
Case Report | DOI: https://doi.org/10.31579/2768-2757/128
1Professor & Head. Microbiology Deptt., Kiran Medical College, Surat.
2Associate Professor, Microbiology Deptt. Gove medical College, Kota.
3Assistant Professor, Microbiology Deptt., PMCH, Udaipur.
*Corresponding Author: Rajeev Shah, Professor & Head. Microbiology Deptt., Kiran Medical College, Surat.
Citation: Rajeev Shah, Suchitra Morya, Nitika Sharma, (2024), Indoor Biomass Fuel as A Higher Risk Factor of Rti and Tb in Hiv Positive Female More Than Male Patients of Western India, Journal of Clinical Surgery and Research, 5(6); DOI:10.31579/2768-2757/128
Copyright: © 2024, Juan A. Ricciardi V. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 13 May 2024 | Accepted: 19 July 2024 | Published: 02 August 2024
Keywords: nasal bone fracture; open reduction; blunt facial trauma
Background: It is well known that one third poor population of world use biomass fuel for cooking and heating. It is universally accepted fact that bio-mass fuel plays a significant role as predisposing factor of tuberculosis, acute respiratory tract infections and COPD even in non-immune-suppressed (HIV sero-negative) individuals. As we all know house hold cooking is the primarily performed by women. So close association with bio mass fuel and even longer duration to it make women more vulnerable to this RTI secondary RTI infections.
Aim: To study effects of biomass fuel on prevalence of RTI/tuberculosis on HIV-infected patients of Gujarat.
Material & Methods:In the present study 961 HIV infected patients with RTI and 300 HIV infected patients without RTI and 300 HIV-uninfected patients with RTI were surveyed for use of bio-mass fuel or clean fuel. Result.
Conclusion: It had been surveyed, statistically analysed and had been found even higher risk predisposing factor mainly for tuberculosis and other acute respiratory tract infections in immune-suppressed HIV-sero positive patients. Here biomass fuel had been evaluated as a risk factor in developing TB in HIV patients and incidences of RTI in HIV sero-positive patients had been found in our study that those who were found to have 2.3 times higher risk of contracting respiratory tract infections as compared to those who were not suffering from HIV. Even among all these RTI patients who might acquire secondary RTI infections due to bio mass fuel, 61.87 % were found to be women. When only TB is considered in this study it was found 67.44 % women were observed suffered from TB when compared with same group males. This increased infected woman to TB and COPD in turn results in preterm delivery which leads to birth of low birthweight babies if women are pregnant.
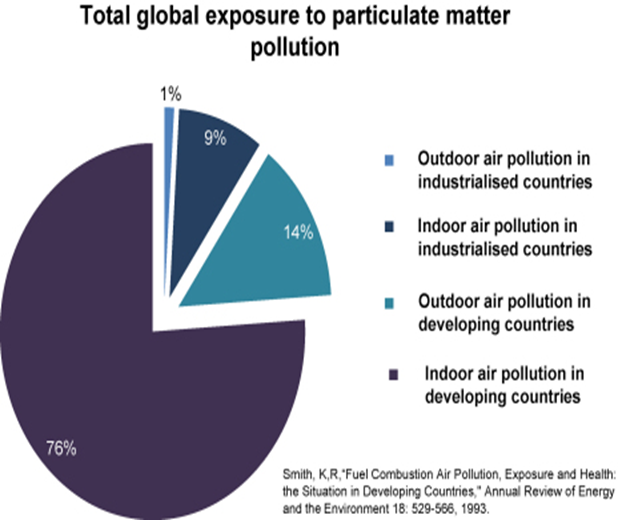
BMF refers to burned plant or animal material; wood, charcoal, dung and crop residues account for more than one-half of domestic energy in most developing countries and for as much as 95% in lower income countries (Smith et al., 2004). Around 2.4 billion people rely on BMF as their main source of domestic energy for cooking, heating and lighting (Reddy et al., 1996, Smith et al., 2004) and a further 0.6 billion people use coal. The adverse health effects of indoor air pollution are often exacerbated by lack of ventilation in homes using BMF and by the poor design of stoves that do not have flues or hoods to take smoke out of the living area. The combustion efficiency of BMF is also very low, thus it yields relatively high levels of products of incomplete combustion, which are more damaging to health.
The polluting effect, efficiency and cost of domestic fuel use are often construed as an ‘energy ladder’ (WHO, 2006a). Dried animal dung, scavenged twigs and grass, which are cheap, inefficient and pollute the most, are at the bottom of the ladder. Crop residues, wood and charcoal are a higher level BMF, whilst kerosene, coal and bottled or piped gas are the most efficient (non-BMF) combustible energy sources. Electricity is at the top of the energy ladder. The correlation of socioeconomic factors with the main fuel used is relatively close, however most households use several fuels in different settings. Four factors that appear to be most relevant in a household's choice of fuel type are: (a) cost of fuel, stove type and accessibility to fuels; (b) technical characteristics of stoves and cooking practices; (c) cultural preferences; and lastly, if at all, (d) the potential health impacts (Masera et al., 2000).
Inefficient burning of BMF on an open fire or traditional stove generates large amounts of particulate matter as well as carbon monoxide, hydrocarbons, oxygenated organics, free radicals and chlorinated organics (Naeher et al., 2007). The particulate matter component of this smoke is classified according to its size, with inhalable material <10>
The RTI are among the first opportunistic infections, observed in HIV patients and unlike HIV sero-negative persons some of the RTI even causes permanent damage to respiratory tract, thus affecting both quality and quantity of rest of their life. So, it is very important to prevent RTI in HIV patients by understanding risk factor for RTI in them. In this study we tried to understand the effect of biomass fuel (BMF) on opportunistic RTI in HIV patients.
| HIV+ | HIV- | Total | |
| RTI+ | 961 | 300 | 1261 |
| RTI- | 300 | 217 | 517 |
| Total | 1261 | 517 | 1778 |
Table 1: Occurrence of RTI among those reporting to ART centre.
OR=2.317 and 95% CI = 1.86 to2.88
It can be seen that those who were detected as HIV+ had 2.3 times higher chance of contracting respiratory tract infection as compared to those detected negative for HIV. The 95% confidence interval not including the null value (OR=1) indicates the significant association of the HIV status and the occurrence of RTI.
Globally, total number people living with HIV in 2012 are 35.3 million. In parts of the world where HIV infection is most common, BMF is the main energy source. In Malawi, for example, the incidence of HIV in pregnant women is 33%, and 70% of hospital admissions and >80% of households use BMF. However, the influence of BMF smoke on HIV-infected individuals has not been clarified.
The most important effect of HIV infection in Africa is to cause increased bacterial infections, pneumonia and TB. HIV infection is associated with mild airway obstruction and loss of gas transfer, with severe impairment occurring in the presence of Pneumocystis jiroveci infection (Mitchell and Clarke, 1995). HIV is also associated with the accelerated development of COPD (Diaz et al., 2003) and it is likely, although not proven, that HIV infection is a significant contributor to airway disease in much of the adult population of Africa. Since both BMF use and HIV are associated with an increase in the incidence of pneumonia (Gordon et al., 2002; Smith et al., 2000) and as particulate matter exposure and HIV result in increased
pulmonary inflammation (Ghio et al., 2000; Rowland-Jones, 2003; van Eeden et al., 2001), it is possible that by causing pulmonary inflammation the two major risk factors for pneumonia in African adults (HIV and BMF smoke) may actually demonstrate previously unrecognised synergy.
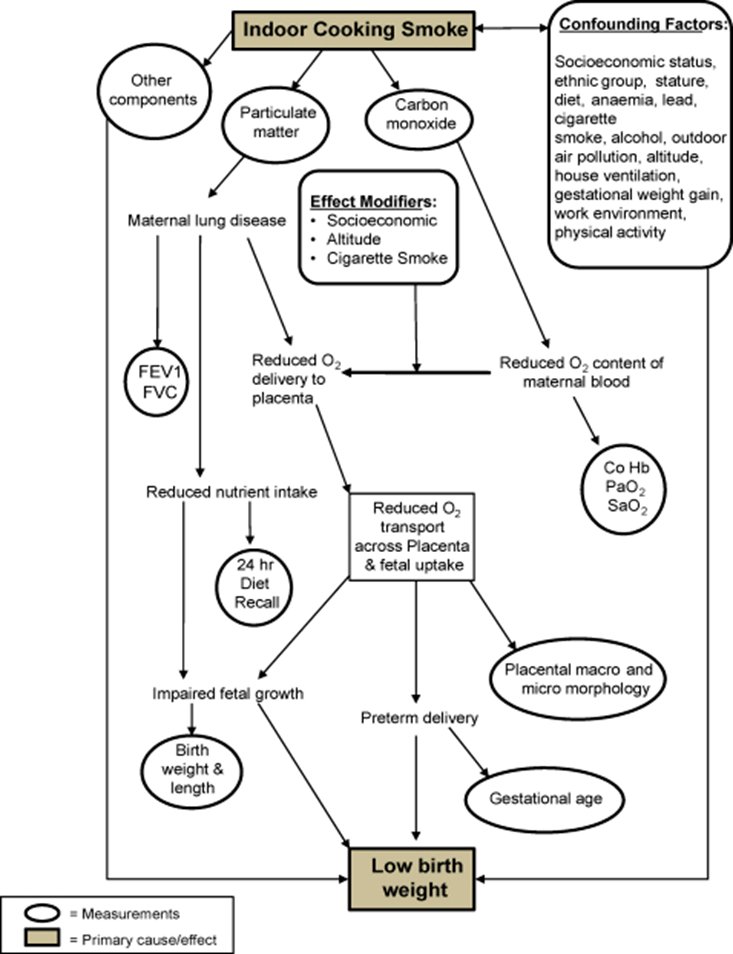
Evidence exists that implicates exposure to BMF smoke in adverse effects on different birth outcomes (Sram et al., 2005). There is a published association of low birthweight, intrauterine growth retardation and perinatal mortality with air pollution (Dejmek et al., 1999, Mavalankar et al., 1991, Wang et al., 1997). A study from Guatemala identified an association between birthweight and type of fuel used. The use of an open fire produced average levels of PM10 of 1000 μg/m3. The babies of mothers using open wood fires were on average 63 g lighter compared with babies born to mothers using cleaner fuels (Boy et al., 2002). A similar (slightly larger) effect has also been reported in Zimbabwe (Mishra et al., 2004). The model in figure below attempts to explain how BMF may fit into a multifactorial explanation of low birthweight.
Tuberculosis is the second most common cause of death globally in adults attributable to a single infectious agent (WHO, 1998). Tuberculosis remains the leading cause of death due to infection in India, which bears nearly 30% of the global tuberculosis burden (Dye C, Scheele, 1999; 282: 677–686).Each year, 2 million people in India develop tuberculosis and nearly 500 000 die from it, averaging more than 1000 TB deaths a day (WHO, 2000). India has the largest pool of people infected with tuberculosis (mycobacterium tuberculosis) with an annual incidence 1.98 million, the largest number in any one country and catering to a fifth of the global burden of TB. It is estimated that more than half of India’s adult population is infected with tuberculosis bacterium, mycobacterium tuberculosis. Once a person is infected, any condition that weakens the immune system can trigger the development of active tuberculosis. Typically 5 to 10% of these infected eventually become ill with active tuberculosis (ATS 1990). However this percentage may be higher in the case of India, because of the ubiquity of the tuberculosis bacillus, high population density and poor socioeconomic and health conditions. Approximately 500,000 persons die from tuberculosis each year in India. In recent years, the growth of drug resistant tuberculosis and the rapid spread of human immunodeficiency virus (HIV) and acquired immunodeficiency syndrome (AIDS) has contributed to the resurgence of tuberculosis in India and in other parts of the world (Raviglione MC, 1995;Piot P, 1997; Kochi A, 1994; WHO, 1992;Sawert H, 1996). NFHS recorded an overall active tuberculosis prevalence rate of 467 per 100,000 persons (IIPS, 1992) slightly higher than other estimates of the active (sputum positive) disease rate in India, which mostly range between 400-450 per 100,000 persons (WHO, 1992). Tuberculosis is a social disease with medical aspects and it has been described as a barometer of social welfare. As the women spend much more time in proximity to biomass fuel for cooking they were found at higher risk of acquiring secondary RTI and TB than male staying in the same home.
| FTB+/HIV+/RTI+ (T) | FTB-/HIV+/RTI- (C2) | P | |||
| (n) | % | (n) | % | ||
| Female Patients using Biomass fuel | 52 | 69.33 | 47 | 35.33 | 0.05 |
| Total Female Patients | 75 | 133 | |||
| Male Patients Using Biomass fuel | 71 | 52.98 | 61 | 36.52 | 0.10 |
Table 2: Comparison of Risk of acquiring TB between TB patients from HIV sero-positive patients from T group and HIV/TB negative patients from C2.
In our present study biomass fuel was found statistically significant predisposing factor of TB with p value found to be 0.5 in female and 0.10 in male it was found less significant, when compared between TB Patients of group C1 and non-TB patients of group C2 (Table 2).
The reason seems to be very simple and well understood that in our society mostly female are supposed to cook food, so spending much more time in close proximity to sources of biomass fuel during cooking food for the family even though she might be even HIV-sero-positive. While males of same family with sero-positivity of HIV spend most of their time either out of home or away from the sources of biomass fuel. So naturally acquire less bad effects of biomass fuel and that is why the chances of acquiring TB due to the bad effect of biomass fuel was found very less when compared with same group of male.
Weather cooking had been done outside of home or even in well ventilated home, the chances of bad effect of biomass fuel always remains more due to close proximity and longer duration of time for women to the biomass fuel sources than men, who very rarely contribute in cooking the food. So, in my present study proved that HIV positive women are at higher risk of acquiring secondary RTI, COPD and TB than HIV positive male patients due to indoor biomass fuel. If such HIV positive women are pregnant it may leads to preterm delivery and low birth weight babies.
Indoor air pollution from BMF disproportionately affects women and children and is the cause of significant global mortality and morbidity in even normal HIV negative women. Here our study proved that the HIV positive person have 2.3 times higher risk of contracting respiratory tract infections as compared to those who were not suffering from HIV. Even among all these RTI patients who might acquire secondary RTI infections due to bio mass fuel, 61.87 % were found to be women. When only TB is considered in this study it was found 67.44 % women were observed suffered from TB when compared with same group malesThis is a neglected area of global disease that affects a large proportion of the world's population.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
