
Case Report | DOI: https://doi.org/10.31579/2690-4861/481
Department of Medical Oncology, Université de Genève, Hôpitaux Universitaires de Genève, Geneva 1205, Switzerland.
*Corresponding Author: Lorenzo Francini, Department of Medical Oncology, Université de Genève, Hôpitaux Universitaires de Genève, Geneva 1205, Switzerland.
Citation: Lorenzo Francini, Rita Brito, Eugenio Fernandez, Petros Tsantoulis and Daniele Frisone, (2024), Impressive response to Pralseltinib in KIAA1468 RET-fusion anaplastic thyroid cancer: a case report and literature review, International Journal of Clinical Case Reports and Reviews, 18(1); DOI:10.31579/2690-4861/481
Copyright: © 2024, Lorenzo Francini. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 25 May 2024 | Accepted: 03 June 2024 | Published: 19 June 2024
Keywords: RET fusion; pralsetinib; selpercatinib; anaplastic thyroid cancer; KIAA1468-RET fusion
Anaplastic thyroid carcinoma (ATC) is a severe, aggressive form of cancer with low survival rates. Multimodal therapies are currently employed with limited success and targeting molecular subgroups of ATC, such as those with RET translocation, is an active area of research.
In this case report, we present a patient with metastatic ATC harboring a RET translocation, treated with two RET-specific tyrosine kinase inhibitors (TKIs), Pralsetinib and Selpercatinib. Pralsetinib resulted in a significant and rapid reduction in lung metastasis complicated by a pneumothorax effects.
The initial efficacy of Pralsetinib in our patient underscores the potential of RET-specific TKIs in the management of RET-altered ATC and highlights the risk of adverse events associated with tumor response in high tumor burden diseases. Meticulous management of side effects remains essential to improve patient outcomes.
Anaplastic thyroid carcinoma (ATC) is an undifferentiated tumor of the follicular epithelium of the thyroid. It represents 1-2 % of thyroid malignancies and is one of the most aggressive malignancies. Its incidence in Europe is stable over time (< 0.3/100,000) [1]. It is more frequent in older age with a higher prevalence in the femalesex and in areas of endemic goiter.About 80% of patients have locally advanced disease at diagnosis, and almost half have distant metastases, especially in lung, bone, and brain. The median survival from diagnosis is 5 months and less than 20% of patients survive at 1 year [2].
It is assumed that ATC derives from well-differentiated thyroid cancer as papillary thyroid cancer following a carcinogenic multistep process. This is supported by a coexisting or a history of well- differentiated thyroid cancer in patients with an ATC. Moreover, mutations in BRAF and RAS genes are the most frequent alterations observed in both PTC and ATC. In the opposite TP53, TERT promoter and PI3K mutations are much more frequent in ATC than PTC and seem therefore essential for anaplastic transformation from PTC [3-6]. NTRK is another possible target in thyroid cancer, with a general frequency of rearrangement of about 3% of all thyroid carcinomas [7]. A pooled analysis of 28 patients with NTRK fusion-positive thyroid cancer across two trials of larotrectinib, including 7 with ATC showed an ORR of 29% in this population [8].
RET rearrangement is observed in 4-7% of non-medullary differentiated thyroid cancers but are relatively rare in ATC [9] [14-16]. RET fusion-positive thyroidcancers are associated with more frequent recurrence and shorter survival. Twenty-four different RET fusions are identified in RET fusion-positive thyroid cancer with CCD6-RET and NCOA4-RET being the most frequent [18]. RET fusions result in a RET protein with a constitutive tyrosine kinase domain activation and oncogenesis [10].
RET encodes a transmembrane receptor protein with an intracellular tyrosine kinase domain that is involved in the MAPK and PI3K-AKT signaling pathways [12,13]. There are two main categories of RET abnormalities: point mutations and RET gene fusions. Point mutations are primarily found in the kinase and cysteine-rich domains and observed in sporadic or in MEN2 syndrome associated medullary thyroid cancer (MTC) [7,8].
Selective RET thyrosine kinase inhibitors (TKI) are an effective approach for RET-driven tumors since 2010. While Lenvatinib and Sorafenib for DTC, and Cabozantinib and Vandetanib for MTC are all treatments FDA approved in case of progressive diseases, with a significant increase of PFS, they have not been proved useful ATC [7].
Selpercatinib and Pralsetinib are both potent, orally bioavailable selective RET-specific TKI with a similar action on docking the ATP-binding pocket [19]. The LIBRETTO-001 phase I/II trial assessed the selpercatinib overall response rate in patientswith thyroid tumorsharboring a RET abnormality. In RET fusion-positive thyroid cancer subgroup (19 patients), the response rate was 79% and 1-year progression-free survival was 64% [16]. In the ARROW multicohort phase I/II trial, a response was reported in 8 of 9 RET fusion-positive thyroid cancer (89%) treated with pralsetinib [6]. In these two pivotal studies, ATC were substantially under-represented 2 cases with RET fusion in LIBRETTO 001 and no cases in ARROW trial) [15]. The two cases described reported a remarkable response lasting 18 et 19 months respectively [14,17].
We present here the case of an 84-year-old woman who experienced sudden onset of dysphonia in September 2022. She described a decline in appetite, and physical examination revealed a palpable mass in the left cervical region. Initial imaging with a CT-scan showed a substantial thyroid tumor on the left side, which was invading the proximal oesophagus.Additionally, approximately 30 pulmonary metastases were identified with the biggest measuring more than 7 cm. There was no evidence of metastases in either the bone or abdominal regions. A surgical thyroid biopsy confirmed the diagnosis of metastatic anaplastic thyroid cancer resulting from a papillary thyroid cancer (Figure 1).
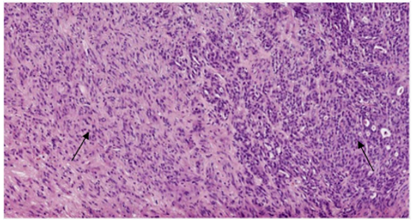
Figure 1: Component of anaplastic thyroid carcinoma (left) and papillary carcinoma (right)
After discussion with the patient, we administered decompressive radiotherapy for complete dysphagia at a dose of 70 Gy (2 Gy/d for 35 days) until 30.11.2022, with minimal clinical benefit leading to gastrostomy placement.
Molecular analysis identified a RET translocation (KIAA1468-RET fusion) associated with TP 53 (p. Glu286Lys) and NOTCH2 (p. Pro6ArgfsTer27) pathogenic mutations. No BRAF, RAS or TERT mutations were observed andDNA mismatch repair proteins were preserved (PMS2, MLH1, MSH2 et MSH6). Based on these results, we started a treatment with Pralsetinib administered through percutaneous endoscopic gastrostomy starting on the 28th of December 2022. During the 2 weeks following the treatment introduction, we observed a rapid favourable evolution with an improvement of dysphonia and dysphagia and a subjective size reduction of the thyroid mass.
On January 24th, one month after the treatment introduction, the patient described an acute dyspnea with a hypoxia while breathing ambient air. A CT-scan showed a right pneumothorax and pulmonary lung metastasis shrinkage and excavation. The pneumothorax was deemed secondary to lung metastasis necrosis and excavation (Figure 2). Pneumothorax was treated by chest tube placement and a pleurodesis. Subsequently the patient presented numerous complications, possibly linked to the oncological treatment, specifically a bacterial pneumonia with Klebsiella Pneumoniae and Pseudomonas Aeruginosa complicated by a heart failure and a Herpes simplex 1 stomatitis. For this reason, Pralsetinib was suspended from 27.01.2023 to 01.02, then reintroduced from 02.02 to 06.02.2023. Since a co-existing drug-induced pneumonitis could not be excluded, given the clinical improvement following the introduction of corticosteroids and CT imaging, the treatment was stopped on the 07.02.2023.

Figure 2: Right pneumothorax secondary to necrosis and reduction of pulmonary metastasis after 1 month on Pralsetinib
A thoracic CT scan performed on 28.02.2023 showed a resolution of the ground glass infiltrates but, on the other hand, oncological disease progression with an increase in size of multiple nodules and necrotic central lung masses.
Due to different toxicity profile, the initial target treatment was replaced by Selpercatinib, another receptor tyrosine kinase RET inhibitor, that was started on 01.03.2023 twice daily 160mg. After a rehabilitation period, the patient could be discharged in April 2023, but deceased after one month for undetermined reasons.
In our case, Pralsetinib administered by gastrostomy was highly effective, leading to a rapid shrinkage of target lesions easily visible on a simple chest X-ray (Figure 3) and confirmed at CT scan (Figure 2).
The RET fusion identified in our study is rare, previously described in only one other article [20].

Figure 3: Chest x-ray. Shrinkage of lung metastasis during the first month of Pralsetinib
After a relatively brief pause with the first RET inhibitor, Pralsetinib, the disease progressed rapidly (Figure 4), and another biopsy was not clinically indicated. The introduction of a second RET inhibitorfailed to elicit a clinical response, and we lack insights into the resistance mechanisms that could have led to this progression upon rechallenge with a second RET inhibitor. Although literature on this topic is limited, analyses of case series in thyroid and non-small cell lung cancers [21] suggest that additional RET mutations or MAPK pathway activation at various levels are the primary mechanisms of resistance [22].

Figure 4: Chest x-ray. Progression of lung metastases after 1 month without RET inhibitors
In an area scarcely covered in the medical literature, we aimed to present our case to highlight the remarkable effectiveness of RET inhibitors in such scenarios, demonstrating significant tumor reduction alongside notable serious complications that must be addressed. Our literature review and case study revealed multiple insights.
A dose-escalation (“ramp-up”) strategy for initiating RET inhibitors may offer a viable approach for patients with extensive tumor burden. This personalized dosing method could provide a safer and more effective treatment administration, underscoring the need for adaptable therapeutic strategies in managing RET-rearranged anaplastic thyroid cancer.
To our knowledge, this is the first documented instance of using RET inhibitors through a gastrectomy, and this administration method has shown effectiveness.
However, there remains much to understand about overcoming resistance to RET inhibitors. Due to the rarity of this condition, a definitive treatment algorithm has not been developed, and other targeted therapies do not appear universally effective.
This case underscores the need for ongoing research and multidisciplinary efforts to optimize treatment strategies for patients with RET-rearranged cancers.
We thank the patient and her family for accepting publication of this case report in an anonymous way, contributing to science developing in this field.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
