
Review | DOI: https://doi.org/10.31579/2640-1053/106
Retired in Hematology Department, Iran University of Medical Sciences, Tehran, Iran.
*Corresponding Author: Ahmad Reza Rahnemoon. Retired in Hematology Department, Iran University of Medical Sciences, Tehran, Iran.
Citation: Ahmad R Rahnemoon. (2022). Immunophenotyping Investigation in Acute and Chronic Leukemias as a Gold Standard Test. Cancer Research and Cellular Therapeutics. 6(1); Doi:10.31579/2640-1053/106
Copyright: © 2022 Ahmad Reza Rahnemoon, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 17 December 2021 | Accepted: 30 December 2021 | Published: 07 January 2022
Keywords: immunophenotyping; hematopoietic stem cell; progenitor cell; leukemia
Immunophenotyping of leukemias and other hematological neoplasms has become one of the most relevant clinical applications of flow cytometry which remains an indispensable tool for the diagnosis, classification, staging as well as hematologic malignancies monitoring. It can provide quantitative data on a number of cell parameters for a large number of cells in the region of cells thousands per second which making it a powerful diagnostic tool. If immunophenotyping is more sensitive significantly, specific and objective than morphological studying, the latter remains the gold standard criterion for creating and establishing the blast percentage in presentation and post treatment together. Moreover, it is important that interpreters of flow cytometric data have the phenotypes exact knowledge of diverse normal cell populations, which can be one of the best tool in recognize deviations from normal as well as are able to discuss the potential clinical significance and knowing look of the flow cytometric findings.
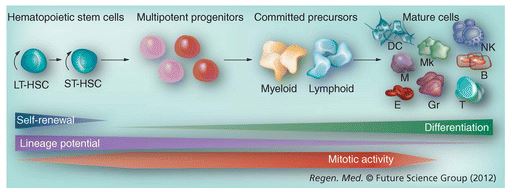
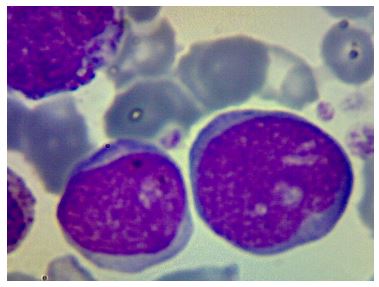
The multi-lineage process of hematopoiesis resulting in the peripheral blood mature cells appearance including erythrocytes, monocytes, granulocytes, lymphocytes and platelets which maintained by hematopoietic stem cells (HSCs). The differentiation of HSC give rise to multi-potent progenitors (MPPs) which limited in self-renewal ability but keep the potential for multi-lineage differentiation MPP can change to common myeloid progenitors (CMPs) and immature lymphoid progenitors population. On the other hand, the leukemic blasts clones of different origin and also maturation levels represent the leukemic stem cells(LSCs) progenitors sharing some common phenotypic features and functional properties with normal HSC (figure 1&2).

The diagnosis of acute leukemia relies on enumeration of the percentage of blasts in the peripheral blood or bone marrow; the current criterion in the world health organization (WHO) classification for the diagnosis of acute leukemia is greater than 20% blasts. In this regard, the vast majority acute lymphoid leukemia (ALL) cases are B lineage. In fact, due to the lack of conformity and the questionable significance of the further sub classification, the WHO classification classified ALL cases as precursors of B and T without additional categorization (figure 2) [7-10, 38-40].
The principle of flow cytometry is rather simple: to scan single cells flowing past an excitation source in a liquid medium and analyzed them according to their fluorescence. Regarding, in flow cytometry, identification of blasts relies on the demonstration of expression of immature antigens by a population having appropriate CD45 expression and light scatter characteristics. Although it is the overall immunophenotype that allows identification of blasts, antigens commonly used for blast identification include CD34, CD117, CD133, and terminal deoxynucleotidyl transferase (TdT). White blood cells express some levels of intensity characteristic of both lineages and stage of differentiation that when used in conjunction with orthogonal light scatter (side scatter) allow delineation of the basic white blood cell populations .This technique is particularly useful for the identification of blasts, given their expression of intermediate CD45 and low side scatter; CD45 versus side scatter analyses has become standard practice in the clinical laboratory for this purpose [1-4,8].
Although flow cytometry is excellent at identifying and enumerating blasts, two issues suggest caution in utilizing flow cytometric blast percentages for making an initial diagnosis of acute leukemia. First, the blast percentage obtained from bone marrow specimens is often inaccurate because of a combination of peripheral blood dilution (artificial decrease) and compromise of nucleated erythroid precursors during specimen processing using lysing reagents (artificial increase). Second, blasts identified by immune phenotyping do not always directly correspond to blasts identified by morphology. This is true because leukemic populations, similar to normal populations, consist of a maturational continuum and there is not perfect concordance between specific antigenic changes and the arbitrary morphologic changes that distinguish blasts from more differentiated cells. Moreover, in some types of leukemia, in early neutrophilic series and monocytic precursors are intentionally included in morphologic blast counts. Nevertheless, if one pays attention to these limitations, the diagnosis of acute leukemia can generally be correctly suggested. Co-expression of other non-lymphoid markers is common on the lymphoblast in both precursor-B and precursor-T ALL and does not necessarily indicate bi lineal potential. The myeloid markers, CD13 and CD33, are the most frequently expressed [1-3, 5-11].
In the past, these have erroneously been interpreted as indicating a bi phenotypic process and a worse prognosis, but more recently this has not been found [10]. Recently, more strict criteria with a uniform grading system have been instituted to help define the bi-phenotypic entity. Cytoplasmic expression of myeloperoxidase in ALL has also been reported by flow cytometric analysis. However, this does not correspond to the cytochemical detection of enzyme reactivity, and when identified with a polyclonal antibody it is of only questionable significance [11-15].
Differential diagnostic considerations
We have to be considered in immunophenotyping include hematogones, thymoma, bi- phenotypic leukemia, and chronic myeloid leukemia (CML) presenting in lymphoid blast phase. Hematogones have the same immunophenotype as common precursor B ALL cells, but the hematogones exhibit a spectrum of maturation with a continuum of cells from immature to mature showing loss of CD34, and gain of CD20 and slg [4-6].
Thymoma cells have the phenotype of common thymocytes, and cannot be distinguished from common To ALL/lymphoblastic lymphoma by immunophenotype alone. Correlation with clinical presentation and histology is important the correct interpretation. When CML presents in lymphoid blast crisis (figure 3), distinction from Philadelphia chromosome-positive (Ph+) ALL cannot be made on the basis of immunophenotype as the blasts are frequently precursor B lymphoblasts. In most cases the presence of a concurrent myeloid component to the leukemia will alert one to the correct diagnosis. If this were not present, lineage analysis showing the BCR/ABL fusion in myeloid as well as lymphoid cells has been suggested as a means of differentiating the stem cell process, CML, from the lymphoid-restricted process, ALL. In some cases, only the emergence of a myeloid component after treatment can indicate the correct diagnosis [16-20].
As it described, myeloid lineages classified according to their stage of maturation. For example, CD34+ and/or TdT+ neoplastic cells are classified as immature, while cells expressing sIg, sCD3/TCR in the absence of CD34, are more likely to be classified as mature. This information is of great help for the diagnostic classification of hematological malignancies and is accordance of previous reports about classification of ALL [16-17, 21].
The first classification categorized by morphology and cytochemistry supplemented by immunophenotyping, as proposed by FAB group; and after that world health organization (WHO) proposed a classification of acute leukemia, then the European group for the immunological classification of leukemias classified it by immunophenotyping alone, as proposed by some researchers [20-25].
Patients with AML show myeloid markers like MPO, CD13, and CD33, whereas patients with ALL show lymphoid markers. Confusion may arise when some patients with ALL express aberrant myeloid markers, such as CD13. If the cells are TdT positive, myeloperoxidase negative, CD33 negative and show lymphoid markers, the leukemia is considered ALL. In our study, eighty-nine percent of cases of ALL are derived from B-cells. The primary distinction was between (1) early (pro-B) ALL which is TdT positive, CD10 and surface immunoglobin G negative (2) precursor B ALL, which is TdT positive, CD10 positive, but surface immunoglobin G negative, and (3) mature B cell (Burkitt type) ALL, which is TdT negative, and surface immunoglobin G positive. Progressively some individual immunophenotypic markers were also associated with disease prognosis. Among others, CD38 and, more recently intracellular ZAP70 expression, were shown to be related to a worse clinical outcome in B-diagnosis. Hence immunophenotypic analysis is critical to confirm a morphological diagnosis of ALL, to resolve a difficult diagnosis and to further sub-classify cases into precursor-B and precursor-T lineage types. However, a specific immunophenotype identified at diagnosis might also be useful for evaluating residual disease by flow cytometry. According to immunophenotipic reports for ALL patients, more than 95% of cases of ALL are positive for TdT, but it is not specific for ALL. TdT is present in some subtypes of AML such as M0. Additionally, TdT is absent in cases of ALL-L3. TdT may also help to distinguish ALL from malignancies of more mature lymphocytes. Immunophenotyping shows TdT positive blasts that express CD la, CD2, CD3, CD4, CD5, CD7, and cyto CD3. Abnormal karyotype is seen in 50-70
Flow-cytometry is the excellent at identifying and enumerating blasts for making an initial diagnosis of acute leukemia, thereby I state some important points as follows; 1) blast cells identified by immunophenotyping do not always directly correspond to blasts as identified by morphology. 2) Flow-cytometry is extremely useful in excluding an acute leukemia diagnosis when the bone marrow is populated by cells that in mimicking to acute leukemia. However, in some cases like small cell carcinoma, the cells can resemble leukemic blasts on the smears, but in flow-cytometry, they can easily distinguish from leukemic blasts as well. 3) The determination of myeloid or lymphoid lineage is a major therapeutic importance decision which can be in the following of flow-cytometry major role in immunophenotyping category and acute leukemia classification too. 4) Residual disease monitoring in acute leukemia, can be very useful in identifying specific differences between background normal elements and the leukemic population at present, thereby, for detect small abnormal populations, we should increase the ability to use flow-cytometry.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
