
Research Article | DOI: https://doi.org/10.31579/2641-5194/017
*Corresponding Author: Alshymaa A. Hassnine, Gastroenterology and Hepatology Unit, Department of Tropical medicine, Faculty of Medicine - Minia University, Minia, Egypt.
Citation: Amr M. Elsayed, Elham Ahmed, Magdy Fouad, Alshymaa A. Hassnine (2021) In Corona Days; Performance Hardships for Suggested Endoscopist Location during Esophagogastroduodenoscopy. J. Gastroenterology Pancreatology and Hepatobilary Disorders. 5(1): DOI: 10.31579/2641-5194/017
Copyright: © 2021, Alshymaa A. Hassnine, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 17 January 2021 | Accepted: 01 February 2021 | Published: 23 February 2021
Keywords: COVID-19; EGD; UGI endoscopy; SARS COV2; PPE; China; EGD
Background and Aims: Corona virus disease COVID 2019 is considered as serious pandemic. Esophagogastroduodenoscopy (EGD) is an aerosol generating process and may precipitate its transmission. The aim of this study is to assess new location for the endoscopist and supporting team during this era of COVID19.
Methods: This study included 43 patients. Patients were classified into two groups, group 1 included 21 patients in which classic position of endoscopic staff members was done, maintaining the personal protective equipment and the group 2 included 22 patients in which the endoscopist and staff members stand behind the patient.
Results: There is no significant statistical difference between groups regarding the time needed for completing the endoscopic process, the success of the maneuver or the satisfaction of the patient about the maneuvers (P = 0.839, P = 1, P = 0.721) respectively, the endoscopist has to do additional movements by his shoulders or his wrists in group II more significantly than in group I (p=0.012)
Conclusions: Standing of the endoscopist behind the patient while performing EGD is as effective as the standard classic one. In simple upper gastrointestinal UGI endoscopic maneuvers, it may be more protective for endoscopic staff members in the era of pandemic COVID19.
A new coronavirus severe acute respiratory syndrome coronavirus (SARS COV2) outbreak leading to corona virus disease 2019 (COVID-19) has begun in Wuhan in December 2019, which has rapidly spread throughout China and beyond [1]. The World Health Organization (WHO) declared COVID-19 as pandemic on 11 March 2020, and the number of confirmed COVID-19 cases had increased to more than 372000 globally by 24 March 2020 [2].
Guan WJ et el., 2020 studied 1099 patients with COVID-19 from Wuhan and showed that typical clinical symptoms of COVID-19 included cough sore throat, fever, fatigue, and shortness of breath. More than 40% of patients had a history of contact with confirmed COVID cases and 56.2% had no fever [3]. Gastrointestinal symptoms aren’t uncommon but seem to be less common when compared with severe acute respiratory syndrome or Middle East respiratory syndrome [4]. Early studies from Wuhan reported that about 10% of cases presented with nausea and diarrhea few days just before the onset of fever and respiratory symptoms [5]. So, if only respiratory symptoms alone are screened, many cases with COVID-19 may be missed [6]. The overall mortality was about 1.4%, and the mortality increases with the severity of cases up to 22.4% in advanced cases [3, 7].
COVID-19 is mainly spread via droplets and close contact, but it is clear now that airborne spread is possible during aerosol-generating procedures (AGPs). In addition, strong evidence suggests that SARS-CoV2, that causes COVID-19 and known as the 2019 novel coronavirus, can be detected in the feces of patients [8] , leading to the possibility of transmission by feco-oral route [9,10].
Gastrointestinal endoscopies, especially those done through the nasal and oral cavities, EGD, may lead to cough and subsequent emission of droplets and increase the risk of exposure of the medical team, including endoscopists, nurses, and assistants, to aerosol contamination [11]. The risk of viral transmission may increase during a prolonged stay in a closed environment as in endoscopic room [12].
Endoscopy units are faced with great challenges during this pandemic as 3.8% of confirmed cases from China were healthcare personnel (HCP) with reported deaths. [13] Endoscopy is likely a high-risk procedure as pulmonary and gastric secretions, as well as fecal material, may contain large viral loads. Infection control measures must be applied to ensure patient safety, avoid nosocomial outbreaks, protect HCP, and ensure rational use of limited personal protective equipment (PPE)[14].
In this study, we want to assess new location for the endoscopist and supporting team during this era of COVID-19 to stand behind the patient instead of the classic position in the upper GI endoscopic maneuver to decrease the possibility of aerosol exposure during the practice of upper gastrointestinal endoscopy.
This study was done during the period from 21 march 2020 till 1st june 2020, involved 43 consecutive patients were coming to endoscopy unit of minia university hospital for doing urgent UGI endoscopy either presenting with mild attacks of GI bleeding, ingestion of foreign bodies, dysphagia, follow up of variceal ligation after recent variceal hemorrhage as an urgent 2ry prophylaxis, dyspepsia with alarm signs suggesting GI malignancy. patients with suspected COVID19, patients with massive bleeding, those need upper GIT stenting, or those need EMR, were excluded from the study, all routine diagnostic endoscopies, all surveillance and routine follow up were postponed.
Patients were randomly classified into two groups, the first group included 21 patients in which classic position of endoscopic staff members was done, maintaining the personal protective equipment (PPE) including a face mask; isolation gown with water resistance; eye protection [15] Standard hand hygiene procedures before and after each case should be performed Ethanol (62–71% concentration), 2% glutaraldehyde and 0.1–0.5%sodium hypochlorite are used as disinfectants [16]. The second group included 22 patients in which the endoscopist and staff members stand behind the patient, the endoscopic tower equipment was put in front of the patient and the scope channel was gently twisted over the patient to be handled by the endoscopist. The patient is monitored during the procedure, all patients received midazolam IV, the endoscopic procedure was done by Pentax video scope EG 2990 I and pentax video scope EG2990 K using light source EPK-I 5000.
Table (1) Shows the age of patients in group I (21 in number) in which the endoscopist stands in the classic position in front of the patient is ranging from 24 to 63 years, its mean is 38.7, age of patients in group II (their number is 22) in which the endoscopist stands behind the patient is ranging from 22 to 70 years, its mean is 37.8. As regarding sex, there are 11 females (52.4 %), 10 males (47.6%) in group I, in group II there are 11males (50%), 11 females (50%). No significant deference between group I and group II as regarding age and sex.

Significant level at P value < 0>
Table (2) shows different endoscopic maneuvers done in studied groups; esophageal variceal ligation was done in 13 patients (61.9%) in group I and in 15 ones (68.2%) in group II, gastric varcies injection was done in 3 patients (14.2%) in group I and in 3 patients (13.6%) in group II. Diagnostic endoscopy and biopsy was done in 5 patients (23.9%) in group I, and in 4 patients (18.2%) in group II.

(C) Chi Square test for qualitative data between the two groups
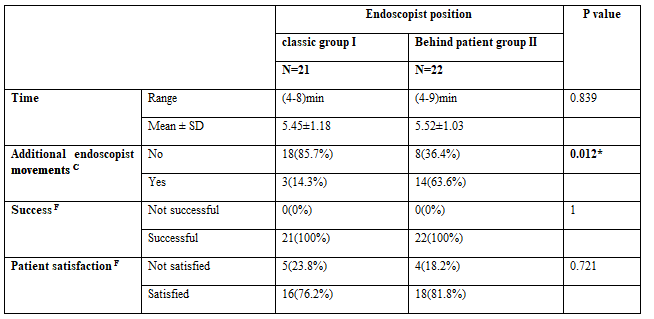
Table (3) shows that the taken time for the endoscopic procedure in group I is ranging from 4 minutes to 8 minutes, its mean is 5.45 minutes and that in group II is ranging from 4 to 9 minutes, average is 5.52, without significant statistical difference. in group I the endoscopist has to do additional movements either by his wrist or his shoulder to facilitate the maneuver in only 3 patients (14.3%) while in group II the endoscopist has to do additional movements by his wrist or his shoulder in 14 cases (63.6%) with significant statistical difference p=0.012. in both groups the endoscopist did the endoscopic maneuver with 100% success. As regard patient satisfaction, 16 patients (76.2%) in group I are satisfied versus 18 patients (81.8%) in group II with no significant statistical difference.
The present study designed to assess the new location of the endoscopist and the accompanying team behind the patient instead of the classic position in which the endoscopist stands in front of the patient in the practice of urgent EGD during the current time of era of pandemic COVID19 with preserving the standard precautions of infection control. This is supposed to do more limitations of the hazards of the generated aerosol resulted from the UGI endoscopy maneuver.
As it known that nearly all endoscopic procedures should be considered aerosol generating procedures (AGPs). Coughing and retching can occur during upper endoscopy, generating aerosols [17]. And so increase the possibility of transmission of COVID19 between the health care workers. We studied 43 patients who consulted for doing urgent EGD; 21 endoscopic maneuvers were done by the classic location of the endoscopic staff team maintaining standard precautions and 22 ones were done by changing the team location with careful monitoring of the patients with maintaining the standard precautions as we said. Most of cases were variceal hemorrhage due to the high prevalence of chronic liver diseases and portal hypertension in Egypt [18]. Other cases needed only screening upper GI endoscopy and may be biopsied if needed.
The time needed for completing the maneuvers in both locations nearly were the same also all maneuvers done using the new position were completed successfully as those done by the classic position 100% success but the endoscopist has to do additional movements using his wrist or shoulder to facilitate the work in about 63% of cases versus only 14% using the classic position.
The new location of the endoscopist has no effect on patient satisfaction by upper GI endoscopic process as no significant difference between the classic or the novel position regarding the patient satisfaction.
We conclude that standing of the endoscopist behind the patient while performing EGD is as effective as the standard classic one, we recommend it during simple UGI endoscopic maneuvers as it may be more protective for endoscopic staff members in the era of pandemic COVID19, for further studies either on larger scale of patients or on other different more complex UGI endoscopic techniques.
Abstract (text).
We would like to thank all the patients, controls who participated in this work. I hope that with this and other studies, we can alleviate their sufferings.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
