
Research Article | DOI: https://doi.org/10.31579/2643-6612/034
1 Department of conservative dentistry, Faculty of Dentistry, Genius University for Sciences & Technology, Dhamar city, Republic of Yemen.
2 Department of conservative dentistry, Faculty of Dentistry, Sana’a University, Republic of Yemen.
3 Orthodontics, Pedodontics and Prevention Department Faculty of Dentistry, Genius University for Sciences, Technology, Dhamar city, Republic of Yemen.
4 Department of Basic Sciences, Faculty of Dentistry, Sana’a University, Republic of Yemen.
5 Medical Microbiology department, Faculty of Medicine, Genius University for Sciences & Technology, Dhamar city, Republic of Yemen.
*Corresponding Author: Hassan A. Al-Shamahy, Department of Basic Sciences, Faculty of Dentistry, Sana’a University, Republic of Yemen.
Citation: Mohammed M. A, Mohammed A. A, Khaled A. A, Hassan A A, Mohammed M. (2022). In Vitro Antifungal Susceptibility of Candida Albicans Isolated from Yemeni Patients with Denture Stomatitis. J Dentistry and Oral Maxillofacial Surgery, 5(3); DOI: 10.31579/2643-6612/034
Copyright: © 2022, Hassan A. Al-Shamahy. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 May 2022 | Accepted: 30 May 2022 | Published: 13 June 2022
Keywords: Candida albicans; Candida-associated denture stomatitis (CADS); in vitro antifungal susceptibility testing (AFST); Yemen
Background and aims: Candida-associated denture stomatitis (CADS) is a common fungal infection in people who wear dentures. The main objectives of this study were to identify the causative agents of CADS and in vitro antifungal susceptibility testing (AFST) for Candida albicans in Yemeni patients with denture stomatitis.
Methods: A total of 88 Candida spp. obtained from patients with denture stomatitis. Candida spp were identified using standard microbiological methods. The in-vitro antifungal susceptibility of Candida albicans. to fluconazole (FCZ), itraconazole (ICZ), voriconazole (VCZ), and amphotericin B (AMB) was evaluated using the E test strips. Interpretive sensitivity criteria for antifungal breakpoints were adapted from the Clinical and Laboratory Standards Institute (CLSI).
Results: Overall, C. albicans was the most commonly isolated species (
Wearing dentures and inadequate denture hygiene, especially constantly wearing dentures rather than removing them during sleep, is another risk factor for both oral candidiasis and Candida carriage. Dentures offer a relatively acidic, moist, and anaerobic environment for the reason that the mucous membrane covered by the dentures is protected from oxygen and saliva, which prevents or limits the growth of germs. Loose and poor-fitting dentures may also cause minor mucosal trauma which is thought to increase mucosal permeability and increase the ability of C. albicans to invade tissue. Dentures may therefore become covered with biofilm and act as reservoirs of infection, resulting in persistent re-infection of the mucosa [1-4]. Candida-associated denture stomatitis (CADS) is a chronic atrophic complication of the oral cavity that mainly affects people who wear removable dentures. Some have reported that up to 65% of denture wearers have this condition to some degree. Although this condition is also known as ‘denture sore mouth”, there is rarely any pain [5]. Candida is associated with approximately 90% of denture-related stomatitis cases [6]. Numerous evidence-based studies have revealed that Candida albicans is the major causative agent of denture stomatitis (DS), goes along by Candida tropicalis, Candida glabrata, Candida parapsilosis, Candida krusei, or other species as Candida stellatoidea, Candida pseudotropicalis, Candida famata, Candida rugosa, Candida geotrichium, Candida dubliniensis, and Candida guilliermondii [1-4, 7-9]. The untimely diagnosis of pathogenic fungal agents and the detection of their susceptibility to antifungal drugs are vital to the treatment of infection and the development of preventive healthcare-associated strategies [1,2,10,11].
Management of CADS is based on a broad-choice treatment strategy [12], which consists of detecting and eradicating potential significant risk factors, avoiding systemic Candida infection, and dipping any associated inconveniences. Use of oral preparations of antimicrobial agents, such as amphotericin B (AMB), nystatin (NYS), and miconazole (MIC), and systemic drugs, such as fluconazole (FCZ), voriconazole (VCZ), posaconazole (POS), itraconazole (ICZ), and ketoconazole (KTZ), has been revealed to be efficient in the treatment of CADS [13–16]. Echinocandins, such as caspofungin (CAS), are a class of antifungal drugs that appear to be highly effective against all species of Candida, including those that are less sensitive or are resistant to FCZ and/or ICZ [15]. Nevertheless, earlier studies have described recurrence and clinical relapse of CADS after treatment [17, 18]. Obtain sufficient information about the antifungal susceptibility testing (AFST) from Candida spp. participation in CADS may aid in the selection of alternative antifungal treatments for recurrent oral candidiasis.
Despite the lack of research on dental problems in Yemen in the past, there is a growing interest in dental problems nowadays as many studies have been conducted in cases of oral bacterial and fungal infections, drug resistance, tooth decay, causes of permanent tooth extraction, chemical drugs and Oral herbal [ 1-4, 19-33]. In Yemen, there have been several studies discussing biofilm formation, sensitivity to antifungals, and isolation of Candida from the oral cavity of denture wearers and free
dentures members, but no study has been found in determining MIC50 and MIC90 antifungal drugs for Candida albicans [1-4]. Therefore, in the current study, we identified the causative agents of CADS and an in vitro antifungal susceptibility test (AFST) to determine the MIC in Candida albicans and the rate of resistance to 5 selected antifungal drugs among Yemeni patients with CADS.
Study site and patient selection
The patients were selected from dental clinics in Al-Thawra Hospital, Al-Jumhouri Hospital, and some private dental centers in Sana'a, Yemen. The inclusion criteria for selecting the subject were healthy individuals with no clinical signs of Candida infection and no systemic disease. In addition, individuals who smoked or were currently taking antifungals, steroids, antibiotics, or immunosuppressive drugs in the past six months were excluded.
Sample Collection Process
After examination of the oral cavity, denture samples were obtained by scraping sterile swabs across the inner surface of the denture. In a 6-month period (1st January to end of June 2020), a total of 88 clinical isolates were collected from 79 patients aged 39–76 years with DS. For patients with stomatitis caused by Candida albicans (CADS) contained 13 (21.7%) males and 47 (78.3%) females, their ages ranged between 39-74 years (Table 1). All samples were streaked on Sabouraud dextrose agar and incubated at 35°C. for 7 days. All suspected colonies were detected by CHROM Agar Candida. Candida species were identified by the color of the colonies using the color reference guide provided by the manufacturer. When color determination was unclear, fermentation assay for sucrose, maltose, glucose, lactose-galactose was performed. Candida species has also been identified by the ability to produce Chlamydia spores on glutinous rice agar [33].
| Characters | Number | Percentage |
| Sex | ||
| Male | 13 | 21.7 |
| Female | 47 | 78.3 |
| Age groups | ||
| ≤40 years | 2 | 3.3 |
| 41-50 years | 16 | 26.7 |
| 51-60 years | 35 | 58.3 |
| >60 years | 7 | 11.7 |
| Total | 60 | 100 |
| Mean age | 53 years | |
| SD | 9.5 years | |
| Min | 39 years | |
| Max | 74 years | |
Table 1: The age and sex distribution of patients with Candida albicans-associated denture stomatitis (CADS) at a selected dental clinic in the city of Sana'a
Antifungal susceptibility testing
The in vitro activity of the antifungal agents against each isolate was determined by E-test (HiMedia, Mumbai, India) according to the manufacturer's instructions. E-test strips for fluconazole (FCZ; 0.016 ∼ 256 μg/mL), itraconazole (ICZ; 0.002 ∼ 32 μg/mL), voriconazole (VCZ; 0.002 ∼ 32 μg/mL), and amphotericin B (AMB; 0.002 ∼ 32 μg/mL) were used [34]. Interpretive sensitivity criteria for antifungal breakpoints were adapted from the Clinical and Laboratory Standards Institute (CLSI), [35]. The breakpoints used in C. albicans are: FCZ (S=2; SDD = 4; R ≥ 8); VCZ (S ≤ 0.12; R ≥ 1), ICZ (S= 0.12; R ≥ 1) and AMB (S =2; R > 2). For quality control, C. albicans (ATCC 10231) was used as a reference strain and tested simultaneously with clinical isolates.
Overall, C. albicans was the most commonly isolated species (n=60; 68.2%), followed by C. glabrata (n-9; 10.2%), C. tropicalis (n=7; 8%), and C. parapsilosis (n=3; 3.4%). 78.3% of the participants are females and only 21.7% are males. The age average ± SD for participants was 53 ± 9.5 years. Most of the subjects covered were in the age group 51-60 years (58.3%) followed by 41-50 years (26.7%). Table 3 shows, the In- vitro antifungal susceptibility of 4 antifungal agents against 60 Candida albicans isolated from Candida-associated denture stomatitis. Voriconazole had the lowest geometric mean minimum inhibitory concentration was 0.0418 ml for MIC50, and 0.957 ml for MIC90; followed by amphotericin B (AMB) in which MIC50 was 0.518 ml and for MIC90 was 1.06 ml.
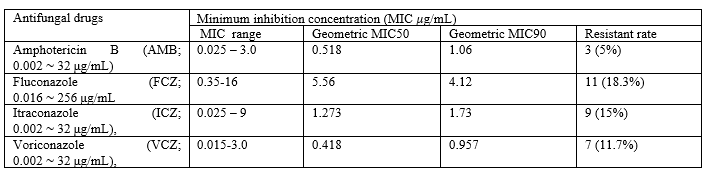
MIC50 = Minimum Inhibitory Concentration required to inhibit the growth of 50% of organisms. MIC90 = Minimum Inhibitory Concentration required to inhibit the growth of 90% of organisms. MIC range is the range of the lowest and highest MIC values obtained from 60 C. albicans isolates tested. Percentage resistance is the percentage of isolates resistant to a specific antifungal drug.
A complete denture (also known as a full denture or plate) is a removable device used when all the teeth inside the jaw are missing and need to be replaced with prosthetics. Unlike a partial denture, a full denture is created when there are no more teeth left in the arch and is therefore an exclusively tissue-reinforced prosthesis. In the current study, the mean age ± SD of the participants was 53 ± 9.5 years and ranged from 39 to 74 years. This result differs from that reported from Iran where the mean age of DS patients was 65 ± 7.5 years and the patients' ages ranged from 55 to 84 years. The younger age of Yemenis in these findings could be explained by the exposure of Yemeni patients to factors of tooth loss, such as: dental caries, periodontal disease, trauma, congenital disorders (such as ergogenesis imperfecta, hypomineralization of molar incisors) and functional impairment more than the Iranian population [36]. Dentures in the oral cavity serve as a reservoir of Candida spp. and, thus, it considered a predisposing factor for DS in denture patients, as well as a possible origin for re-infection [37]. In the current study, the dominant Candida species isolated from the mouth was Candida albicans with 58%. Other species were also isolated from the mouth; Candida glabrata from 9 patients (10.2%), Candida tropicalis from 7 patients (8%), and Candida parapsilosis isolated from 3 patients (3.4%). These results are similar to that reported by Samaranayake et al. and Lee et al. in which the most frequently identified species is C. albicans, although C. glabrata, C. guilliermondii, C. parapsilosis, C. krusei, and C. tropicalis are less commonly seen [38,39]. However, Bouquot et al. reported that C. tropicalis was the most common non-Candida albicans Candida (NCAC), followed by C. glabrata, while C. parapsilosis were rare isolated in oral colonization or as a cause of stomatitis [40]. As it is known Candida species may be able to metabolize ethanol and convert it into the carcinogen acetaldehyde, and can thus progress oral and upper gastrointestinal tract cancer. This means that our studied individuals under risk of oral and upper gastrointestinal tract cancer. Consequently, , greater emphasis should be placed on diagnosis and treatment of oral Candida albicans infections, also on other Candida species than C. albicans as recommended to prevent this development [41,42]. In agreement with other studies, the current research found that C. albicans, C. parapsilosis, C. tropicalis, and C. glabrata caused CADS [1, 2, 43-45] and recommended drugs in CADS patients without an underlying disease commonly includes a NYS suspension or a clotrimazole tablet. However, topical application of anazole, such as Fluconazole (FCZ or Itraconazole (ICZ), can also be used to prevent persistent or chronic fungal infections in the patients [34, 46]. Several studies reported the emergence of antifungal resistance to azoles, which has been associated with multiple episodes of recurrence [16, 47-49]. In the current study, 18.3% of C. albicans (11/60) was observed to be resistant to Fluconazole (FCZ). In contrast with the current study data, Abaci and Haliki-Uztan (2011) reported that 59.4% of C. albicans were resistant to Fluconazole (FCZ) [50].
| Candida species | Number | Percentage |
| Candida albicans | 51 | 58 |
| Candida glabrata | 9 | 10.2 |
| Candida tropicalis | 7 | 8 |
| Candida parapsilosis | 3 | 3.4 |
| Candida albicans+ Candida glabrata | 5 | 5.7 |
| Candida albicans+ Candida tropicalis | 4 | 4.5 |
| Total Candida albicans | 60 | 68.2 |
| Total Candida species | 88 | 100 |
Table 2: Distribution of different types of Candida species among Candida-associated denture stomatitis (CADS) isolated from 79 patients.
AMB, also used in the management of CADS, proved effective against Candida spp. [51]. Besides, the findings obtained in the present study were in agreement with the results of Wingeter et al. [52] regarding the susceptibility of oral Candida strains to AMB. In the current study, 5% of C. albicans (3/60) was observed to be resistant to Amphotericin B (AMB) as AMB-resistant C. albicans isolates were reported from several previous studies [50,53]. In the current study, 11.7% of C. albicans (7/60) was observed to be resistant to Voriconazole (VCZ). However, the geometric MIC90 was 0.957ml, for C. albicans, Omran et al. (2018) in Iran previously showed that the GM-MIC90 for Voriconazole (VCZ ) were 0.25/ml for C. albicans less than our findings [36]. Several other studies also demonstrated that Voriconazole (VCZ) was strong antifungal agents against Candida spp. [36, 54-57]. Other studies have shown that ITC is useful for treating patients with DS [37, 58, 59]. Dorocka-Bobkowska and Konopka (2007) reported that AMB, FCZ, and ICZ were effective against 100%, 88.7%, and 87.3% of C. albicans and less sensitivity rates equal to 79.6%, 71.4%, and 79.6% respectively for other Candida strains [12]. Our results showed that the tested antifungal showed good efficacy for most of the isolates. However, the observed variability between some of the isolates and drug resistance highlights the need for the AFST as a monitor to administer the therapeutic procedure.
In conclusion, Candida albicans was the most prevalent Candida species in Yemeni patients with CADS and was susceptible to both azoles and amphotericin B. In addition, Voriconazole could be a suitable alternative to antifungal agents currently used in the treatment of CADS, as well as in the treatment of recurrent Candidasis.
Also, the increasing rates of NCAC strains among CADS patients in Yemen should viewed as both novel and alarming. Extensive observational studies should be performed on all clinical specimens yielding significant growth of Candida spp. and the effect of resistance pattern on ICZ. As a consequence of selective pressure, emergence of drug resistance is inevitable. Therefore, future studies should focus on the emergence of drug-resistant Candida strains and their frequencies.
The authors thank the Faculty of Dentistry, Sana'a University, Sana'a, Yemen for their generous support in providing working space and materials.
Ethical approval
We have obtained written consent from all cases. Consent was obtained from the participants prior to sample collection. The study proposal was evaluated and approved by the Ethics Committee of the Faculty of Medicine and Health Sciences, Sana'a University.
No conflict of interest associated with this work.
All authors co-wrote the article and reviewed the results. Laboratory parts and data analysis were performed by Hassan Abdelwahab Al Shamahy.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
