
Case Report | DOI: https://doi.org/10.31579/2690-8808/214
1MD Pediatrics Hematologist Oncologist, College of Medicine / Al-Qadisiyah University
2MD Pediatrics Hematologist Oncologist, AlMojtaba hematology and BMTcenter /Health Authority and Medical Education
3MD Pediatrics Oncology resident/ AlMojtaba hematology and BMTcenter /Health Authority and Medical Education
*Corresponding Author: Abdulaziz Wannas Abd, Pediatrics Hematologist Oncologist, College of Medicine / Al-Qadisiyah University.
Citation: Abdulaziz W. A., Allawi N. H., Entisar H. M., Amir F. M., Samaher A. F, et. al., (2024), Infantile hemangiomas mimic neurogenic tumor behavior, J, Clinical Case Reports and Studies, 5(7); DOI:10.31579/2690-8808/214
Copyright: ©, 2024, Abdulaziz Wannas Abd. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 August 2024 | Accepted: 21 August 2024 | Published: 27 August 2024
Keywords: giant retroperitoneal hemangioma; thrombocytopenia; steroid; VCR therapy
Kasabach-Merritt syndrome (KMS) is a rare disorder that can affect infants from the time of birth, or may appear later in infancy as the vascular malformation grows. KMS require intensive resuscitation by blood and blood product to avoid life threating hemorrhage. A 6-month-old female previously healthy, presented with one-month history of skin rash involving the napkin area with extension to the back. This rash was discovered following her visit to a primary health care center for her routine vaccination and appeared four days after receiving the vaccine. The rash extended over the napkin area without any fever, no itching and no involvement of other parts. Mother tried different types of topical treatments such as creams prescribed by the dermatologist but the patient’s condition did not improve with the peripheral blood sample showing low platelets. Full investigation was done at the hospital and a huge mass was discovered in the para-spinal area involving overall the lumber vertebrae and mildly compressing the spinal cord therefore suggesting a neurogenic tumor by imaging study but later on the tru-cut biopsy actually revealed it to be a vascular tumor namely infantile hemangioma with CD31 positive. Although medical treatment by combined steroid and vincristine are widely used to achieve control over the complications of giant vascular abnormalities, the effect of these drugs are mainly on the symptoms of KMS such as correcting the bleeding profile but without significant effect on the tumor size. Once the diagnosis of KMS was established, multidisciplinary team was required.
The association of hemangioma, thrombocytopenia, and hypofibrinogenemia was first described in 1940 by Kasabach and Merritt [1] who took care of an infant with a giant capillary hemangioma and thrombocytopenic purpura. Kasabach-Merritt syndrome (KMS) is a rare disorder that can affect infants from the time of birth, or may appear later in infancy as the vascular malformation grows. Diagnosis of KMS is made based on the constellation of a vascular lesion, thrombocytopenia, consumptive coagulopathy, and microangiopathic hemolytic anemia. Unlike true capillary hemangiomas that regress in childhood and are a cosmetic nuisance, the lesions in KMS are distinctive vascular tumors that include tufted angiomas and kaposiform hemangioendotheliomas [2]. It is exclusively associated with the vascular tumors kaposiform hemangioendothelioma (KHE) and tufted angioma (TA), which exist along the same neoplastic spectrum. Treatment includes supportive therapy and management of the underlying tumor [3 ,4].
KMP occurs exclusively as a complication of KHE and TA, which are rare, benign vascular tumors that typically present in infancy. KHE and TA are classified as having intermediate malignant potential as they are locally aggressive but are not known to metastasize [5,6]. Treatment aims to involute the tumor to prevent significant morbidity or mortality, or in response to a life-threatening event. Surgical excision is curative but most lesions are not amenable to this option. Historically, the first-line of treatment has been high-dose systemic corticosteroids. However, up to two-thirds of lesions will not respond to corticosteroids, or will quickly relapse once treatment is discontinued [7]. Also, this treatment is not without its own troubling adverse effects. A number of alternative therapies have been tried with variable results, including interferon α−2a and 2b, radiation therapy and chemotherapeutic agents such as vincristine and actinomycin [8].
A 6-month-old female presented with one-month history of skin rash involving the napkin area with extension to the back and the lower abdomen (figure -1), she was previously a healthy infant till 5-month age until this rash was discovered during a routine visit to the primary health care for vaccination, 4 days after receiving the vaccine, the rash extended over the napkin area without any fever, no itching and no rash at other sites. Mother tried different types of creams prescribed by the dermatologist but the patient’s condition did not improve, and over time the skin lesion changed from dark red to a pinkish color as well as the peripheral blood sample showing low platelets by routine investigations during follow up. Full investigation was done at the hospital which discovered a mass in the para-spinal area, CT abdomen was seen by three diagnostic radiologists showing right 7.5 x 2 cm para-spinal mass, overall involving the lumber vertebrae and mildly compressing the spinal cord. Suggesting it to be a neurogenic tumor while the size continued to grow reaching 8x4.4x6.2 cm after 12 weeks of treatment{figure-2}. As per history provided by the parents, such skin rash was not present at the time of birth. The retroperitoneal swelling later on was diagnosed as a giant infantile hemangioma and the patient was admitted to the Pediatrics department at Al-Mojtaba hematology and bone marrow transplant center. Tru–cut biopsy from the mass shows vascular proliferation of capillary sized vascular spaces with CD31 diffusely positive, these massive lesions were related to the hemangiomas. Bone marrow, following aspiration, was active & hyper-cellular. Surgical consultation for interventional radiology reported the mass could be controlled by trans-arterial embolization after stabilization of her condition and after the age of 1 year.

Figure 1: The skin lesion of the infantile hemangioma at different times (6 month and 8 months age).
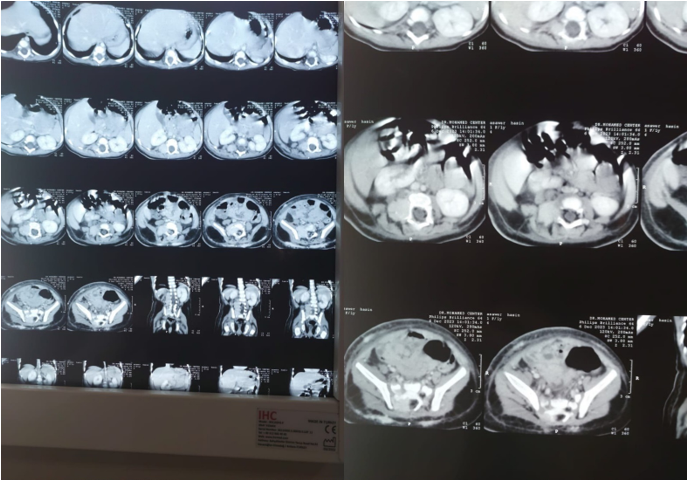
Figure-2: presences of Para-spinal hemangioma which is highly suggest neurogenic tumor by image studies.
Initially, the patient was put under our observation and regular follow up was done to assess the disease progression and to reassure the family, as parents of the child were apprehensive and did not agree to any kind of intervention. We were able to see the changes in size and skin texture of the rash at the age of 8 months. We treated the patient by daily cryoprecipitate, plasma, platelets infusion and packed RBCs according to the hemoglobin level and vitamin K every other day and started combined steroid with vincristine weekly for 12 weeks used to achieve control over the complication of giant vascular abnormalities, the effect of these drugs were mainly on the symptoms of KMS and correcting the bleeding profile without significant effect on the tumor size. At presentation, the mean platelet count was 17× 109/L (range: 17.2–2.600 × 109/L) diagram-1, WBCs 18.0 x 109/L diagram-2, PT 33.3 sec (range 33.3-14) diagram-3, INR 2.9 (range 2.9-1.1) diagram-4 (range: 18.0–7.600 × 109/L) while the mean fibrinogen level was 50mg (200-400 mg/dl). The patient was anemic during the entire period of treatment, with a mean hemoglobin of 8.3 g/L (range: 7.7–10.9) diagram-5. With a normal differential count and a normal peripheral blood film except for thrombocytopenia.
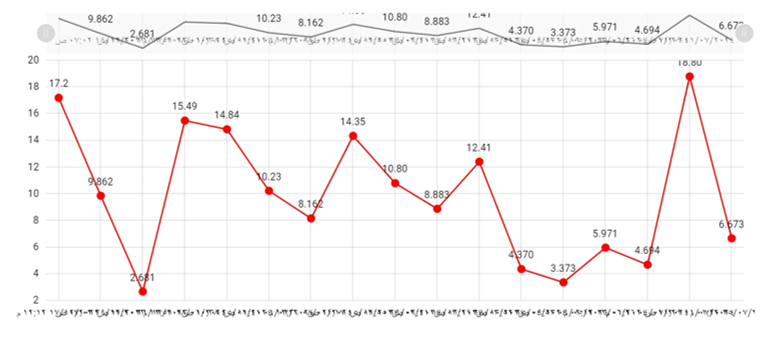
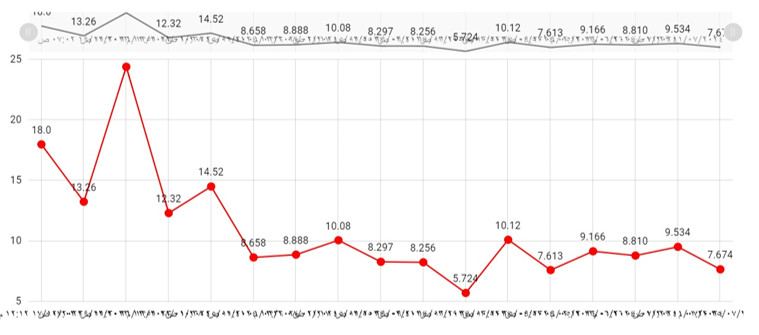
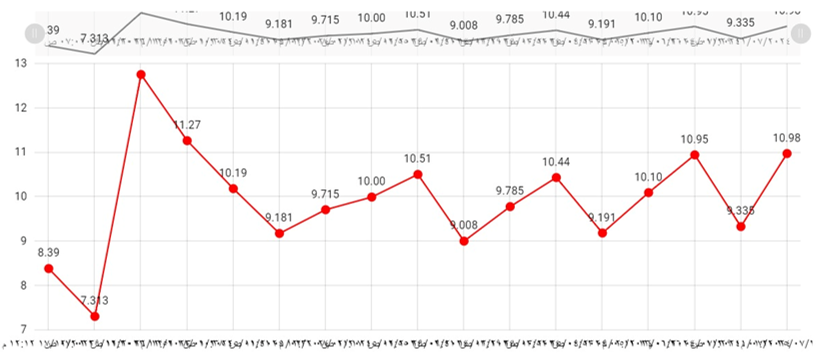
Diagram 1-3: shows the blood elements (platelets, hemoglobin, WBCs) before and during 12 weeks’ treatment, respectively.
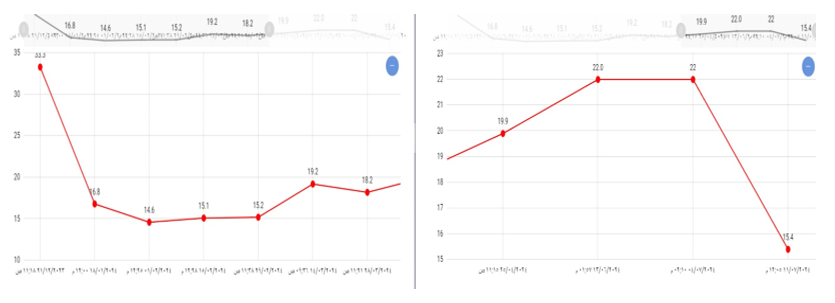
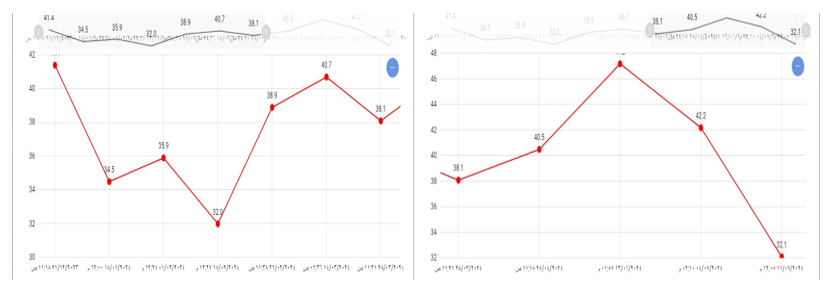
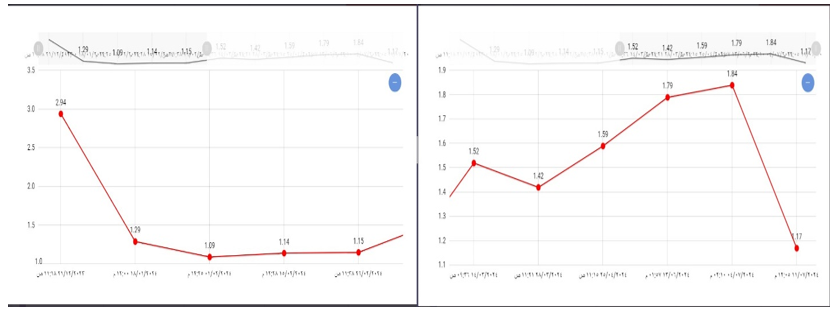
Diagram 4-6: shows the levels of bleeding parameters (PT, PTT, INR) before and during 12 weeks’ treatment, respectively.
Unlike this case, most of the lesions are located on the extremities. Some infants and older children with visceral lesions present with an enlarged abdomen. Those with hepatic kaposiform hemangioendotheliomas also may present with hepatomegaly or jaundice. These vascular lesions may continue to enlarge during the first 18 months of life. The thrombocytopenia and consumption coagulopathy associated with KMS may not initially be severe. However, symptoms may worsen as the lesion enlarges and the infant grows. Affected infants may present soon after birth or may not come to medical attention for several months. Affected individuals rarely present as late as the second or third decade of life. Petechiae, bruising, and frank bleeding may be the initial symptoms prompting medical treatment. The lesions may be painful. The large volume of blood circulating through the lesion may cause high-output congestive heart failure in infants [9]. The hemangioma is often within the skin but can be present anywhere, including retroperitoneal organs, the mediastinum, the pelvis, visceral organs, or the mesentery. For skin lesions, the mortality rate, with treatment, is under 10%, but retroperitoneal tumors like this case have a mortality rate of approximately 60% [10]. Treatment of KMP is largely supportive and aimed at preventing life-threatening complications while addressing the underlying tumor. While the thrombocytopenia of KMP may be profound, life-threatening hemorrhage is, in fact, rare, similar to our case and platelet transfusion is not recommended except in the cases of active bleeding. Transfused platelets may become trapped in the tumor and lead to further abnormal coagulation, worsening KMP [11]. Symptomatic anemia should be treated with red blood cell transfusion. In cases of bleeding or as preparation for surgery, cryoprecipitate may be administered [12,13].
Multicenter expert management of Kasabach-Merrit syndrome by corticosteroid and vincristine together at the same time with other centers uses these drugs as monotherapy [14]. The advantage of vincristine is to induce apoptosis of the cells and prevent angiogenesis [15], these two drugs when used together like in this case led to the correction of the bleeding profile and decrease in the PT, PPT, INR and fibrinogen level after 12 weeks of treatment and stabilization of the tumor without significant regression. In the literature, the length of corticosteroid and vincristine therapy varies from one month to one year according to the clinical response because complete clearance of this tumor rarely occurs and residual tumor fibrosis is common [16].
The diagnosis and management of retroperitoneal infantile hemangioma requires a multidisciplinary team that includes an Oncologist, hematologist, interventional radiologist, intensivist, nurse practitioner, and the primary care provider. Once the diagnosis is made, the treatment is largely supportive and includes prevention of life threatening complications like hemorrhage. The underlying tumor must be treated. Surgery and arterial embolization carry high risk of injury to adjacent structures. In some children, radiation may induce regression of the mass, but the therapy can also lead to growth retardation and induction of secondary malignancies. Less potency chemotherapeutic agents Vincristine weekly with oral prednisolone used carry good symptomatic response but the tumor size response is less significant. The outlook for most children with KMP is guarded.
Unfortunately, many vascular lesions involving the retroperitoneal region may represent as neurogenic tumor by image study. These misdiagnoses of vascular anomalies or aggressive vascular tumors may lead to improper intervention and improper management.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
