
Research Article | DOI: https://doi.org/10.31579/2692-9392/170
Department of Medical Laboratory Science, College of Health and Medical Sciences, Afe Babalola University, Ado-Ekiti, Ekiti State, Nigeria.
*Corresponding Author: Omon A. Emmanuel, Department of Medical Laboratory Science, College of Health and Medical Sciences, Afe Babalola University, Ado-Ekiti, Ekiti State, Nigeria.
Citation: Ekundina V.O, Oladele A.A, Omon A Emmanuel, and Aliyu, A, (2023), Immunohistochemical Expression of MSH6 and MSH2 in Colorectal Cancer, Archives of Medical Case Reports and Case Study, 7(2); DOI:10.31579/2692-9392/170
Copyright: © 2023, Omon, A. Emmanuel. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 04 April 2023 | Accepted: 11 April 2023 | Published: 18 April 2023
Keywords: colorectal cancer; immunohistochemistry; expression; MSH2; MSH6
Colorectal cancer (CRC) is the cancer of the colon and rectum, which are situated, in the lower digestive tract. CRC is caused by mutations that target oncogenes, tumor suppressor genes and genes related to DNA repair mechanisms. The aim of this study was to observe and study the expression of MSH6 and MSH2 in colorectal cancer and to determine the expression of these markers in normal colorectal sample, colorectal intraepithelial neoplasia and colorectal cancer. A total of 65 formalin fixed paraffin embedded tissue blocks comprising 15 normal colorectal tissues, 25 colonic polyps tissues and 25 malignant invasive colorectal cancer were retrieved from the Pathological Archives. Immunohistochemical analysis was carried out on the samples. The immunohistochemical staining was evaluated and the results obtained were considered. Nuclear MSH2 staining was expressed; Normal cases showed a positivity rate of 46%, Colonic polyps’ cases showed a positivity rate of 56%, colorectal carcinoma cases had a positivity rate of 100% as all of the cells showed significant expression. Nuclear MSH6 was expressed; Normal cases showed a positivity rate of 40%, Colonic polyps’ cases showed a positivity rate of 60%, colorectal carcinoma cases had a positivity rate of 100% as all of the cells showed significant expression. There was a distinct upregulation of MSH2 and MSH6. The upregulated expression of MSH2 and MSH6 in normal colorectal tissues, neoplastic colonic polyps and colorectal cancer confirms the usefulness of tumor biomarkers and Immunohistochemistry in predicting progression of malignant lesions.
Cancer of the colon and rectum, which are located in the lower digestive tract, is referred to as colorectal cancer (CRC). Around a million people are affected by adenocarcinoma of the colon and rectum every year, and the 5-year mortality rate is close to 50% [1]. As the third most frequently diagnosed cancer and the fourth leading cause of cancer death globally, colorectal cancer poses a serious threat to public health [2]. Oncogenes, tumor suppressor genes, and genes involved in DNA repair pathways are the targets of mutations that lead to CRC. Colorectal cancers can be categorized as sporadic (70%), hereditary (5%) or familial (25%), depending on the source of the mutation. Chromosome instability, microsatellite instability (MSI), and the CpG island methylator phenotype are the pathogenic processes causing this condition [3].
DNA mismatch repair protein the MSH2 gene, which is found on chromosome 2, encodes the protein known as MSH2, often referred to as MutS homolog 2, or MSH2[4]. A DNA mismatch repair (MMR) protein, MSH2, is encoded for by the tumor suppressor gene MSH2. MSH2 forms a heterodimer with MSH6 to create the human MutS mismatch repair complex [5]. MSH2 participates in a variety of DNA repair processes, including base excision repair [6], homologous recombination [7], transcription-coupled repair and homologous recombination [8]. Microsatellite instability and various malignancies, including hereditary nonpolyposis colorectal cancer, are linked to mutations in the MSH2 gene (HNPCC). This gene has at least 114 known pathogenic mutations [9].
In the budding yeast Saccharomyces cerevisiae, the MSH6 gene, also known as mutS homolog 6, codes for the DNA mismatch repair protein MSH6. Whereas hMSH2 mutations strongly influence the phenotype of all mutators, hMSH6 mutations have a much more limited impact. At the gene level, it was discovered that the mutations mainly resulted in single-base substitution mutations, which implies that hMSH6 predominantly functions to repair single-base substitution mutations and, to a lesser extent, single base insertion/deletion mutations [10].
Immunohistochemical markers MSH6 and MSH2 have been demonstrated to be helpful in the diagnosis of colorectal lesions. In order to understand how MSH6 and MSH2 are expressed in colorectal cancer, this study will examine how these markers are expressed in normal colorectal tissue, colorectal intraepithelial neoplasia, and colorectal cancer. The study's results will help in observing the development of benign into malignant lesions of the colon through the process of immunoreactivity and figuring out whether these markers may be employed to express colorectal cancer for potential treatment choices.
One of the most prevalent tumors of the gastrointestinal tract is colorectal cancer (CRC). Almost 10% of all cancers diagnosed each year and cancer-related deaths globally are caused by colorectal cancer [5]. It is the second most frequent cancer among women and the third most frequent among men. Estimates of the heredity of colorectal cancer based on twin and family studies range from 12% to 35%. Immunohistochemical markers MSH6 and MSH2 have been demonstrated to be helpful in the diagnosis of colorectal lesions [9]. The aim of this study is to determine the expression of MSH6 and MSH2 in colorectal cancer.
Tissue Sample Selection
A total of 65 formalin fixed paraffin embedded tissue blocks comprising of 15 normal colorectal tissues, 25 colonic polyps tissues and 25 malignant invasive colorectal cancer were retrieved from the Pathological Archives of the Obafemi Awolowo University Teaching Hospital Complex Ile-Ife (OAUTHC).
Immunohistochemical Analysis
The expression of the biomarkers, MSH2 and MSH6, were demonstrated immunohistochemically using the Avidin-biotin immuno-peroxidase method. Sections on adhesive coated glass slides were deparaffinized in xylene and rehydrated using different gradients of ethanol. The sections were pretreated in a pressure cooker for antigen retrieval, using antigen retrieval buffer at 950C for 30 minutes, 900C for 10 seconds and 100C for 10 minutes. Endogenous peroxidase activity was blocked by immersion in 3% hydrogen peroxidase solution for 5 minutes. Non-specific binding was blocked with the use of blocking buffer (horse non-immune serum) for 15 minutes. 200μl of diluted primary antibody (BioGenex mouse monoclonal primary antibodies) for MSH2 and MSH6 sequentially was added to slides and incubated at room temperature for 80 minutes. The slides were incubated with biotinylated rabbit anti-mouse secondary immunoglobulins for 15 minutes at room temperature. They were subsequently incubated with avidin-biotin peroxidase complex. 3,3-diaminobenzidine was used as a chromogen. The sections were counter stained with hematoxylin.
Immuno-staining Assessment
Expression of MSH6 and MSH2 were determined through a semi-quantitative method. The immunoreactivity of these markers was determined by assessing the staining intensity and percentage of stained cells per field. The staining intensity was graded as mild, moderate and severe. The percentages of positive cells were graded as follows:
0.1%- 10% are stained = negative (-), grade 0.
10.1%- 39% are stained= positive (+), grade 1.
40. 0%-79% are stained= positive (++), grade 2.
80.0%-100% are stained = positive (+++), grade 3 (Ekundina et al., 2021).
Analysis
Results were presented in figures and tables; pictures (micrographs) were also used where necessary. MSH2 and MSH6 staining was evaluated using regular light microscope at x100 and x400.
Photomicrography
The Stained sections were examined under a LEICA research microscope (LEICA DM750, Switzerland) interfaced with digital camera (LEICA ICC50). Digital photomicrographs of stained sections for the histomorphology and immunohistochemistry on the organs studied were taken at various magnifications and reported for Morphological changes.
Figure 1 is a pie-chart showing the case distribution with 15 normal cases, 25 colonic polyps cases and 25 colorectal carcinoma cases.
Table 1 showed the semi-quantitative expression of MSH2 in normal, colonic polys and colorectal cancer. Normal cases showed a positivity rate of 46%, Colonic polyps’ cases showed a positivity rate of 56%, colorectal carcinoma cases had a positivity rate of 100% as all of the cells showed significant expression.
Table 2 showed the reaction expression of MSH2 in normal, colonic polyps and colorectal cancer, where in Normal, 8 slides showed no significant reaction and 7 showed slightly significant reaction; Colonic polyps had 11 slides with insignificant reactions and 14 with slight and moderate significant reaction; Colorectal cancer had all twenty-five (25) slides showing varying degrees of significant reaction.
Table 3 showed the semi-quantitative expression of MSH6 in normal, colonic polys and colorectal cancer. Normal cases showed a positivity rate of 40%, Colonic polyps’ cases showed a positivity rate of 60%, colorectal carcinoma cases had a positivity rate of 100% as all of the cells showed significant expression.
Table 4 showed the expression of MSH6 in normal, colonic polyps and colorectal cancer, where in Normal, 9 slides showed no significant reaction and 6 showed slightly significant reaction; Colonic polyps had 10 slides with insignificant reactions and 15 with slight and moderate significant reaction; Colorectal cancer had all twenty-five (25) slides showing varying degrees of significant reaction.
Table 5 showed the mean percentage reactivity of MSH2 and MSH6 in normal, colonic polyps and colorectal carcinoma. It shows an increase in reactivity in MSH2and MSH6 from normal to colorectal carcinoma.
Figure 2 showed the mean percentage reactivity of markers in indicated cases. The results obtained showed a gradual increase in percentage reactivity in MSH2 and MSH6 from normal to colorectal carcinoma.
Figure 3 showed the H&E plates. The results obtained showed general structure stained sections of colorectal carcinoma at x100 and x400 (plate A); colonic polyps at x100 and x400 (plate B); normal at x100 and x400 (plate C). Presence of karyomegaly, Hyperchromasia, increased nuclear to cytoplasmic ratio and koliocytes.
Figure 4 showed the MSH2 Immunohistochemistry Plates. Nuclear MSH2 stained sections of colorectal carcinoma at x100 and x400 (plate A); colonic polyps at x100 and x400 (plate B); normal at x100 and x400 (plate C). Insignificant MSH2 immunohistochemical stains in normal colorectal tissue (plate C), moderate immunohistochemical staining within the nucleus of colonic polyps (plate B) and moderate to severe immunohistochemical staining in colorectal carcinoma (plate A).
Figure 5 showed the MSH6 Immunohistochemistry Plates. Nuclear MSH6 stained sections of colorectal carcinoma at x100 and x400 (plate A); colonic polyps at x100 and x400 (plate B); normal at x100 and x400 (plate C). Insignificant MSH6 immunohistochemical stains in normal colorectal tissue (plate C), moderate immunohistochemical staining within the nucleus of colonic polyps (plate B) and moderate to severe immunohistochemical staining in colorectal carcinoma (plate A).
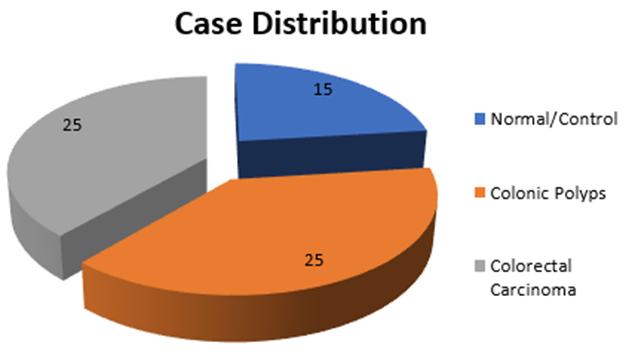
Figure 1: Pie-chart showing the case distribution with 15 normal cases, 25 colonic polyps cases and 25 colorectal carcinoma cases
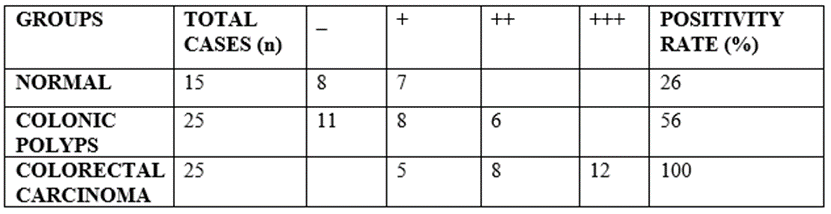
Table 1: Expression of MSH2 in indicated cases

Table 2: Reaction expression of MSH2 in indicated cases
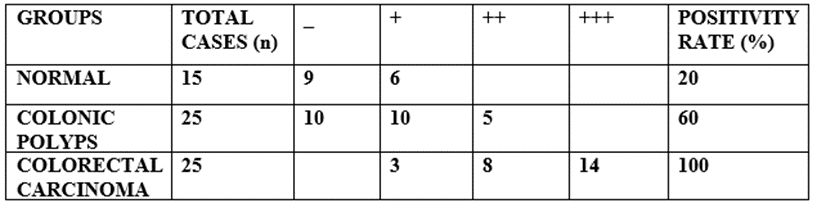
Table 3: Semi-quantitative expression of MSH6

Table 4: Reaction expression of MSH6 in indicated cases
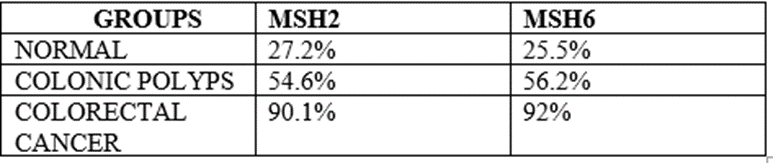
Table 5: Mean percentage reactivity of immunohistochemical markers in indicated cases
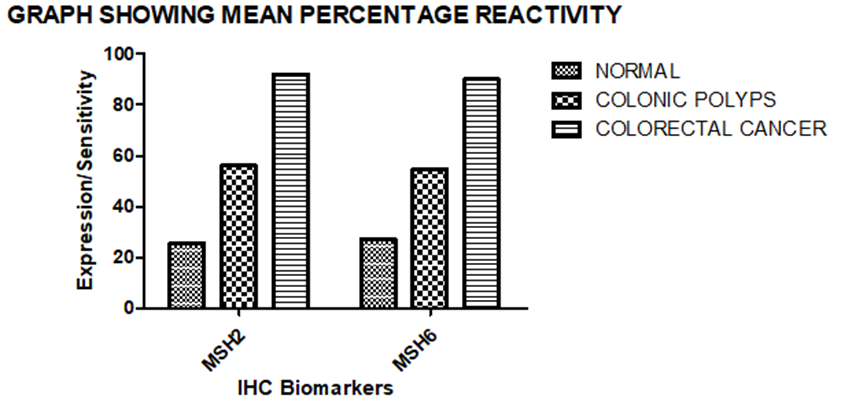
Figure 2: Mean percentage Reactivity of IHC biomakers
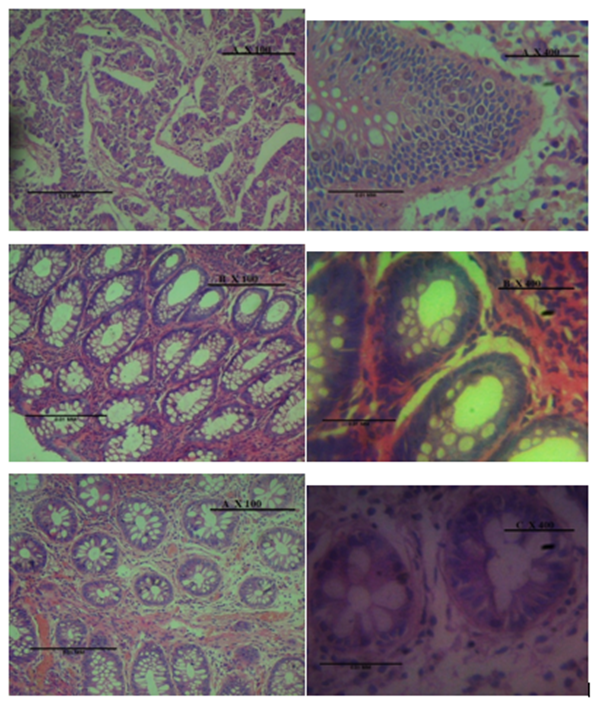
Figure 3: H&E Plates
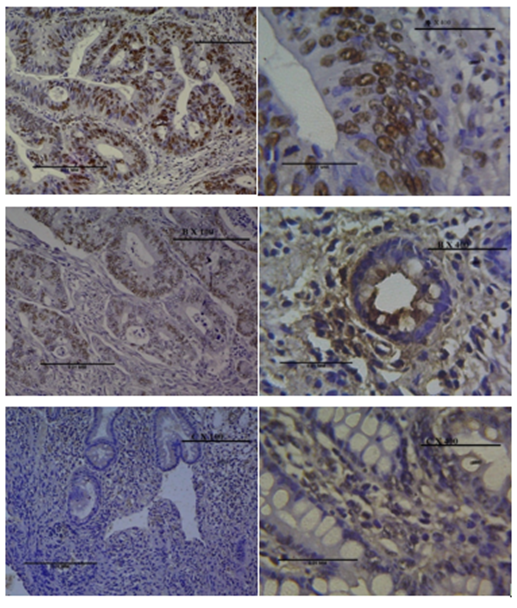
Figure 4: MSH2 Immunohistochemistry Plates
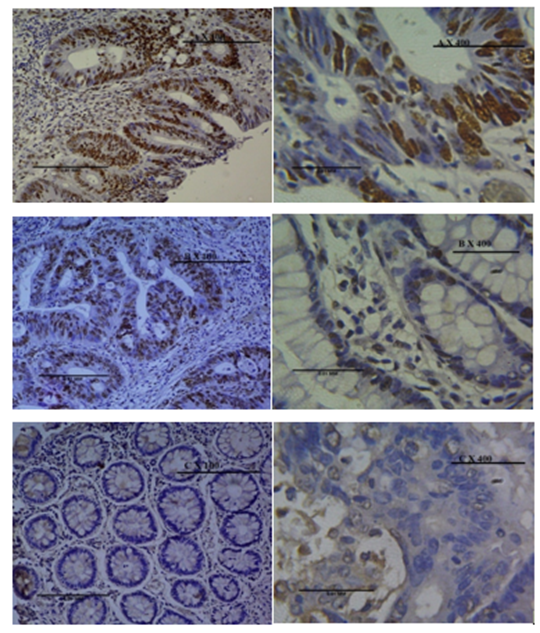
Figure 5: MSH6 Immunohistochemistry Plates
From this retrospective study, the findings revealed that MSH2 and MSH6 is expressed significantly in colorectal cancer cases with high immunohistochemical expression and degree of reactivity while in the normal colorectal tissue and colonic polyps, weak immunohistochemical staining was observed within the nucleus and classified as negative and mild respectively. The positivity rate of MSH2 among the cases was forty-six (46%) in normal, fifty-six percent (56%) in colonic polyps and one hundred percent (100%) in colorectal carcinoma and the mean percentage reactivity was 43.2%, 56.6% and 90.1% in normal, colonic polyps and colorectal carcinoma respectively, while the positivity rate of MSH6 among the cases was forty percent (40%) in normal, fifty percent (50%) in colonic polyps and one hundred percent (100%) in colorectal carcinoma and the mean percentage reactivity was 40.5%, 56.2% and 92% in normal, colonic polyps and colorectal carcinoma respectively. This expressions is in agreement with Arshita et al. [ 11] which shows that with increase in reactivity the more severe the colorectal case and also confirms that MSH2 protein performs its function by forming a heterodimer complex with MSH6 (MutSα) or with another alternative pair MSH3 (MutSβ). Lack of MSH2 expression can occur due to mutations of MSH2 and EpCAM (epithelial cellular adhesion molecule) genes. Meanwhile, MSH6 can only be expressed when it forms a pair with MSH2 because MSH6 has a special intrinsic ATPase activity for binding to MSH2. In addition, MSH2 mutations also cause weak or unbinding to MSH6 that result in the degradation of MSH6. The negative expression of MSH6 by itself in IHC indicates the MSH6 germline mutation [11].
In order to function, MSH2 protein forms a heterodimer complex with either MSH6 (MutS) or an alternate pair, MSH3 (MutS). Mutations in the MSH2 and EpCAM (epithelial cellular adhesion molecule) genes can result in a lack of MSH2 expression. MSH6 has a unique intrinsic ATPase activity for binding to MSH2, hence it can only be expressed when it forms a pair with MSH2[12]. Moreover, MSH2 mutations result in MSH6 degradation by weakening or impairing its ability to connect to MSH2. The MSH6 germline mutation is shown by the negative expression of MSH6 by itself in IHC [13].
The proximal (cecum, ascending colon, transverse colon), distal (descending colon, sigmoid colon) regions and rectum are possible locations for tumors. The distinction between the proximal and distal regions might be challenging in some situations[14]. MSH2 MSI or MSH6 MSI was more common in patients whose tumors were in the colon. Another study revealed that the intestinal area experiences mutations more frequently than the rectum [15]. Moreover MSI-H cases were more frequent (15–20%) in patients with colon cancer than in those with rectal cancer (10%), according to Charara et al. [16]. Furthermore, MSI and hyper-mutation of the MMR, KRAS, BRAF, and PIK3Ca proteins are more prevalent in the proximal colon. It has been suggested that environmental factors like bacterial toxins or CYP450 metabolites can accelerate the rate of mutation in this area [17].
The World Health Organization suggests a two-tiered system of histological grading, with a low grade for well-differentiated and moderately differentiated adenocarcinomas (50%-100% gland formation) and a high grade for poorly differentiated adenocarcinomas (0%-49% gland formation) [18]. The majority of the individuals in this study had tumors that were well-differentiated. The outcome was consistent with Fleming et al. [19] findings, which demonstrated that almost 70% of CRC patients with adenocarcinoma fall into the group of well-differentiated tumors and have a moderate degree of differentiation. Nonetheless, the poorly differentiated tumor is typically involved in CRC cases with a propensity for MSI-H[20-21]. Although patients with poor tumor differentiation were more likely to have MSH6 MSI (OR>3), our results were consistent with this finding. According to Xiao et al. [21], people with MSI and poor tumor differentiation have higher disease free survival (DFS) than those with MSS and poor tumor differentiation by about 4 years. Lymph node metastasis is less common in MSI patients with poor tumor differentiation than it is in MSS individuals with poor tumor differentiation [21].
The majority of heritability-causing factors are still unknown and under investigation, despite the fact that multiple genome-wide association studies of colorectal cancer have effectively discovered cancer susceptibility genes that are related with colorectal cancer risk. Yet, because these patients have few adenomas and because those adenomas physically resemble random lesions, Lynch syndrome caused by a dysfunction of the DNA mismatch repair system is commonly overlooked. Microsatellite instability (MSI), a condition defined by the increase or contraction of microsatellite areas in the tumor compared with healthy tissue, is the root cause of Lynch syndrome and is identified through molecular analysis. On immunohistochemistry, these tumors exhibit a lack of mismatch repair proteins. Whereas MSI is not unique to Lynch syndrome, it is present in about 15% of sporadic colorectal malignancies [22].
MSH2 showed majorly nuclear staining across the epithelium and MSH6 showed strong nuclear staining in the epithelial cells. MSH2 and MSH6 were up regulated. The two markers showed consistency but due to fact that MSH6 is a subgroup of MSH2 it cannot function without forming heterodimer with MSH2 which makes it less reliable than MSH2. MSH2 also showed prognostic significance and is recommended to be used alongside MSH6 to aid in microsatellite instability detection. This study has established the usefulness of MSH2 and MSH6 immunohistochemical markers in studying the colorectal tissue from normal to colonic polyps and then to colorectal carcinoma.
Source of Funding
This work did not receive any funding from neither Government nor non-governmental agencies.
Conflict of Interest
The authors declare no conflict of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
