrelor 180 mg; Atorvastatin 40 mg laboratory tests were performed, His Blood pressure was 160/100 mmHg and pulse 58/min, regular. Blood chemistry showed total cholesterol 250mg/dl, triglyceride 365mg/dl, high-density lipoprotein cholesterol 28 mg/dl, and LDL-C 170 mg/dl, fasting blood sugar 140g/dl, HbA1c 7.8% under the medication. An Echocardiogram in ER revealed left ventricular end-diastolic dimension of 54mm, Ejection fraction 45% and mild left ventricular hypertrophy. Basal, mid segment of IVS and apex wall segment showed hypo-kinesis while in rest of the segments of LV normal contraction noticed. The patient was taken to the catheterization laboratory

Coronary angiography revealed severe stenosis at the middle portion of the Left Anterior descending Artery (LAD) (Fig. 1A). Lesion was successfully opened and 1 drug eluting stents (Taxus, 3.5 X28 mm) was deployed sequentially after intravascular ultrasound assessment with maximum inflation pressures 14, 12, and 16 ATM respectively (Figures 1B).
He denied any discomfort after the deployment of DES. 4 weeks later he presented with recurrent fever, chills, a persistent dry cough and unstable angina 4 days duration in ER. The presumptive diagnoses on admission were chest infection and acute coronary syndrome.
On admission were chest infection and acute coronary syndrome.
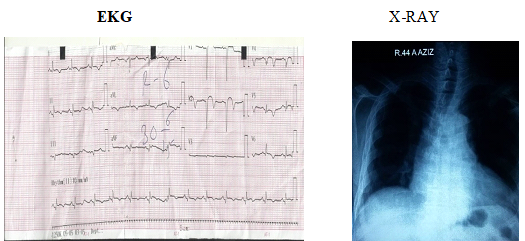
EKG Showed Q-wave with T-wave inversion in the anterior lead (figure 2A) mean while blood culture and other lab test were sent. X-RAY chest was unremarkable.
After 45 min of hospital delay, patient underwent repeat coronary angiography showed no significant stenosis in the right coronary, main left coronary and circumflex arteries but shows LAD eccentric secular aneurysm with tight stent re-stenosis (90% stenosis) at the junction of mid to distal segment at the site of DES implanted 4 weeks back. {Figure 3A}
Assessment of the aneurysmal area using intravascular ultrasound (IVUS, 40 MHz, Boston Scientific Scimed) demonstrated a true aneurysm about 6.5 mm in diameter. Intravenous unfractionated heparin (100 unit/kg) was administered.
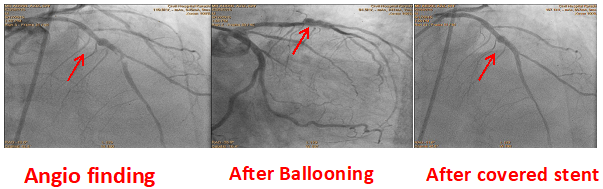
A 0.014 floppy guide wire was positioned in the distal portion of the left anterior descending (LAD) artery through the occlusion. Then, pre-dilation was performed with a 2.5 × 20 mm balloon catheter inflated to 10 ATM and a 275.0 × 24 mm PTEF stent deployed at 10 atm. A good result of the implanted stent was observed on the control coronary angiography, image (3-C).
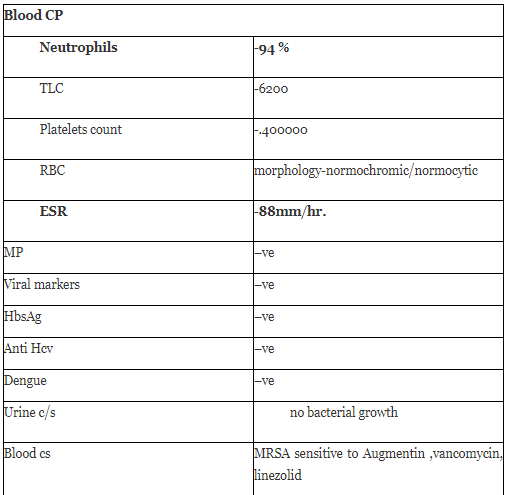
Admission blood cultures grew methicillin-resistant Staphylococcus aureus (MRSA). (Table-1)
Laboratory Tests
Relevant therapy Intravenous vancomycin and gentamicin continued .The patient improved clinically. At the 6-month follow-up, he was asymptomatic, performing his activities of daily living normally, and taking the medications prescribed at hospital discharge.
Coronary Artery aneurysm after coronary intervention are rare.[14] According to a study ,the actual incidence of coronary arterial aneurysm (CAA) formation after Stents implantation is not yet thoroughly surveyed,[15] yet available data shows incidence of 3.9 to 5% after PCI with stents and up to 10% from directional coronary atherectomy. Residual dissection and deep arterial wall injury (rupture or resection of the vessel media) caused by oversized balloons or stents, high-pressure balloons inflations, atherectomy, and laser angioplasty have all been associated with coronary artery aneurysms after coronary intervention. In addition to mechanical risk factor observed for the aneurysm formation with both BMS and DES ,other potential mechanism are also related and Specific to Drug-eluting stents (DES) [16,17,18,19] , although inflammatory and allergic reaction to Nickle and molybdenum have been reported after BMS implantation triggers for inflammatory and allergic reaction after DES implantation are more complex which locally elute anti-proliferative drugs, these can dramatically inhibit neointimal growth , thereby suppressing re-stenosis [20] , DES at the same time potentially cause coronary aneurysms due to other mechanisms alsoDES consists of 3 components the antirestenotic drug ,the drug carer vehicle polymer and stent platform ,in particular the polymer carrier has been shown to provoke eosinophilic /heterophilic infiltration and marked inflammatory reaction of the arterial wall with extensive inflammation consisting of eosinophils and lymphocytes and focal giant cell reaction around the stents struts ,surrounding the polymer after DES implantation. In addition, delayed healing reaction in response to DES such as incomplete endothelialisation over struts have been detected by invasive approaches (angioscopy and optical co-herence tomography) as well as autopsy studies [21]. In short the combination of physical trauma induced by stent implantation and specific biological reactions after DES implantation might together contribute to coronary aneurysm formation after DES implantation and can lead to type 1 aneurysms that demonstrates rapid early growth with pseudo aneurysm formation detected within 4 weeks and arterial injury related procedure is also likely contributor to this type of aneurysm formation [22] And typically complicated by clinical pericarditis [23].

Second type of aneurysm is typically detected incidently during angiography for recurrent symptoms or as a part of protocol mediated angiography follow up (usually detected >6 months duration after the procedure and have most varied presentations [24]. Specially some complains of angina, seems more likely in this scenario that a chronic arterial response to a metal stent, polymer and drug may be basis for aneurysm in this sub type of aneurysm [25]. Our case was having infectious aetiology (type 3) these patients typically present with systemic manifestation and high grade fever as the result of bacteraemia [26, 27]. Whether the local immunosuppressive effects of Eluted drugs from stents tend to increase the incidence of these rare
Infectious aneurysms or multiple risk factors for infections after PCI could have been suspected [28, 29]. Evans and Goldstein noted that any of these events—repeat PCI with re-puncture of the ipsilateral femoral artery within 3 to 7 days of the initial procedure, access site hematoma, or skin drainage—increased the peri -procedural risk of infection to 30%. It has been suggested that small soft-tissue hematomas may impair local host defence mechanisms. McCready and co-authors described re-puncture of the ipsilateral artery and indwelling of the vascular sheath for more than 24 hours after the procedure as major risk factors for post-PCI septic complications. Other predisposing factors may include duration of the procedure, number of passages of the catheters through the femoral sheath, bleeding at the puncture site, and pseudo-aneurysm [30, 31, and 32]. In our patient had none of these risk factors were clearly operative .Staphylococcus aureus and Pseudomonas aeruginosa seem to be the most frequently infective organisms in infected aneurysms [33,34,35,36]. In large infected aneurysms after DES or BMS implantation, Staphylococcus Aureus has been reported as cause of Coronary infection after stenting can present days to weeks after intervention most frequently as an acute coronary syndrome [36,37]. Other complications include thrombosis, distal embolization, and rupture. Evaluation of infection consists of positive blood cultures which are diagnostic of a serious infection but they do not identify the anatomic source of the infection. A radiolabelled leukocyte scan can early confirm the diagnosis [12]. Although angiography remains the gold standard for diagnosis, coronary aneurysms can also be detected by transesophageal echocardiography, contrast-enhanced computed tomography, and magnetic resonance imaging and IVUS [22,25] Aneurysms more than 1 to 2 cm in diameter are unlikely to resolve and they may enlarge and eventually rupture even when the lesions have been sterilized with antibiotics. The frequency of these complications is difficult to determine, because of the extremely low prevalence and lack of published data on coronary artery aneurysms secondary to stent implantation and the absence of natural history data of untreated coronary aneurysms, after stents treatment gives dilemma of treatment on individualized basis on case by case best clinical judgment decision as the treatment for infectious coronary aneurysms is not clear-cut.
Broad spectrum antibiotic therapy and surgical intervention includes stent removal, should be ideal strategy and depends on coronary angio findings. The PCI using PTFE or autologous venous covered stent, the surgical repair with CABG or conservative management under continuing dual-antiplatelet therapy and proper antibiotic therapy are supposed to be considerable strategy. what complicates the clinical decision making process further is the fact that complete resolution of these aneurysms has been observed in some cases without specific treatment ,in contrast to the possibility of rupture if the aneurysm is left untreated [11]. If CAA is small and may have a lower risk for rupture, and conservative management will be more appropriate [32]. As in our case was performed .Covered (polytetrafluoroethylene (PTFE), saphenous vein or papyrus) with spring release inside the aneurysm are the most frequently percutaneous techniques to treat aneurysm [7, 11]. Coil is implanted using a technique that, although aimed only at thrombosis of aneurysms, is technically challenging and associated with risks [1, 20].Surgery should be considered for patients with large aneurysms because of the high risk of rupture. Surgical revascularization procedures include saphenous vein grafting alone or in combination with aneurysm resection [36].
In our patient, the occurrence of bacteremia shortly after coronary artery intervention suggests a causal effect of the procedure on the formation of the aneurysm. however the source was not determined .learning point here is this is one of the rare complication which should come into the mind of cardiologist if patient have fever after stenting, further investigations is necessary to determine the pathophysiology .natural historyand best therapy forinfectious aneurysms .although difficult to prove which is only possible on the examination of the surgical material of autopsy.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
