
Research Article | DOI: https://doi.org/10.31579/2639-4162/001
1 Department of Applied Nutrition, Faculty of Livestock, Fisheries and Nutrition, Wayamba University of Sri Lanka, Makandura, Gonawila (NWP), Sri Lanka.
2 Dr. Neville Fernando Teaching Hospital, Sri Lanka.
*Corresponding Author: AMNT Adikari, Department of Applied Nutrition, Faculty of Livestock, Fisheries and Nutrition, Wayamba University of Sri Lanka, Makandura, Gonawila (NWP), Sri Lanka.
Citation: Adikari AMNT, Madumali KAC, Perera ULDS, Improving Nutritional Status of Malnourished Bedridden Patient Diagnosed with Deep Vein Thrombosis and Pulmonary Embolism: A Case Study Approach. J General Medicine and Clinical Practice, Doi: 10.31579/2639-4162/001
Copyright: © 2018. Adikari AMNT. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 05 July 2018 | Accepted: 27 July 2018 | Published: 20 August 2018
Keywords: Bed ridden patients; Malnutrition; Nutritional management; Nutrition supplements
Malnutrition is common among hospitalized bed ridden patients. Nutritional management of hospitalized patients is a necessity in order to improve their nutritional status and disease conditions. The objectives of nutritional management of malnourished bedridden patient diagnosed with deep vein thrombosis and pulmonary embolism were to improve nutritional status of the patient through gradual provision of calorie and protein intake, to improve body protein status and control muscle wasting. Nutritional status was assessed by anthropometric, biochemical, clinical and dietary information. SGA was used to assess the malnutrition status of the patient. Since the patient was severely malnourished, she was fed with NG feeds followed by PEG feeds by gradually increasing calorie and protein up to the target level mainly through nutritional supplements for the one and half months of hospital stay. Patient’s serum protein, albumin levels and muscle mass were improved. According to the SGA, the patient was at normal/ well-nourished condition after nutrition management. Dietary management incorporating nutrition supplements indicated improvement of nutritional status of severely malnourished bedridden patient.
ASPEN: American Society for Parenteral and Enteral Nutrition
CRP: C - Reactive Protein
DRM: Disease Related Malnutriiton
DVT: Deep Vein Thrombosis
GI: Gastrointestinal
MNT: Medical Nutrition Therapy
MUAC: Mid Upper Arm Circumference
NG: Nasogastric
PE: Pulmonary Embolism
PEG: Percutaneous Endoscopic Gastrostomy
RFS: Refeeding Syndrome
SGA: Subjective Global Assessment
Disease-related malnutrition (DRM) is a highly prevalent disease within the hospital environment (Morán López et al., 2016). It is associated with a worse clinical outcome, longer hospital stay and higher costs (Bonilla-Palomas et al., 2016). Malnutrition leads to a range of poor clinical outcomes (Charlton et al., 2012). Malnourished patients who did not receive any nutritional intervention experienced further deterioration in nutritional status in the seven days following admission (McWhirter & Pennington, 1994). Malnutrition increases the risk of developing infection and pressure ulcers (Banks et al., 2010a). Improving nutritional status of these patients is essential for rapid cure, reduce hospital stay and reduce the cost.
Deep vein thrombosis (DVT) is the formation of blood clots (thrombi) in the deep veins. It commonly affects the deep leg veins (such as the calf veins, femoral vein, or popliteal vein) or the deep veins of the pelvis (Emeka et al., 2011). Despite adequate therapy, 1% to 8% of patients in whom pulmonary embolism develops will die, whereas others will experience long-term complications such as postphlebitic syndrome (40%) and chronic thromboembolic pulmonary hypertension (4%) (Scarvelis and Wells, 2006). Compared with DVT, pulmonary embolism is more often fatal, has a higher recurrence rate, and presents with less specific symptoms. Pulmonary embolism is usually a consequence of DVT (Wilbur and Shizan, 2012).
This case study focuses on nutritional management of hospitalized malnourished bed ridden patient with DVT and PE.
Materials and Methods
Case details: A 59 years old woman was diagnosed with deep vein thrombosis in left calf and bilateral pulmonary embolism. She had past history of right side arterio-venous malfunction, bronchial asthma, ischemic heart disease. She was unconscious at the time of admission. Before admission to the hospital, she had been admitted to another hospital and on NG feeds for two months.
Nutrition assessments
Anthropometric Assessments
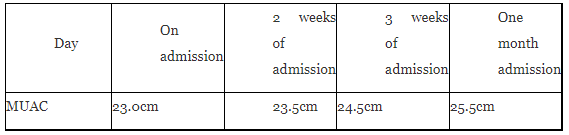
Estimated body weight and height were 50 kg and 153 cm, respectively and mid upper arm circumference (MUAC) was 23.0 cm. Changes of MUAC throughout the hospital stay is shown in table 1.
Biochemical Assessments
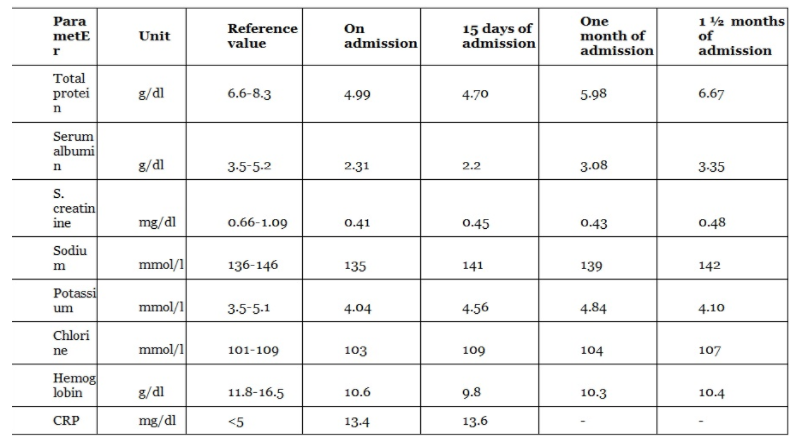
Biochemical parameters of the patient were taken before and during the nutritional management is shown in table 2.
Clinical Assessments
The patient was unconscious. Edema was not present throughout the hospitalized period. Clavicle and Acromion bone region muscles and interosseous muscles of dorsal hand were wasted.
Dietary Assessments
She could not take food orally. She was on NG feeds at the time of hospitalization. She had recurrent vomiting and less food intake since two months.
Medical management (Drugs):
Omeprazole, FeSO4, Warfarin, Meropenem, Metoclopramide
Nutrition diagnosis
This patient was severely malnourished related to poor food intake for about two months as evidence by SGA nutrition assessment (annexure 1),
reduced serum albumin and protein levels and reduced mid upper arm circumference which was closer to margins of cut off value (<22.0 cm). The patient is slightly anemic as seen by her hemoglobin levels.
Goals of MNT
Dietary management during the hospital stay
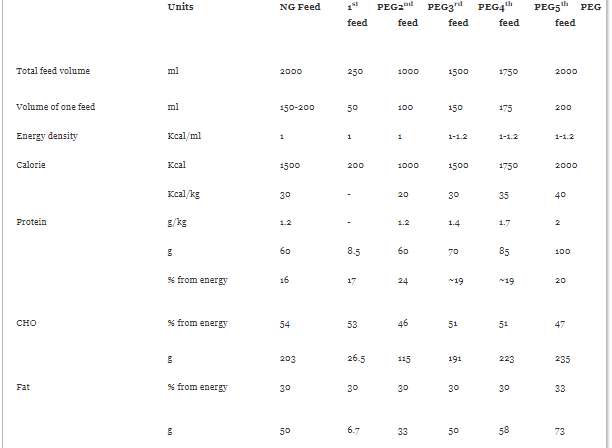
The patient was at risk of refeeding syndrome since she was in malnourished category and did not have adequate food intake for a long time. The targeted calorie and protein requirement was 2000kcal and 100g (2g per kilo gram of body weight), respectively. But, enteral nutrition was recommended starting with low amount of calorie and protein in order to prevent from refeeding syndrome. Gradually, energy and protein levels were increased up to the target. On the day of admission usual hospital NG feeds were given and patient specific NG feeds were started from second day. After one week of NG feed PEG feeds were started and continued by gradually increasing energy and macro nutrients as show in table 2.
Initially, the patient was fed with patient specific NG feeds with follow up supervision of the dietitian. Since she had tolerated usual hospital NG feed with 1000 kcal energy, 1g/kg of body weight protein, and 200 ml volume per feed, her NG feed contained 1500 kcal per day and volume per feed was 150-200ml. Energy density was maintained as 1 kcal /ml and protein given as 1.2 g/kg of body weight. Her normal energy requirement was given with higher protein content with this NG feed. Energy and protein intake was increased gradually, since she needs high energy and protein to recover from malnutrition.
She was fed with two hourly from 6.00 am to 12.00 pm with ten feeds. Fluid intake was decided by discussing with physician and observing her urine output. Around 2000 ml of fluid could be given to her from feeds and part of that fluid was given with the feeds and remaining was given as water.
After one week of admission, PEG feeding was started. 1st PEG plan was started with very low feed volume and energy level. Since PEG tube was inserted at around 12.00 pm, feeding was started after about 4 hours of insertion and only five feeds could be given on that day. Initial feeding volume was 50 ml and the patient was closely monitored to check the tolerability of the feed. From the 2nd day onwards of the PEG insertion, ten feeds were given for a day. Fluid volume was increased as 50ml, 100 ml, 150 ml, 175 ml and finally 200 ml. Along with increased fluid volume, calorie level was gradually increased as 200 kcal, 1000 kcal, 1500 kcal, 1750 kcal and finally 2000 kcal was continued until patient gets complete recovery. Energy density was maintained as 1kcal/ ml or less in initial feeds and it was 1-1.2 kcal/ml in last feeds. Initially protein was given as 1.2 g/kg of body weight with NG feed and 2nd PEG feed. Thereafter, it was increased gradually as 1.4 g/kg, 1.7 g/kg and finally 2g/kg was continued until the recovery.
Nutrition supplements were suggested as main food item in all the meal plans. Only two or three kitchen feeds were given for a day and rest were given by nutrition supplements. High energy formula (Pentasure (2.0) and sustacal) were suggested as nutrition supplements for the patient since they are specially produced for the patients who need high calorie amounts.
There was a negative nitrogen balance due to high protein catabolism than protein synthesis. Her CRP level was not much high (~13.6). Therefore serum albumin level was taken as an indicator of body protein status. Her serum albumin and total protein levels were lower than normal values on admission. Gradual increase of dietary protein level was effective to reach the target protein intake (2 g/kg). Her improvement could be observed by increased serum albumin levels and mid upper arm circumference in 15 days period (See 2). Serum albumin level was increased from 2.31 to 3.08 after one month and to 3.35 after 1 ½ months of admission as shown in figure 1.

Improvement of serum total protein level is shown in figure 2.

The mid upper arm circumference was increased from 23 cm to 25.5 cm after one month of admission through nutrition care process ( see table 1). This indicates that the patient’s body protein level has been increased to normal range and muscle mass has been increased by provision of high protein and high calorie diet. Patient was in normal/ well-nourished category according to the SGA after nutrition management (annexure). Patient was conscious and started to take foods orally after one and half months nutritional care process.
Many studies have shown that patient outcomes can be improved with adequate nutrition support (Smedley et al., 2004). There is a large and growing body of evidence to show that nutrition support is effective and leads to improved nutritional status and clinical outcomes in malnourished patients. Adequate nutrition is essential to the bed ridden malnourished patients to help anabolism and control catabolism to maintain proper immune system and speed up disease recovery. If dietary intake is not able to meet requirements, oral supplementation is the next line of treatment, followed by tube feeding and finally, if the gut is not working and there is contraindication to feed enterally, parenteral nutrition can be explored (Thomas, 2001). The patient was hemodynamically stable and had a functioning gastrointestinal tract. Thus enteral nutrition was best to provide adequate nutrition to her.
Subjective Global Assessment (SGA) is well accepted as an assessment tool in clinical practice (Lochs et al., 2006). It has been regarded by ASPEN as the best nutrition assessment tool and one of the only two tools (the other one being MNA) recognised as an assessment tool (A.S.P.E.N. Board of Directors and the Clinical Guidelines Taskforce, 2002). It is an easy, non-invasive and inexpensive tool for widespread use by trained clinicians or dietitians (Keith, 2008). Subjective Global Assessment has been widely accepted and used as a diagnostic tool for malnutrition, to track clinical outcomes and as a reference standard to validate nutrition screening tools (Steenson et al., 2013). Hence SGA was the tool that used to assess malnutrition of the patient. This patient did not have any chronic disease condition related to the diet but she was severely malnourished as assessed by subjective global assessment (SGA). Hence nutrition management was focused towards improvement of her nutrition to correct malnutrition condition, micronutrient deficiencies with improved immune system and improve body protein status.
Diet plans were prepared to avoid over feeding, provide adequate energy, protein, carbohydrates, vitamin, mineral and fluids as her requirements. All nutrients were provided gradually by observing her improvements of conditions and clinical features. She requires high amount of energy, protein and other macro and micronutrients. But, they cannot be given suddenly because of refeeding syndrome (RFS). RFS may occur usually in malnourished patients undergoing re-feeding after a period of under nutrition (Rio et al., 2013). Hospitalized patients with risk of malnutrition demonstrate significant risk of RFS (Pourhassan et al., 2017). As malnutrition is the main risk factor for RFS, routine malnutrition screening should also screen for risk of RFS (Boland et al., 2013). The syndrome is complex and may feature hypophosphatemia, abnormal sodium and fluid balance; changes in glucose, protein and fat metabolism’ thiamine deficiency; hypokalemia and hypomagnesaemia (Mehanna et al., 2008). Therefore it was suggested that this patient is at risk of RFS anf energy and all the nutrients were provided gradually.
During feeding tolerance was determined by physical examination, passage of stool and vomiting conditions. GI intolerance is usually defined by vomiting, abdominal distention, complaints of discomfort, high NG output, high GRV, diarrhea, reduced passage of flatus and stool, or abnormal abdominal radiographs (ASPEN, 2016). If the patient do not tolerate the feed, diarrhea and vomiting can be occurred. Initially she had diarrhea, but after one- two days she tolerated the feed since she was given metoclopramide drug. Metoclopramide drug was very much important to tolerate the feed for the patient. Metoclopramide increases the lower oesophageal sphincter pressure, gastric tone, forward peristalsis of the stomach and the duodenum, while simultaneously decreasing pyloric sphincter pressure. These mechanisms accelerate gastric emptying, reduce gastric stasis and residual volume, and thus decrease gastroesophageal reflux (Warusevitane et al., 2014). This reduced the vomiting condition of the patient and helped to patient to tolerate the feed.
Protein is very important to increase the response of immune system, increase muscle mass which loss during illness and prevent from protein energy malnutrition. If patient do not receive adequate protein, she may be at risk of getting infections, increased synthesis of acute phase proteins (CRP, Fibrinogen), reduced gut functions muscle wasting and decreased functions of respiratory muscles (Hoffer & Bistrian, 2014). In the final meal plan she was given 2 g/kg of protein and was continued without further increment. Protein requirements are expected to be in the range of 1.2–2.0 g/kg actual body weight per day in critically ill patients except in burn or multitrauma patients. Providing proteins higher than 2 g/kg per day do not give additional benefits unless in burn or multitrauma patients (ASPEN, 2016). Therefore final protein level was 2 g/kg/ day and continued until complete recovery by observing renal function. Serum creatinine, blood urea nitrogen, uric acid levels were assessed to know the protein metabolism in the body and to measure whether the protein intake is excessive for the patient. Carbohydrates and fat was given as normal requirements in initial meal plans. After that fat content was little increased with reduced carbohydrate level. Fat is a good source of energy dense foods. Energy dense foods are very important to patients who are fed with enteral nutrition in order to provide adequate nutrition along with given fluid amount.
Studies have shown that judicious use of nutrition supplements can improve weight, protein and energy intake, nutritional status, physical function, quality of life and length of stay in acute care (Dietitians Association of Australia, 2009)
Nutrition supplements are the best sources to provide adequate nutrition for tube feeding patients. Supplements contain almost all the macronutrients and micronutrients in correct proportions. The osmolality of supplements are similar to the blood osmolality value which is around 300 mOsm /kg and 300-350 mOsm /kg in supplements are considered to be iso-osmolar. As well as these products have been produced under hygienic conditions and it requires less contribution to be prepared and give to the patient. Then the risk of contamination is less when compared to kitchen feeds. The risk of getting infection is high with kitchen feeds since they are prepared under less hygienic conditions. Further the osmolality cannot be controlled and measured in those kitchen feeds and normally osmolality value is high in them. All the nutrients in the food cannot be extracted to the feed though it is blended and filtered. Hence the energy density and nutrient content is low in kitchen feeds and unable to provide required nutrition with given feed volume. With the consideration of all these reasons, supplements are the best source to provide adequate nutrition for patients.
This is one of the few cases that reports the applying the nutrition care process for malnourished bed ridden patient. Energy, protein, feeding mode, feeding volume, tolerability, refeeding syndrome, type of food sources were several factors to be considered when planning nutrition care process for these people. Nutritional status of malnourished patient of this case was improved along with high energy and high protein diets provided mainly by commercial nutrition supplements through enteral feeding.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
