
Case Report | DOI: https://doi.org/10.31579/2639-4162/046
1 PGY-3 Resident Department of Oral and Maxillofacial Surgery Eisenhower Army Medical Center Fort Gordon, GA 30905
2 Residency Assistant Program Director Department of Oral and Maxillofacial Surgery Eisenhower Army Medical Center Fort Gordon, GA 30905
3 Residency Program Director Department of Oral and Maxillofacial Surgery Eisenhower Army Medical Center Fort Gordon, GA 30905
4 PGY-4 OMS Resident Department of Oral and Maxillofacial Surgery Eisenhower Army Medical Center Fort Gordon, GA, 30905
*Corresponding Author: Andrew C. Jenzer, Residency Assistant Program Director Department of Oral and Maxillofacial Surgery Eisenhower Army Medical Center Fort Gordon, GA 30905
Citation: Tyler J. Hagler, Andrew C. Jenzer, Joseph W. Ivory, Jai-ik Cho, (2021) Incidental Finding of Unilateral Parotid Gland Agenesis: A Case Report. J. General medicine and Clinical Practice. 4(1); DOI:10.31579/2639-4162/046
Copyright: ©2021 Andrew C. Jenzer, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 10 February 2021 | Accepted: 11 June 2021 | Published: 16 June 2021
Keywords: maxillofacial surgery; maximal interocclusal opening
A 34-year-old male active duty soldier presented to the Dwight David Eisenhower Army Medical Center (DDEAMC) Oral and Maxillofacial Surgery Clinic on referral from a local General Dental Clinic for a reported history of temporomandibular joint painful popping and clicking, favoring the right side. As a component of the patient’s outpatient clinical workup, an MRI of the bilateral temporomandibular joints was ordered with an incidental finding noted of partial-to-complete absence of the left parotid gland. The patient completed a conservative therapy regimen and subsequently underwent a non-arthroscopic lysis and lavage of the right temporomandibular joint with resolution of the index symptoms.
A 34-year-old male active duty soldier was referred to the DDEAMC Oral and Maxillofacial Surgery Clinic for evaluation and treatment of temporomandibular joint pain favoring the right side. The patient had a non-contributory past medical history with a reported allergy to sulfa based medications. His surgical history was notable for septoplasty and a vasectomy with subsequent reversal. On initial evaluation, the patient reported frequent, painful clicking and popping of the right temporomandibular joint. These symptoms were described as progressive in nature over the preceding three years.
On clinical examination, the patient was found to have a stable occlusion in a good state of repair with missing teeth #1, 16, 17, and 32. Bilateral temporomandibular joint pain was appreciated on opening, to include reciprocal popping and clicking observed on the right side. Maximal Interocclusal Opening (MIO) was noted to be approximately 37 millimeters without pain. No deviation of the mandible was noted and occlusal range of motion was found to be repeatable. The patient denied tenderness on palpation of the bilateral muscles of mastication. A Mahan Test was performed at chairside with negative findings.
A series of existing dental plain film radiographs and a panoramic image were all reviewed with unremarkable findings. At the conclusion of the initial evaluation, the patient was provided instructions on conservative therapy measures to include soft diet modification, application of warm compresses to the affected areas, stretching exercises, and the use of as-needed non-steroidal anti-inflammatory (NSAIDS) medications. In addition, an MRI of the temporomandibular joints was ordered to facilitate final diagnosis of the patient’s suspected internal derangement of the right joint.
A Multiplan Multisequence Image (MRI) of the bilateral temporomandibular joints was completed without intravenous contrast. The study was reviewed by a radiologist and the oral surgery team. There was no evidence of focal abnormalities involving the left disc tissue, though subtle anterior displacement of the left discal tissue was noted. The right disc was found to be of appropriate morphology and appreciated in the appropriate position on both opening and closing. An incidental finding of missing left parotid gland tissue was noted with fatty tissue in the expected anatomical position (Figures 1, 2, 3).
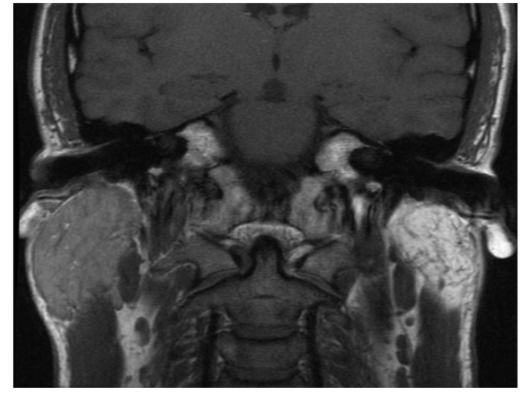
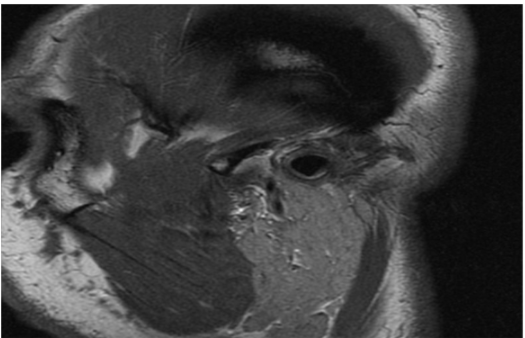
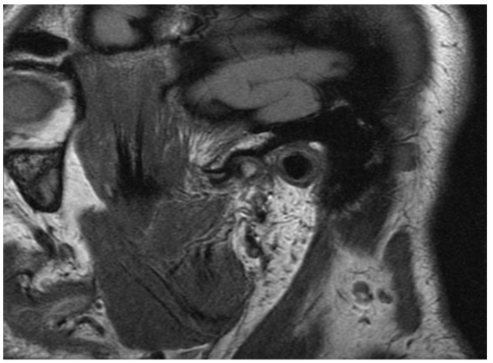
The right parotid gland was observed and found to be unremarkable. Formal review by the radiologist highlighted the unusual nature of this findings and indicated that absence of the left parotid gland is likely congenital with the observed overlying soft tissue structures representing a rudimentary gland.
The patient was re-evaluated and diagnosed with Anterior Disc Displacement (ADD) with Reduction of the Right Temporomandibular Joint with examination findings consistent with a Wilkes Stage II disease classification. The patient denied any benefit from conservative therapy measures and elected to pursue surgical options given the continued pain and reported impact on daily quality of life. The patient was consented for non-Arthroscopic lysis and lavage of the right temporomandibular joint with placement of medications into the joint and manipulation under anesthesia. The procedure was completed without complication, as an outpatient in operating room setting, under general anesthesia. Therapeutics included intra-articular administration of both Kenalog and Hyaluronic Acid. The patient was seen on follow-up and reported satisfaction with the procedure with an improvement in symptom severity and frequency. No additional procedures were discussed and the patient remains on as-needed recall with Oral and Maxillofacial Surgery Service.
Incidental discovery of missing salivary glands, commonly known as agenesis of the salivary glands, represents an exceedingly rare phenomenon.[1,2] In particular, congenital agenesis of the parotid gland has been described in the literature with both unilateral, bilateral, and presentations involving multiple other major salivary glands. [7,8,9,10] There have been cases reported with syndromic associations such as hemifacial microsomia, cleft palate, Levy-Hollister Syndrome, but also single cases Klinefelter Syndrome and Down Syndrome. [3,13]
This condition is frequently described as asymptomatic in nature and this case represents a new asymptomatic, incidental discovery on routine imaging for an unrelated condition. [11] Symptomatic patients can experience xerostomia leading to a higher indicent of dental caries and possible facial asymmetry. The precise incidence of unilateral congenital parotid gland agenesis is difficult to ascertain and less than 30 cases have been reported in the literature to date. [1-6] There does not appear to be a gender predilection and a wide range of ages have been reported on discovery. Of note, unilateral agenesis of the right parotid gland has been reported more than twice as frequently as unilateral agenesis of the left side. [9,11,12]
In many of the reported cases, authors have described hypertrophy of the contralateral parotid gland thought to be secondary to a compensatory function. This present case did not demonstrate any gross evidence of contralateral hypertrophy. Additional modalities such as salivary function scintigraphy and computed tomography may be useful to better appreciate the presence of any accessory parotid tissue as well as the general status of the duct system in this patient.
Given the asymptomatic nature of the present case, the patient was informed of the findings and no further workup was indicated. This case is limited in that the authors were unable to classify this patient into any known maxillofacial syndromes or combination presentations.
DISCLAIMER:
The views expressed herein are those of the authors and do not reflect the official policy of the Department of the Army, Department of Defense, or the United States Government.
DISCLOSURE:
None of the authors reported any disclosures.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
