
Research Article | DOI: https://doi.org/10.31579/2690-1919/458
1 Department of Dermatology, Santa Casa de Misericórdia de Porto Alegre Hospital, Brazil.
2 Department of Infectology, Mãe de Deus Hospital, Brazil.
*Corresponding Author: Jacqueline Sarmento Fernandes, Department of Dermatology, Santa Casa de Misericórdia de Porto Alegre Hospital, Brazil.
Citation: Jacqueline S. Fernandes, Pezzini Teixeira CE, Da Silva CS, Fernanda M. Aguiar, Magda B. Weber, et al., (2025), Infection by Mycobacterium abscessus as a Complication of Calcium Hydroxyapatite Injection: A Case Report and Literature Review, J Clinical Research and Reports, 18(4); DOI: 10.31579/2690-1919/458
Copyright: © 2025, Jacqueline Sarmento Fernandes. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 07 January 2025 | Accepted: 03 February 2025 | Published: 22 February 2025
Keywords: calcium hydroxyapatite; mycobacterium abscessus; atypical mycobacteriosis
Non-surgical aesthetic procedures for managing skin aging have seen increased demand in recent years, among which are injectable collagen bio-stimulators such as calcium hydroxyapatite. These procedures aim at preventing aging and improving skin laxity. Some complications, such as the formation of nodules, hypersensitivity reactions, and granuloma formation, have been reported. In this article, we present a literature review on Mycobacterium abscessus infection following subdermal injection of calcium hydroxyapatite in a 56-year-old healthy woman who developed nodules on the forehead and malar region one month after the application. A culture of a skin biopsy fragment revealed the presence of Mycobacterium abscessus resistant mycobacteriosis, with the patient treated with clarithromycin, amikacin, and tigecycline for 30 days in an inpatient setting. After discharge, treatment continued with oral clarithromycin and doxycycline for 6 months, resulting in clinical cure. There are few reports in the literature of atypical mycobacteriosis following dermal application of bio-stimulators.
The number of aesthetic procedures has been increasing in recent years, with Brazil being one of the leaders in aesthetic interventions worldwide¹. Associated with this rise in demand for aesthetic procedures, there is a growing number of non-medical professionals, such as dentists, biomedical professionals, physiotherapists, and aestheticians, performing invasive procedures³. This article presents a case report of Mycobacterium abscessus infection following dermal injection of calcium hydroxyapatite, of unknown origin, performed by a non-medical professional. The objective of this case report is to alert the risks of procedures performed by non-medical professionals and with materials of unclear origin, as well as to guide preventive and therapeutic measures for similar cases.
Non-tuberculous mycobacterioses (NTM), previously known as atypical mycobacterioses, refer to infections caused by mycobacteria other than Mycobacterium tuberculosis and Mycobacterium leprae⁵. In recent decades, NTM infections related to aesthetic treatments have become more frequent⁸.
These microorganisms are present in the environment: water, soil, and the surface of humans and animals⁴. They may be present on the body surface or even in bodily fluids without causing disease⁷.
The mode of transmission of NTM is not fully understood, but skin and soft tissue diseases are caused by trauma or surgical procedures. Drummond et al. reviewed several risk factors for NTM infection, showing that, in addition to environmental contact, host factors such as genetics and immunosuppression are important considerations⁸.
Skin lesions begin as papules or nodules, as in the case of the patient described, which evolve into tissue necrosis. This tissue necrosis progresses to relatively painless ulcers. The lesion may remain stable or progress to necrosis of adjacent tissues. Despite the low mortality, cases can progress to osteomyelitis or loss of limb function, depending on the location⁸.
The Mycobacterium abscessus complex includes rapidly growing mycobacteria with a high frequency of antimicrobial resistance. Literature reports cases acquired through surgical procedures, mesotherapy, acupuncture, tattoos, and nail treatments⁹. Treatment is not consensual; in general, a combination of macrolides (clarithromycin is typically the choice) with parenteral antibiotics (amikacin, cefoxitin, tigecycline, or imipenem) is used. Treatment usually lasts 4 to 6 months, with possible surgical debridement. When choosing the treatment, it is crucial to consider the antibiogram and each patient’s profile¹⁰.
Calcium hydroxyapatite is presented in a syringe with microspheres suspended in a carboxymethylcellulose vehicle, a substance derived from cellulose and acetic acid, soluble in water, which increases the viscosity of the product ¹¹. It is considered a semi-permanent product with high density and cohesiveness, used to treat areas with bone resorption in the deep compartments of the face ¹². Additionally, it can improve skin quality and smooth wrinkles and grooves. Calcium hydroxyapatite likely works by stimulating fibroblast activity and promoting neo-collagenesis ¹³.
Before application, it is necessary to dilute the product in saline solution or lidocaine to reduce its viscosity. After local asepsis, the product is injected subdermally using a cannula or needle ¹³.
Careful dilution and asepsis before product administration are crucial to avoid infectious processes such as NTM. These microorganisms form a biofilm that can hinder the sterilization process ¹⁰. Furthermore, a study by Rodriguez Jan M. et al. suggested contamination from tap water, highlighting the importance of proper asepsis ⁴.
All the described precautions are essential, assuming the infiltration of an original product. However, as previously reported with hyaluronic acid by Cohen Joel L. et al. and Yuanzhi Liu et al., the product administered may be of unknown origin. In such cases, as in our report, there is no knowledge of the hygiene and sterilization conditions of the product formulation, which increases the risk of infectious processes.
Due to the infection’s potential for antimicrobial resistance and possible sequelae, there should be a high suspicion in cases of nodules after aesthetic procedures. As described by Ianhez Mayra et al., the main complication with collagen bio-stimulators is the formation of nodules, with calcium hydroxyapatite specifically presenting edema¹⁵. In suspected cases of infection, material culture should be performed, and empirical treatment should be initiated¹².
This is a case report associated with a literature review.
A 56-year-old white female patient with hypertension, using hydrochlorothiazide, losartan, and propafenone, presented with a nodular lesion in the left malar region one month after receiving a calcium hydroxyapatite injection in her face by a non-medical professional (Figure 1).

Figure 1: Erythematous-violaceous nodulation in the left malar region, 30 days after the application of collagen bio-stimulator.
She consulted a medical service, where the nodule was drained and antibiotics (amoxicillin and clavulanic acid 875/125mg twice a day for 30 days) were prescribed. A week after this treatment, additional nodules appeared, leading to consultation at the Dermatology Department of the Santa Casa de Porto Alegre.
Physical examination revealed three erythematous, violaceous nodules, hardened in consistency, approximately 1 cm in size, located on the left upper forehead, near the hairline, in the malar region, and at the ipsilateral mandibular angle (Figure 2 and 3).

Figure 2: Two erythematous-violaceous nodulations with hardened consistency in the left malar region and ipsilateral mandibular angle, and one erythematous-violaceous nodulation with hardened consistency, approximately 1 cm in size, in the left upper forehead region, near the hairline.
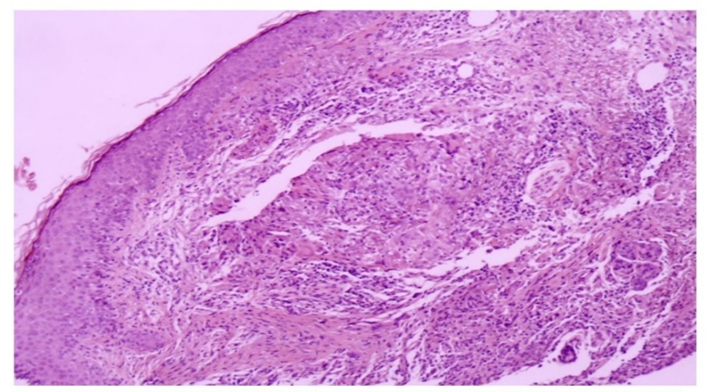
Figure 3: Anatomopathological image of the incisional biopsy of a nodule in the left malar region at 20x magnification, showing chronic granulomatous inflammation in the superficial dermis. Acid-fast bacillus and fungal tests using Ziehl-Neelsen, Fite-Faraco, PAS, and Grocott stains were negative.
An ultrasound of the skin showed focal thickening and increased dermal echogenicity with an anechoic central area in the malar region, suggesting a fluid content. The mandibular angle lesion exhibited a liquid area with peripheral flow on Doppler, suggestive of a collection with an inflammatory process. The frontal lesion showed dermal thickening of an indeterminate nature. Dermis and hypodermis in the malar, zygomatic, and nasolabial folds showed pseudocystic anechoic areas suggestive of a non-permanent filler (hyaluronic acid) and echogenic foci suggesting a permanent filler (calcium hydroxyapatite).
Laboratory tests, including VDRL, FAN, FR, VSG, and PCR, showed no alterations. An incisional biopsy of the left malar lesion revealed chronic granulomatous inflammation in the superficial dermis (Figure 4).
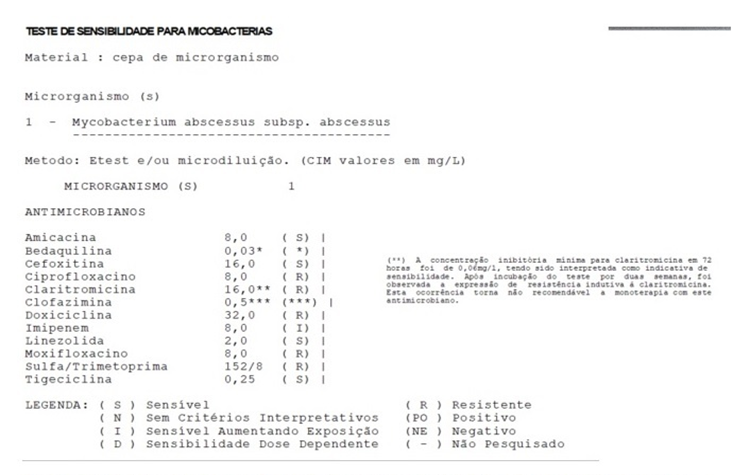
Figure 4: Antibiogram result performed on the sample sent for culture from the incisional biopsy of the nodule in the left malar region.
The acid-fast bacillus test and fungal cultures were negative. A fragment sent for culture was positive for Mycobacterium abscessus, consistent with atypical mycobacteriosis.
The patient was referred to the Infectious Diseases service, where inpatient treatment with clarithromycin (500 mg every 12 hours), linezolid (600 mg daily), and amikacin (500 mg intravenously three times a week for 30 days) was initiated following the antibiogram results (Figure 5).
After clinical cure, the patient remained without recurrence of lesions for the past 16 months of follow-up.
The patient presents an otological sequela from intravenous amikacin use, including permanent tinnitus and mild hearing loss.
A search in the PubMed database using the terms: bio-stimulator, calcium hydroxyapatite, Mycobacterium abscessus, atypical mycobacteriosis; did not yield previous reports of non-tuberculous mycobacteriosis specifically related to the application of calcium hydroxyapatite. It is important to note that the search in PubMed was limited to articles in English or those with translated titles. Additionally, there may be similar unreported cases in the scientific community.
The authors declare no conflict interests.
There is undeniable growth in the demand for non-surgical aesthetic procedures, with several reasons, such as shorter recovery times ¹. However, the increasing availability of these procedures, including those performed by non-medical professionals, should also be considered ³. As explained earlier, NTMs are environmental microorganisms, with defense mechanisms that make sterilization challenging ¹⁰. Like other materials used in aesthetic procedures, calcium hydroxyapatite requires subdermal infiltration and prior dilution ¹³. Therefore, attention to asepsis, sterilization, and material provenance is crucial to avoid potential infectious processes.
It is essential to ensure the surveillance and quality control of the materials used and the technique, through public authorities and health surveillance, given that this is an invasive procedure with serious complications and potential sequelae.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
