
Review Article | DOI: https://doi.org/10.31579/2768-2757/155
1Medical microbiology department /College of Health Sciences/ Hawler Medical University/ Kurdistan region /Erbil/Iraq.
2Midwifery department, Erbil technical medical institute, Erbil polytechnic university, Kurdistan region/Erbil/ Iraq.
*Corresponding Author: Fattma A. Ali., Medical microbiology department /College of Health Sciences/ Hawler Medical University/ Kurdistan region /Erbil/Iraq.
Citation: Fattma A. Ali., Aki A, Khudhair Al-Daoody., Muna M Najeeb., Media A. Othman, (2024), Impact the Connection Between Adaptive Immunity and Systemic Lupus Erythematous, Journal of Clinical Surgery and Research, 6(1); DOI:10.31579/2768-2757/155
Copyright: © 2024, Fattma A. Ali. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 11 November 2024 | Accepted: 10 December 2024 | Published: 01 January 2025
Keywords: adaptive immunity; systemic lupus erythematous; t cells;b cells; il-6; il-10
Background: Systemic lupus erythematosus (SLE) is a systemic autoimmune disorder of unknown etiology that mostly impact females. SLE illness is defined by the emergence of auto antibodies and the accumulation of immune complexes, leading to inflammation and tissue damage in multiple organs. Patients suffering from this condition may display pathological harm to several organs such as the kidneys, skin, joints, blood, or neurological system.
Objectives: Our study aimed to carry out the role of the adaptive immunity including the main cells of adaptive immunity T cells, B cells, IL-6, IL-10 in the systemic lupus erythematous autoimmune disease.
Main body: T lymphocytes immune tolerance. The breakdown is a crucial factor in the development of SLE and T lymphocytes perform a significant role in this pathway. It may result in triggering and stimulation of B lymphocytes and dendritic cells at sites of inflammation, as well as abnormal release of cytokines and cellular signaling. B lymphocytes in patients with SLE suffer from impaired regional and peripheral tolerance. Lupus arises from an abundance of self-reactive B lymphocytes that produce a variety of auto antibodies. Interactions between T cells and B cells are widely recognized. IL-6, a type of inflammatory cytokine, has been linked to the development of SLE in both mice and humans based on scientific research. IL-10 has been observed to have two distinct functions in SLE patients. It is a cytokine that reduces inflammation by preventing the production of other cytokines that promote inflammation, such as IFN-c. In addition, IL-10 plays a role in the B cell function, resulting in the growth and specialization of B cells, the switching of antibody classes, and the reduction of B cell mortality in germinal centers, so facilitating the creation of autoantibodies.
Conclusion: The underlying mechanisms of SLE are not yet understood completely. Multiple predisposing factors are likely involved in the development of SLE and play a crucial role in triggering and sustaining aberrant immunological reactions. Nevertheless, the precise mechanism by which the disease develops is still not fully understood.
Systemic lupus erythematosus (SLE) is a systemic autoimmune disorder of unknown etiology that mostly impact females [1]. SLE illness is defined by the emergence of autoantibodies and the accumulation of immune complexes, leading to inflammation and tissue damage in multiple organs [2]. Typically, the body's immune system specifically evolves for response with external compounds, and cells from the immune system that try to fight against cells in the body are eliminated during development. In lupus and other autoimmune illnesses, however, the immune system learns to recognize and attack the "self." In other words, immune system cells begin to harm the body's own tissues. This incident is analogous to "friendly fire" aS it might result in permanent damage impairing the functioning of various body organs and systems. [3]. Individuals with this illness may exhibit clinical damage to the kidneys, skin, joints, blood, or neurological system, among other organs A number of predisposition variables are likely involved in the development of SLE an play a crucial role in triggering and sustaining aberrant immunological reactions. However, the exact nature of the pathogenesis remains unclear [4]. Approximately 8% of people worldwide suffer with autoimmunity. However, a variety of variables, such as increased awareness and better clinical diagnosis, are contributing to the incidence's rise [5] . Furthermore, there is proof that autoimmune illnesses rank among the USA's top causes of death for young women[6]. With a 9:1 gender skew, SLE mostly affects women. It has been partially linked to oestrogen receptor-1 and unidentified immunomodulatory genes on the X chromosome [7]. Immunosuppressive medication is the cornerstone of treatment; there is neither a cure nor a preventative. Gender is a factor in the etiology of disease, which also includes genetic predisposition and environmental influences [8]. The stages of SLE can be diverse, and not everyone will advance in the same way. It's worth noting that the concept of separate stages in SLE is not universally accepted, as the disease manifests differently in different people. Some general patterns and categories, however, are recognized, including: Early Stage/Incident Phase: Individuals may have nonspecific symptoms such as weariness, joint pain, and skin rashes during this phase[9] .Acute/Active Phase: Distinguished by the emergence of particular clinical and laboratory characteristics such as joint inflammation, skin lesions, kidney involvement, and hematologic abnormalities[10]. Remission: Some people may experience periods of remission in which their symptoms are less severe or nonexistent. A fundamental goal of treatment is to achieve and maintain remission[11] .Chronic/End-Stage :Chronic organ damage may occur in some situations, leading to long-term consequences. This can result in irreparable kidney, heart, and other organ damage [12] . The onset or severity of human disease has been linked to more than 60 genetic areas These genetic associations have directed research towards multiple pathways involved in innate and adaptive immunity ( involved T and B cells) [13 ].
Dysregulation of adaptive immunity
2.1.T lymphocytes
T lymphocytes immune tolerance. The breakdown is a crucial factor in the development of SLE and T lymphocytes perform a significant role in this pathway.It may result in triggering and stimulation of B lymphocytes and dendritic cells at sites of inflammation, as well as abnormal release of cytokines and cellular signaling. [14]. CD3 is a surface marker produced on mature T cells that establishes a non-covalent connection with T cell receptor and Takes part in the body's defense to antigen activation. The T cell receptor-CD3 comprises immune receptor tyrosine-based activation motif area , CD3 serves as the primary signaling molecule. After T cell receptor identification along with interaction of the major histocompatibility cell - antigen convoluted, Lck The Src kinase lymphocyte- specific protein tyrosine kinase phosphorylates the immune receptor tyrosine-based activation motifs of CD3. Phosphorylated CD3 ITAMs attract ZAP-70; Lck phosphorylates and stimulates ZAP-70, leading to the entry of calcium into T lymphocytes [15]. In Systemic lupus erythematosus , Expression of the CD3 chain was observed drastically reduced, resulting in T cell receptor complex recompilation The CD3 molecule was substituted with the analogous Fc receptor (FcR) [16]. The spleen tyrosine kinase is recruited by FcR, resulting in increased Calcium entry into T lymphocytes. Elevated calcium responses lead to raised calcineurin activity. Calcineurin dephosphorylates the inactive nuclear factor of activated T cells , which then translocates to the nucleus. As a result, the promoter of the CD40L gene and T cells are more easily activated. Calmodulin kinase IV activation, on the other hand, enhances The intranuclear expression of cyclic adenosine monophosphate sensitive component regulator inhibits the manufacture of IL-2. Lck is present in rafts of lipids, and previous studies have demonstrated that the creation of rafts made of lipids can exacerbate the state of lupus mice lymphocytes (T cells) obtained from individuals with SLE exhibited elevated levels of ganglioside M1 is
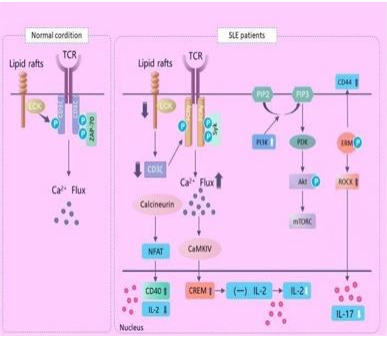
Figure 1: Action of the T lymphocyte in SLE.
Connected to and cholesterol, which are constituents of the lipid raft region. This finding provides confirmation that lipid rafts have a
significant impact on the underlying mechanisms of SLE (Figure 1) [17]. Alterations in lymphocyte activation in SLE. Lck is a protein tyrosine kinase that is exclusive to lymphocytes. TCR stands for T cell receptor. The proteins mentioned are: zeta-chain-associated protein kinase -70, Fc receptor common gamma subunit chain, spleen tyrosine kinase ,(NFAT) stand for nuclear factor of activated T lymphocytes , calmodulin kinase IV (CaMKIV) , cyclic AMP responsive element modulator , and interleukin . PIP2 , PIP3 , PIP4 , and PIP5 are abbreviations for phosphatidylinositol-4,5- bisphosphate, phosphatidylinositol-3,4,5-triphosphate, phosphatidylinositol-4,5-triphosphateand phosphatid PI3K, respectively. PI3K is an acronym for phosphoinositide-3 kinase .Protein kinase B (Akt), ROCK Rho-associated protein kinase, mTORC mammalian target of rapamycin complex, ERM ezrin- radixin-moesin. The pathway of cellular communication CD44 is a kind of protein that is associated with the rock and ERM signaling pathways. CD44 is a molecule that found on the surface of the cell in which plays a role in both T lymphocyte activation and adhesion. Previous studies have indicated that the levels of CD44 expression are elevated in patients with SLE. Additionally, specific splicing variants of CD44, namely CD44V3 and CD44V6 , have been found to be linked to disease activity in those with SLE [18-20]. The adhesion and migratory functions of CD44 necessitate its interaction with the (ERM) proteins. Rho-associated protein kinase (ROCK), a serine threonine kinase, phosphorylates the ERM protein. In patients with SLE, there was an elevation in the phosphorylation level of ERM protein, leading to an enhancement in lymphocyte adherence and movement. In addition, ROCK has the ability to initiate the activation of Interferon regulatory factor 4, impact the process of T helper 17 differentiation, and control the synthesis of the interleukin-17 and Interleukin- 21 [21]. The signaling pathway known as the PI3K- Akt-mTOR cascade The lipid downstream kinase family encompasses phosphoinositide-3 kinase . At present, class I PI3K is the main researched. G protein coupled receptors and receptor tyrosine kinase can both activate it. Akt is an essential downstream target kinase of PI3K. The mammalian target of rapamycin signaling pathway is a crucial controller that combines nutritional data and mammalian target of rapamycin signaling stimulates protein production. PI3K activity is increased in SLE, according to studies in humans and animals, PI3K suppressor have the ability to decrease inflammation in tissues and enhance clinical manifestations. [22, 23]. Following TCR activation, PI3Ks are recruited to the TCR complex and produce phosphatidylinositol-3,4,5- triphosphate (PIP3) from membrane phospholipids. PIP3 then phosphorylates and activates Akt via phosphoinositide-dependent protein kinase 1. Phosphorylated Akt stimulates mTOR and increases protein synthesis, which aids in lymphocyte splitting, growth, and surviving (Figure 1). Prior studies have demonstrated that there is an increase in Akt expression in both T and B lymphocytes in the peripheral blood vessels of individuals with SLE. Additionally, it has been found that the level of Akt mTOR activation in B lymphocytes is positively correlated with the severity of the illness [24, 25]. Th1 Th2 cell imbalance Th cells are a kind of CD4+ T cell. Th cell dysfunction is linked to the onset and progression of SLE. And an imbalance of Th1 Th2 cells is thought to play a role in the development of SLE. Th cells are classified as Th1 or Th2 based on the release of different cytokines and the adjustment process is dynamic. TNF-, IL-2, and IFN- are secreted by Th1 cells and are involved in the activation of macrophages and CD8+ T cells, which is associated with organ-specific autoimmune disorders. T helper 2 lymphocytes release Interleukin-4, Interleukin-6, and Interleukin-10, that have ability to activate B lymphocytes and cause Immunoglobulin G1 production. In order to preserve the equilibrium of the immune system, the two distinct cell types often regulate and suppress each other through the use of cytokines. The equilibrium mentioned above is disrupted in SLE, however the inclination of balance remains a subject of ongoing debate. The prevailing consensus among researchers is that active SLE is marked by reduced T helper1 activity and excessive T helper2 activity, resulting in heightened activation of B lymphocytes, generation of autoantibodies, and tissue damage [26, 27]. Although , Dolff et al. [28] discovered that T helper1 take the place of the Th1/Th2 balance in the long duration of sequences of SLE, particularly those individuals with lupus nephritis IV. More research is required. Th17 Treg cell imbalance T helper17 lymphocytes , a kind of effector T helper cell, that distinguished by their capacity for synthesis Interleukin- 17A, Interleukin-17F, and Interleukin-22, that facilitate inflammatory reactions and contribute to the progression of autoimmune diseases. Interleukin-17 is the primary cytokine that promotes the involvement of T helper17 lymphocytes in SLE. Elevated levels of Interleukin-17 have been observed in the kidneys of patients with lupus nephritis, as well as a higher expression genes of Interleukin- 17 in urine sediment [29, 30]. Th17 expression was also detected in the skin, lung, and renal tissues of patients with SLE. Disease activity in Systemic Lupus Erythematosus was found to be associated with increased levels of T helper 17. The collaboration between Interleukin-17 and B-lymphocytesstimulating factor enhances the growth of B cells and surviving, hence promoting humoral defence and the formation of autoantibodies. Regulatory T cells are involved in maintaining self-tolerance and their impaired function is associated with the onset of autoimmunity. Regulatory T cells have the ability to impact the activity of effector T lymphocytes, uphold immunological balance, and prevent the occurrence of autoimmunity. Multiple studies have revealed a decrease in the quantity of Regulatory T cells in individuals with systemic lupus erythematosus accompanied by impaired functionality [31, 32]. The presence of Thelper17 and regulatory T cells is typically maintained in a state of equilibrium, but this balance is disrupted in the context of SLE [33]. Current understanding suggests that an elevation in T helper 17 cells is associated with a reduction in Regulatory T cells, and that the dynamic changes in both cell types play a role in the immune system's defense mechanism. T follicular Helper lymphocytes a subset of T helper cells, have a crucial function in the establishment of germinal centers and the selection of Blymphocytes with high affinity. Multiple investigations have established aconnection between T follicular Helper and germinal centers responses with the occurrence of SLE. The circulating T follicular Helper phenotype in patients with SLE is described as follows: The chemokine receptors CXCR3 and CCR6, the inducible co-stimulator and the programmed death molecule-1 . When T helper cells come into touch with antigen-presenting cells , the inducible T-cell co-stimulator transmits activation signals, while programmed cell death protein 1 transmits inhibitory signals. Inhibiting the ligand in NZB NZW mice can restrict T follicular Helpercells activityand germinal centers synthesis, while also reducing the levels of anti-dsDNA antibodies [34]. Following in vitro co-culture with naive B lymphocytes circulating T follicular Helper cells had the ability to generate Interleukin-21, enhance B-cell growth and distinction and secrete Immunoglobulin G and Immunoglobulin A. Elevated levels of circulating T follicular Helper cells were observed to be positively associated with disease activity and serum autoantibody concentrations in living organisms [35]. A recent study has demonstrated that immunological complexes containing DNA contribute to the development of autoantibodies in SLE by stimulating -cell responses . This finding provides evidence of the involvement of T follicular Helper cells response in pathogenesis of SLE [36].
2.2.B lymphocytes
B lymphocytes / SLE patients exhibit compromised immune tolerance of lymphocytes, both in the regional and peripheral systems. Lupus arises from an abundance of self-reactive B lymphocytes that produce a variety of autoantibodies. The connections between B and T lymphocytes are widely recognized. Immature B lymphocytes demonstrate a discernible inclination towards activation by integrating signals that originate from B-cell receptors and Toll-like receptors. Following Toll-like receptors management, B cell receptor recognizes certain antigens that contain RNA and or DNA and generates protein polypeptides, hence stimulating B lymphocytes. B cells that have been activated go towards the outer edge of the follicle and interact with T helper cells through the T cell receptor and co-stimulatory molecules. On the contrary, activated B lymphocytes secrete cytokines such as Interleukin-6, tumor necrosis factor interferon necrosis and Interleukin-10 [37]. T follicle helper cells, however, are T helper cells that become active and migrate to B-cell follicles in order to secrete Interleukin-21 and Interferon necrosis-. T follicular helper cells augment germinal centers formation by secreting Interleukin-21, which sustains the expression of B-cell lymphoma 6 and stimulates B-lymphocyte activation, class-switch recombination, and the differentiation of plasma cells. Plasma cells with an extended lifespan are ultimately produced (Figure 2). The connections between T and B lymphocytes are also affected by B lymphocytes activating factor . B lymphocytes activating factor is upregulated, stimulating B cell proliferation and prolonging the lifespan of self-reactive B cells. B lymphocytes activating factor transgenic mice exhibited notable B-lymphocytes proliferation, generation of anti-ds DNA antibodies , increased levels of serum Immunoglobulin M, A, E and G and lupus-like changes in renal tissue, including the deposition of complex immune responses moreover, studies conducted on NZB/NZW lupus mice have shown that there is an elevation in B lymphocytes activating factor levels during the initial phases of SLE and the concentration of B lymphocytes activating factor in the blood is directly associated with the severity of kidney damage-cell subsets Regulatory B cells, also known as Bregs, are a specific type of cell that regulates the immune system [38].

Figure 2: Action of the B lymphocyte in SLE.
Interactions between T and B lymphocytes are frequently observed in SLE. TLR stands for Toll-like receptor, MHC-II refers to major histocompatibility complex-II, and BCR stands for B-cell receptor. BCL is a shortened form of B-cell lymphoma. TCR stands for T cell receptor, IL stands for interleukin, IgM stands for immunoglobulin M, IgG stands for immunoglobulin G, ICOS stands for inducible co-stimulator, and ICOSL stands for inducible co-stimulator ligand. BAFF is a substance that activates B-cells, BAFFR is a receptor that responds to BAFF, IFN is a type of protein that interferes with viral infections, IFNR is a receptor that responds to IFN, and GC is a specialized area where B-cells develop. contribute to autoimmune regulation and inflammation. Bregs were found to generate Interleukin-10 that modulates the T-cell-dependent immunological response in mice [39]. Regulatory B lymphocytes were shown to be lower in individual those with lupus than in normally individuals , particularly in those with lupus nephritis, and the list of these lymphocytes increased after immunosuppressive treatment [40]. Furthermore, the sensitivity of Regulatory B lymphocytes to Cluster of differentiation40 activation and Interleukin-10 secretion. that decrease in SLE patients' peripheral blood vessels , indicating that of Regulatory B lymphocytes were dysfunctional [41].
2.3. Interleukin-6
Interleukin-6 / is an inflammatory cytokine that has been linked to the development of SLE in both animal and human research. The presence of Interleukin-6 in MRL/lpr mice leads to a reduction in renal function. This observation is supported by results from tests in which mice were administered synthesized Interleukin-6 or inhibitory IL-6 Ab, leading to an increase or decrease in lupus nephritis, correspondingly. IL-6 is crucial in the process of B cell maturation into plasma cells, and research has shown that inhibiting this cytokine reduces the production of autoantibodies. In addition, research has shown that SLE patients have higher amounts of IL-6 in their blood serum compared to healthy individuals [42]. The potential therapeutic use of Tocilizumab, an IL-6 receptor blocker, is currently being investigated for the treatment of SLE. Tocilizumab exhibits good tolerability and reinstates the equilibrium of B- and T-lymphocytes [43].
2.4. Interleukin-10
Interleukin-10 has been observed to have two functions in systemic SLE. This is a cytokine that reduces inflammation by preventing the production of proinflammatory cytokines like Interferon necrosis-c. In addition, IL-10 plays a role in B lymphocytes function, resulting in the growth and specialization of B lymphocytes, the switching of Ab types, and the reduction of lymphocyte mortality in germinal centers. This ultimately encourages the creation of autoantibodies [44].
2.5. Potential therapeutic targets in SLE
Between 1999 and 2008, no additional drugs were included in the treatment guidelines for SLE as recommended by the American Academy of Rheumatism and the European League For Rheumatism. Nonsteroidal anti-inflammatory medications, glucocorticoids, hydroxychloroquine, and immunosuppressive medicines are now the mainstays of SLE therapy. However, all of these treatments try to control the symptoms of the disease rather than the root cause; they exhibit a broad spectrum of non-specific impacts and are associated with substantial toxicity. Advancements in comprehending the causes of SLE have led to the exploration of medications that target putative illness links, offering a novel approach to treating SLE [45]. T-cell immune therapy T lymphocytes support lymphocytes in generating autoantibodies with a strong binding affinity for Immunoglobulin G. T lymphocyte activation requires distinct signals. The second signal can be activated by co-stimulatory signals such as CD40/40L, CD28, cytotoxic T-lymphocyte antigen 4 , CD80/CD86 and ICOSL/ICOS. Abatacept is a recombinant protein that combines the Fc region of immunoglobulin IgG1 with the extracellular domain of cytotoxic T-lymphocyte antigen 4 , . It has a higher affinity for binding to CD80/CD86.compared.to.CD28. It restricts the activation of T lymphocytes by reducing the co- stimulation of T and B lymphocytes, hence preventing the response of B lymphocytes [46]. The effectiveness of this medication in treating arthritis is widely recognized, while its impact on SLE remains uncertain. In a phase II/III research study, abatacept proved effective in increasing levels of C3 and C4, while also reducing levels.of.ds-DNA [47]. However, the primary objectives were not achieved in a subsequent randomized controlled trial that specifically targeted LN, which is another crucial receptor/ligand pair necessary for the formation of T follicular helper cells, known.as.CD40-CD40L. BG9588 is a monoclonal Ab that specifically targets.CD40L [48]. B lymphocytes targeted therapies The disruption of B lymphocytes tolerance, leading to an enhanced production of various The presence of autoantibodies targeting nuclear Ag is a characteristic feature of immunological dysfunction in SLE. Consequently, there is a development of new therapeutic medications that specifically aim at inhibiting the growth and maintenance factors, surface compounds, and receptors of B lymphocytes, leading to their demise, reduction, or functional inactivation. Belimumab is a monoclonal Ab of the human Immunoglobulin G1λ type that hinders the surviving and development of B lymphocytes by obstructing the soluble B cell activating factor. In 2011, it received approval in both the USA and Europe for treating people who have active autoantibody-positive SLE and are already undergoing conventional therapy. Based on the phase III randomized controlled trials , the medicine showed a more significant therapeutic response in a specific group of patients who had higher disease activity at the beginning, as indicated by anti-dsDNA positive, hypocomplementemia (C3 or C4), or the need for corticosteroid treatment [49]. APRIL functions in a manner similar to soluble B cell activating factor and is also essential for the survival and activation of B lymphocytes [50]. APRIL exhibits higher affinity than soluble B cell activating factor for binding to transmembrane activator-1, calcium modulator ligand interactor (TACI), and B-cell maturation antigen receptors. In vivo studies have demonstrated that TACI-Ig, but not soluble B cell activating factor -R-Ig, effectively inhibits the production of Immunoglobulin M antibodies in the bloodstream, reduces the number of plasma cells in the spleen, and restricts the Immunoglobin M immune responses to an antigen that requires lymphocyte involvement [51]. Atacicept is the representative agent of TACI-Ig. Additional medications targeting B lymphocytes are now under investigation. Rituximab is a monoclonal Ab that is a combination of human and mouse components. It specifically targets CD20.receptors on B lymphocytes, leading to their death and reducing their growth. It is highly effective in eliminating abnormal B cell growth. Originally, the FDA promoted and authorized its use for treating B-cell lymphomas, and it demonstrated significant therapeutic benefits. Subsequent trials have demonstrated the efficacy of rituximab in treating refractory symptoms of SLE specifically nephritis and neuropsychiatric disease, in both adult and pediatric patients [52-55]. The primary adverse event is an allergic reaction due to the chimeric nature of the anti-CD20 Ab. Additional anti-CD20 Ab, such as the fully human monoclonal Ab (ofatumumab) and modified versions with enhanced antibody- dependent cellular cytotoxicity (obinutuzumab), are being studied in the pipeline for SLE [56].
SLE is a multifaceted, complicated autoimmune illness marked by aberrations at the cellular and molecular level. Pathophysiology of Systemic lupus erythematous is still not completely understood. Individuals with this illness may exhibit clinical damage to the kidneys, skin, joints, blood, or neurological system, among other organs. Several predisposing variables are likely involved in the development of systemic lupus erythematosus and are important in initiating and maintaining abnormal immune responses. However, the exact nature of the pathogenesis remains unclear. It’s mainly affect female more than male due to estrogen receptor-1. The SLE can be accord through different stages which differ from one individual to another the stages including of Early Stage/Incident Phase, Acute/Active Phase, Remission or Chronic/End-Stage. In SLE, the immune response has been widely investigated, including adaptive immunity. And our understanding of aberrations at the cellular and molecular level for the pathogenesis of Systemic lupus erythematous has grown dramatically. B lymphocytes are important in the adaptive immune response to SLE, as they are involved in the generation of autoantibodies, The display of self-antigens and the stimulation of self-reactive T lymphocytes. T lymphocytes also contribute through the co-stimulator-mediated signaling pathway and the release of cytokines by certain subsets of T cells. IL-6, an inflammatory cytokine, has been linked to the development of SLE in both mice and humans based on scientific research. Also two important interleukins are participate in the pathogenesis of SLE IL-6 can be produced by activated B cells when T cells loss tolerance and remains incompletely defined, Interleukin-6 plays a crucial role in sustaining the auto-inflammatory cycle in systemic lupus erythematosus. Elevated levels of Interleukin-6 have been observed in both human and murine lupus. In all investigated models of lupus, the positive effect of inhibiting Interleukin-6 or its receptor has been demonstrated. IL-10 was first thought to be a cytokine produced solely by CD4+ Th2 cells, but subsequent research revealed that it was secreted by both T helper1 and T helper2 cells. CD4+ Foxp3+ CD25+ "natural" regulatory T cells and Interleukin-10-induced CD4+ Regulatory cells (Tr1 cells) both produce Interleukin-10. IL-10 plays a dual role in immunological responses, inhibiting T cell activation while stimulating B cells. It is also generated by helper T cells and is thought to play a pathogenic role in SLE by stimulating autoreactive B cells. Understanding the immunological pathophysiology of SLE has resulted in the development of novel biologic drugs that attempt to specifically target aberrant immune processes, reducing the undesired side effects associated with traditional broad-spectrum immunosuppressive medications. Despite the fact that our understanding of SLE is still limited, and the majority of the innovative medications are still in clinical trials, these new biologic agents and small-molecule therapeutics may lead to the creation of safer and more effective therapies.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
