
Review Article | DOI: https://doi.org/10.31579/2768-2757/157
Medical microbiology department /College of Health Sciences/ Hawler Medical University/ Kurdistan region /Erbil/Iraq.
*Corresponding Author: Fattma A. Ali., Medical microbiology department /College of Health Sciences/ Hawler Medical University/ Kurdistan region /Erbil/Iraq.
Citation: Fattma A. Ali, Ahmed Akil Khudhair Al-Daoody, Solin Shahab Ahmed, (2025), Impact the Influence of Immunotherapy on Cancer, Journal of Clinical Surgery and Research, 6(1); DOI:10.31579/2768-2757/157
Copyright: © 2025, Fattma A. Ali. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 02 December 2024 | Accepted: 18 December 2024 | Published: 03 February 2025
Keywords: immune system and immunotherapy; necessity of immunotherapy; testing; typing of immunotherapy; side effects
Immunotherapy is a treatment that uses certain parts of a person’s immune system to fight diseases such as cancer, when the immune response is not strong enough to recognize cancer cells or signals are produced by cancer cells that make the immune system unable to attack them or the cancer cells escape from the immune system. Immunotherapy helps the immune system to destroy cancer. Immunotherapy can be useful for a few types of cancer, but it is not suitable for all types of cancers. Immunotherapy can be used on its own(alone), or in combination with other treatments such as chemotherapy, surgery, or radiotherapy. This review article emphasizes the pivotal role that advancements in cancer immunotherapy's history have played in establishing treatments that are now considered standard of care and delineates several primary strategies employed in the field of cancer immunotherapy (cancer vaccines, adoptive cellular immunotherapy, immune checkpoint blockade, and oncolytic viruses, Immunomodulators).
In contrast to prior benchmarks of treatment (such as radiotherapy, chemotherapy, and surgery), cancer immunotherapy has yielded substantial advancements in both survival rates and overall well-being for cancer patients. Immunotherapy has emerged as an innovative cornerstone in cancer treatment (Esfahani et al., 2020). Agents are utilized in cancer immunotherapy to stimulate or enhance the immune system's activation to combat cancer cells via intrinsic mechanisms, many of which are circumvented as the disease advances (Riley et al., 2019). The goal of cancer immunotherapy is to activate a patient's T-cells so that they can attack and kill malignancies. Amazing recovery stories abound, with individuals remaining cancer-free for years after receiving the treatment. Although using immune cells to combat cancer is not new, scientists have recently accumulated enough clinical evidence to show how transformative cancer immunotherapy can be. Because this field is not without its challenges, the future seems bright (Meiliana, Dewi, and Wijaya, 2016). "immunotherapy" refers to the application of substances that suppress or restore the immune system's capacity to defend against and prevent illness. A balance is maintained in the immune system so that cancer cells can be eliminated without unchecked autoimmune inflammatory responses, which are detrimental to the efficacy of immunotherapies and represent one of their therapeutic limitations. Innate immunity is restricted to the activation of non-specific immune responses by releasing cytokines that recruit immune cells to begin the non-specific immune response (Abbott and Ustoyev, 2019). For cancer immune therapy, these are exciting times. After years of poor results, the tide has finally turned, and immunotherapy has been clinically approved for various malignancies. Cancer vaccines, oncolytic viruses, adoptive transfer of ex vivo activated T and natural killer cells, and administration of antibodies or recombinant proteins that either co-stimulate cells or block so-called immune checkpoint pathways are all examples of immunotherapeutic techniques. The recent success of certain immunotherapeutic regimens, such as monoclonal antibody blocking of cytotoxic T lymphocyte-associated protein 4 (CTLA-4) and programmed cell death protein 1 (PD1), has accelerated the development of this therapy modality, resulting in the rapid creation of novel therapy targets and schemes that combine multiple immunological agents(Farkona, Diamandis and Blasutig, 2016). Controlled modulation of the immune system continues to be a significant obstacle in the widespread application of immunotherapies for cancer, given that these treatments induce severe adverse effects such as autoimmunity and nonspecific inflammation. Gaining insight into methods to enhance response rates for different categories of immunotherapy is crucial for optimizing effectiveness and managing these detrimental effects (Riley et al., 2019).
The Immune System and Immunotherapy
The immune system has created a range of intricate processes to identify and eliminate cancer cells(Kennedy and Salama, 2020).By distinguishing between self and non-self, the human immune system safeguards the body against both exogenous and endogenous pathogens. The immune system, which is comprised of white blood cells and lymphatic system organs and tissues (thymus, spleen, tonsils, lymph nodes, lymph vessels, and bone marrow), recognizes and eliminates numerous threats to maintain homeostasis. To comprehend how immunotherapy has become a cornerstone of cancer treatment, one must know the interaction between cancer cells and the immune system An objective of immunotherapy is to maintain immune system equilibrium so that cancer cells can be eliminated without unchecked autoimmune inflammatory responses, which are detrimental to the efficacy of immunotherapies (Abbott and Ustoyev, 2019).
Necessities of Immunotherapy
Immunotherapy for the treatment of cancer is a critically important and validated method. In light of the substantial research and clinical investigation endeavors devoted to the advancement of endogenous and synthetic immunotherapy strategies, it is imperative to concentrate on fundamental inquiries and delineate obstacles impeding both fundamental comprehension and clinical advancement. From identifying the most effective combinations of immune-based therapies for a given patient to overcoming a lack of confidence in the translation of preclinical findings, here we identify ten of the most significant obstacles that cancer immunotherapy must overcome (Hegde and Chen, 2020).
Ten Key Challenges of Immunotherapy
Testing
Numerous studies provide empirical evidence in favor of the hypothesis that immunotherapy exhibits heightened efficacy when applied to tumors that are highly mutagenized. Immunotherapy has significantly transformed the landscape of cancer treatment with immune checkpoint-based therapy experiencing especially rapid advancements. However, the efficacy of these immunotherapies is limited to a fraction of patients. As a result, patient selection is critical to prevent treatment-associated toxicity and expense for patients who are likely to gain any benefit. The establishment and verification of dependable surrogate biomarkers that can forecast clinical benefit or offer an early indication of response will be necessary for this purpose. Numerous ongoing initiatives are focused on the identification of predictive biomarkers for immune checkpoint therapy (Farkona, Diamandis and Blasutig, 2016).
Types of Cancer Immunotherapy
1-Immune checkpoint therapy
2-T-cell transfer therapy
3-Monoclonal antibodies
4-Oncolytic virus immunotherapy
5-Immunomodulators
6-Cancer vaccines
The recent success of immune checkpoint therapy, which uses antibodies to block the CTLA-4 and PD-1 pathways to treat cancer patients, is due to the elucidation of mechanisms underlying cancer immune regulation (Yang, 2015). CTLA-4 isn't the only checkpoint being studied by scientists and drug makers. Drugs that block a particular checkpoint, PD-1, seem to be more successful and have fewer side effects than Ipilimumab (anti-CTLA4 drug), according to early trials (Meiliana, Dewi and Wijaya, 2016). The accumulation of evidence about immune checkpoint inhibitors indicates that their efficacy is not universal, but rather restricted to certain subpopulations of cancer (Igarashi and Sasada, 2020).

Figure 1: Blockade of immune checkpoints to enhance T cell responses. After T cell activation, T cells express immune checkpoints (Basudan, 2022).
Particularly during the equilibrium phase, T cells play a crucial role in regulating tumor development throughout the immunoediting process(O’Donnell, Teng and Smyth, 2019). Regarding the treatment of cancer, immunotherapy represents an extraordinary clinical development. Current immunotherapies for cancer, such as immune checkpoint inhibitors and adoptive cell therapies, rely heavily on T cells for their effectiveness. T cell exhaustion, a hypofunctional state distinguished by a gradual decline in the ability of T cells to renew themselves and execute effector functions, is, nevertheless, a correlation with cancer. Considered a pathway of resistance for cellular immunotherapies, the "un-exhaustion" of T cells in the microenvironment of the tumor is widely recognized as a crucial mechanism by which immune checkpoint inhibitors function. Insights into the transcriptional and epigenetic mechanisms that regulate T-cell exhaustion have been illuminated by several elegant studies (Chow et al., 2022).

Figure 2: T-cell transfer therapy (Kruger et al., 2020).
There are two types of T-cell transfer therapy
A-Chimeric Antigen Receptors
Therapeutic applications of chimeric antigen receptor (CAR)-T cells are revolutionary due to the remarkable efficacy and durability of the results. CARs are synthetic receptors that have been engineered to redirect lymphocytes, predominantly T cells, to identify and eradicate cells that express a particular target antigen. The binding of CARs to target antigens that are expressed on the cell surface occurs in a manner that is not reliant on the MHC receptor. This leads to robust T-cell activation and potent anti-tumor responses. In 2017 the Food and Drug Administration (FDA) of the United States approved anti-CD19 CAR-T cell therapy in response to its extraordinary efficacy against B cell malignancies. Life-threatening CAR-T cell-associated toxicities, limited efficacy against solid tumors, inhibition and resistance in B cell malignancies, antigen escape, limited
persistence, poor trafficking, and tumor infiltration, and an immunosuppressive microenvironment are significant limitations of CAR-T cell therapy that remain to be addressed. Furthermore, to accommodate the demands of this expanding and dynamic industry, it is imperative to establish educational initiatives that provide workforce training. To increase antitumor efficacy, expand clinical efficacy, and reduce toxicities, numerous strategies have been suggested, such as combining CAR-T cell therapy with other anticancer therapies or employing novel CAR engineering techniques. This review examines recent advancements in CAR-T cell engineering that aim to enhance clinical effectiveness against solid and hematological tumors. It also addresses approaches to surmount existing obstacles, such as CAR-T cell-associated toxicities, antigen evasion, tumor infiltration, the immunosuppressive microenvironment, and tumor infiltration (Sterner and Sterner, 2021).

Figure 3: Chimeric antigen receptors therapy (Maru, Nadeau and McKeague, 2021).
BTumor Infiltrating Lymphocytes Immunotherapy
In contrast to other types of cancer, the clinical success of immune checkpoint blockade (ICB) for cancer has redirected interest toward tumor-infiltrating lymphocytes (TILs). In cancer patients, the efficacy of immune checkpoint inhibitor therapy has been associated with the magnitude and quality of T cell, NK cell, and, more recently, B cell responses in the tumor microenvironment. The examination of TIL gene expression profiles and clonality using cutting-edge single-cell analysis has unveiled an exceptional level of cellular heterogeneity, as well as discernible patterns of immune activation and exhaustion. Consistent with the broad clinical responses, a number of these states are standardized across tumor types. Notwithstanding this similarity, how various cancer types with comparable TIL landscapes react to immunotherapy differs, underscoring the intricate nature of the tumor-immune interactions that
lie beneath. Additionally, this observation is complicated by the substantial prognostic advantage of TILs observed in tumor types that have exhibited inadequate response to immunotherapy thus far. Thus, although there is a growing recognition of the importance of unifying single-cell-level lymphocyte infiltration and dysfunction, the investigation into biomarkers that predict response and prognosis is still in its early stages. It is now indisputable that the presence, activation, and stimulation of all lymphoid components of the immune system—CD8+ T cells, CD4+ T cells, B cells, and innate lymphoid cells—are essential for a successful antitumor immune response. This is demonstrated in particular by the identification of tertiary lymphoid structures (TLSs), which are clusters of TILs that are exceptionally well-organized and generate an advanced immune response (Paijens et al., 2021).

Figure 4: Tumor Infiltrating Lymphocyte Immunotherapy(Maqsood et al., 2023).
As an alternate treatment, monoclonal antibodies can be administered to cancer patients whose regular chemotherapy has failed or
progressed(Bayer, 2019). B-lymphocytes become active as a result of a foreign substance entering the body, and antibodies are produced in response to this foreign substance (antigen). Antibodies recognize the antigen's epitope regions. Monoclonal antibodies are antibodies that are generated against a single epitope rather than a complete epitope (mAb). The efficacy of mAbs in cancer immunotherapy is dependent on three basic mechanisms:
1-Antibody binding inhibits the factors and receptors that activate the signal pathways employed by cancer cells in division and angiogenesis, which is one of these processes.
2- Antibody-dependent cellular cytotoxicity (ADCC), which is made up of target monoclonal antibodies made up of chimeric or fully human antibody components that bind to specific antigens found in tumors.
3- Complement-dependent cytotoxicity (CDC) is a type of cytotoxicity caused by the activation of the complement system (Kimiz-Gebologlu, Gulce-Iz and Biray-Avci, 2018).

Figure 5: Monoclonal antibody immunotherapy in cancer(Xu, 2021).
Oncolytic viruses, like other immunotherapies, operate by a multimodal mechanism that imparts direct and indirect toxicity to tumor cells. These effects include autolysis, immune cell honing, vascular supply disruption, and enhancement of other complementary anti-cancer treatments(Raja et al., 2018).At the outset, oncolytic viruses may be administered intratumorally, subcutaneously, intraperitoneally, or intraarterially, among others. The preferred entry of oncolytic viruses into tumor cells is facilitated by natural tropism and genetic targeting. Following this, oncolytic viruses begin to identify abnormal cells via substances expressed in the tumor environment and can connect with and infect the host cell via various receptors. At this juncture, the virus initiates its utilization of the cellular apparatus to facilitate its replication process. This results in the production of viral proteins, impairment of cellular functionality, induction of oxidative stress states, and activation of certain pathways associated with autophagic processes. Simultaneously, certain viral organisms are encapsulated within the antigen-presenting cells, which initiates the formation of an endosomal vesicle that subsequently fuses with a lysosomal vesicle, resulting in the virus being digested and reduced to smaller particles that can be processed within the cell. Subsequently, the viral proteins and major histocompatibility complex class 2 are expressed on the cell surface, fostering an environment conducive to antigenic presentation and subsequent activation and stimulation of CD4+ and CD8+ T cells. The latter are involved in the direct destruction of the pathogen and the former in the synthesis of cytokines that aid in the maturation and migration of inflammatory cells. Ultimately, the eradication of tumor cells is facilitated by both the viral action and the immune response, which release viral progeny into the host organism. This allows the virus to infect additional aberrant cells and recommence its fight against the tumor. In addition, cell death facilitates the release of tumor antigens that can be recognized by the immune system, thereby promoting the development of novel inflammatory responses that can operate not only within the tumor microenvironment but also at metastatic sites (Apolonio et al., 2021).
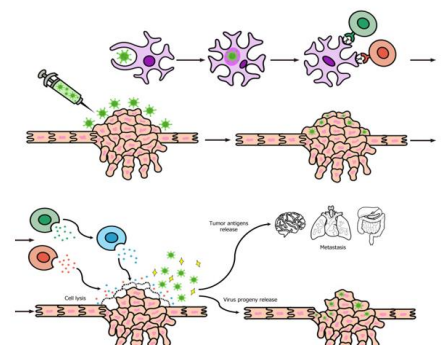
Figure 6: Oncolytic Virus therapy(Apolonio et al., 2021).
5.Immunomodulators
Small molecule immunomodulators targeting the adaptive immune system. Programmed cell death protein 1 (PD-1), also known as CD279, is a surface protein that can regulate the immune system by inhibiting T-cell activity. PD-1 is an important immunosuppressive molecule that plays a key role in the inhibition of antigen-specific T-cell response in diseases such as cancer. PD-1 is constitutively expressed in various immune cells like T lymphocytes, natural killer T cells, activated monocytes, and B lymphocytes. Nevertheless, PD-1 is only expressed on the cell surface of activated T lymphocytes rather than resting T cells. Thus, PD-1 can function as an intrinsic negative feedback loop for preventing T cell activation, thus reducing autoimmunity and promoting self-tolerance. PD-1 can be activated by two ligands including PD-L1 and PD-L2, which are also type I transmembrane proteins belonging to the B7/CD28 family. PD-L1 is widely expressed in lymphoid as well as tumor cells. Unlike PD-L1, the expression of PD-L2 is more restricted and barely found in tumor tissues. the infiltrated T cells overexpress PD-1, while tumor cells overexpress PD-L1 and PD-L2, which are induced by the tumor microenvironment (TME) in the body. The binding between PD-1 and PD-L1 causes a down-regulation of T cell effector functions in cancer patients, thereby promoting immune escape and leading to the survival of tumor cells. Inhibitors that inhibit the interaction between PD-1/PD-L1 reinstate the functionality of T cells, thereby restoring their immune function in the fight against cancer. Inhibitors of PD-1/PD-L1, also referred to as ICIs (immune checkpoint inhibitors), have exhibited remarkable effectiveness against a wide range of tumor types. As of now, the FDA has approved a multitude of ICIs, all of which are monoclonal antibodies (mAbs). Notable examples include Pembrolizumab (BMS), which is anti-PD-1; Avelumab, which is anti-PD-L1; Ipilimumab (BMS), which is anti-CTLA-4; Duvalumab, which is anti-PD-L1; Nivolumab, which is anti-PD-1; atezolizumab (Roche, anti-PD-L1). Despite the promising anti-tumor activities demonstrated by these mAbs in patients with specific tumor types, the clinical implementation of these antibody-based ICIs was impeded by obstacles including oral bioavailability and immune-related adverse effects. Consequently, there has been a heightened focus on the advancement of small molecule-based ICIs due to their potential to surmount the aforementioned constraints associated with therapeutic antibodies (Wu et al., 2022).

Figure 7: (A) PD-1/PD-L1 interaction between T cell and tumor cells. (B) Pharmacophore model of PD-1/PD-L1 immunomodulators (Wu et al., 2022).
In the past decade, therapeutic vaccinations against cancer have witnessed a revival. Advancements in understanding the magnitude of tumor-associated antigens, the mechanisms behind the host immune response, and the development of novel antigen delivery methods have collectively facilitated the enhancement of vaccine design(Song, Zhang and Wu, 2018). Therapeutic cancer vaccines can be incorporated into the treatment regimen for a wide array of cancer subtypes and stages(Schlom et al., 2014). Analyses of many tumor antigens have uncovered target characteristics that result in a high degree of selectivity towards tumor cells as opposed to normal cells and sufficient immunogenicity to impact therapeutic effectiveness. A limited number of tumor-associated antigens (TAIs), which are host proteins that are normally expressed but abnormally expressed in cancer cells, have exhibited promise as immunotherapeutic targets(Hollingsworth and Jansen, 2019). Therapeutic cancer vaccines aim to achieve the following objectives: promote tumor regression, eliminate minimal residual disease, establish durable antitumor memory, and prevent non-specific or adverse reactions. However, monoresistance and tumor-induced immunosuppression present formidable obstacles to achieving this objective. Vaccines against cancer commonly comprise exogenous delivery of specific tumor antigens in conjunction with adjuvants that stimulate dendritic cells (DCs), or DCs themselves. Boosting the patient's adaptive immune system against particular tumor antigens is the objective of therapeutic cancer vaccines to restore tumor growth control, induce regression of established tumors, and eliminate minimal residual disease. Successful therapeutic vaccination against tumors requires the following fundamentals: delivery of large quantities of a high-quality antigen to dendritic cells (DCs), optimal activation of DCs, induction of robust and sustained CD4+ T helper cell and cytotoxic T lymphocyte (CTL) responses, infiltration of the tumor microenvironment (TME), and maintenance and durability of the immune response. There are multiple approaches to achieve this goal, including the use of immune checkpoint inhibitors to reverse the immune exhaustion induced by the tumor, the administration of adjuvants containing tumor-associated antigens to stimulate DCs and effector T cells, or vaccination with autologous DCs loaded with specific tumor antigens. Conversely, the local immune environment of the tumor can be extensively stimulated to promote apoptosis of tumor cells. Furthermore, the availability of tumor antigens can be enhanced through the application of in situ vaccines (ISVs). In contrast to conventional vaccine methods, which involve the meticulous selection, purification, or preparation of antigens before injection into patients, the in-situ approach produces the vaccine within the tumor microenvironment (TME) through the utilization of antigens derived from deceased or dying tumor cells (Saxena et al., 2021).

Figure 8: Mechanism of Cancer Vaccine (Apostolopoulos, 2019).
Side Effects of Cancer Immunotherapy
Immunotherapies cause adverse effects through immune-mediated tissue damage to healthy tissues as shown in the(table1) below. This is because these therapies operate by modulating the interactions that occur between cancer cells and the immune system. Skin and mucosal surfaces, the luminal gastrointestinal tract, the liver, and the endocrine system are the most frequently affected organs. Mucositis may manifest as a dry mouth, whereas erythematous, reticular, or maculopapular skin rashes are typically the initial adverse effects. A prevalent adverse effect of anti-CTLA-4 antibodies is diarrhea. Similar characteristics to graft-versus-host disease are observed in luminal gastrointestinal tract biopsies, including villous blunting (small intestine), increased crypt epithelial cell apoptosis, lymphoplasmacytic lamina propria expansion, neutrophilic infiltration of epithelium, cryptitis, and crypt abscess formation. Although elevated levels of lymphocytes within the epithelial lining are uncommon, ipilimumab treatment may be linked to symptoms in the duodenal mucosa that resemble coeliac disease. It is noteworthy that immunotherapy-associated colitis may exhibit a favorable response to antitumor necrosis factor-α therapy, such as in the case of infliximab. Histolytic symptoms typically manifest as increased levels of transaminase in the bloodstream, although elevated bilirubin levels may also be detected. Lobular inflammation accompanied by perivenular accentuation or inflammation of the portal tract encompassing the bile ducts may be observed in liver biopsies. Involvement of the endocrine system generally leads to generalized symptoms including fatigue, nausea, and headache. (Bateman, 2019).
| Sites of potential side effects for immune checkpoint inhibitor therapies | |
| Sites | Examples |
| Kidney | Granulomatous interstitial nephritis. Membranous glomerulopathy |
| Pancreas | Acute pancreatitis |
| Neurological system | Encephalitis. Aseptic meningitis. Enteric neuropathy. Transverse myelitis. |
| Hematological system | Red cell aplasia. Neutropenia. Thrombocytopenia. |
| Lungs | Sarcoidosis. Organizing pneumonia. Pneumonitis. |
| Endocrine system | Hypophysitis Hypothyroidism. Adrenal crisis. |
| Liver | Hepatitis |
| Luminal gastrointestinal tract | Gastritis. Enteritis. Colitis. |
| Skin and mucosae | Rash. Oral mucositis. |
Table 1: Sites of potential side effects for immune checkpoint inhibitor therapies (Bateman, 2019).
The mechanism of drug resistance in immunotherapy
Immunity against cancer comprises immune surveillance, equilibrium, and evasion. By recruiting immune regulatory cells, downregulating tumor antigen expression, releasing immune inhibitory factors, and employing other immune evasion mechanisms within the host, tumor cells can elude immune system recognition and attack. This enables the cells to progress to metastasize and ultimately develop into visible tumor lesions. Additionally, it is possible to induce tumor proliferation through the targeted amplification of proteins that evade immune detection, such as PD-L1, arachidonic acid lipoxygenase, and IDO1/IDO-2. Mechanisms underlying resistance(Tan, Li and Zhu, 2020).

Figure 9: The mechanism by which immunotherapy induces drug resistance (Tan, Li and Zhu, 2020).
The pros and cos of Cancer Immunotherapy
Anti-tumor immunotherapy is presently assuming a role of growing significance within the domain of tumor therapy. Positive outcomes have been observed in treatment trials about a range of malignant tumors. By identifying novel targets and approaches, including combination therapy, the effectiveness of immunotherapy is enhanced, and adverse reactions are diminished. However, immunotherapy remains a subject of controversy due to several factors, including empirical and practical limitations, treatments that result in blindness, individual cases of severe and potentially fatal adverse reactions, the unpredictable nature of the therapeutic effect, and the exorbitant cost of treatment. Below the benefits and drawbacks of immunotherapy are detailed. Recognizing that tumor
development is a dynamic and intricate process, it would be possible to conduct targeted immunotherapy under the immune status of patients and the characteristics of the tumor to achieve the most effective therapeutic effect and restore the health of patients afflicted with tumors (Tan, Li and Zhu, 2020).
The Advantages of Cancer Immunotherapy
The disadvantages of cancer immunotherapy
Cancer immunotherapy, a therapeutic approach that harnesses the patient's immune system to combat the disease, is currently experiencing a surge in popularity. Vaccines, CAR-T cell therapy, and immune checkpoint therapy have collectively transformed the landscape of cancer treatment. Using CRISPR/Cas9 technology, specific genes or receptors can be silenced in allogenic T cells, potentially stimulating an immune response against these genetically modified cells when introduced intravenously into a patient. Furthermore, inaccessible to a surgeon, the activated and tumor-specific T cells are capable of efficiently penetrating those regions. The genetically modified tumor-specific T cells can therefore target even the most minute components of the disease. As opposed to alternative anti-cancer therapies, cancer immunotherapy does not induce significant cellular damage in healthy cells that are near the cancerous cells. In contrast to alternative treatments, it elicits prolonged clinical benefits and induces fewer adverse effects. Despite being regarded as a safer alternative to chemotherapy, immunotherapy is not without its limitations and adverse effects. Generally, dramatic and diverse treatments are administered, depending on the type, location, and patient of the cancer. As a result of the progress made in the field of cancer immunotherapy, the current emphasis is on treating the biological characteristics of tumors. In particular, for cancer immunotherapy to be effective, methods must be developed to regulate acquired resistance and ensure that tumors exhibit almost no resistant response. Therefore, the immunotherapy patient must be treated with caution and under appropriate monitoring.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
