
Research Article | DOI: https://doi.org/10.31579/2637-8892/032
Department of Psychology, Oregon , USA.
*Corresponding Author: Eric Arthur Blair, Department of Psychology, Oregon, USA.
Citation: Eric Arthur Blair (2018) Immune deficiency derive a favorable response to IVIg in PANDAS, J.Psychology and Mental Health Care. 2(3); DOI: 10.31579/2637-8892/032
Copyright: © Eric Arthur Blair. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 10 May 2018 | Accepted: 21 June 2018 | Published: 06 July 2018
Keywords: pediatric autoimmune; neuropsychiatric disorder; hemolytic streptococcal infection
For two decades, pediatric autoimmune neuropsychiatric disorder associated with group a beta hemolytic streptococcal infection (PANDAS) has been treated with high-dose intravenous immune globulin (IVIg) therapy based upon the understanding that the disorder is partly due to post-infectious dysimmunity.
Introduction: For two decades, pediatric autoimmune neuropsychiatric disorder associated with group a beta hemolytic streptococcal infection (PANDAS) has been treated with high-dose intravenous immune globulin (IVIg) therapy based upon the understanding that the disorder is partly due to post-infectious dysimmunity.
Study Aims: To summarize literature cases of PANDAS treated with IVIg therapy.
Methods: A search for publications documenting the experience of PANDAS treated with IVIg therapy was carried out in the English-speaking medical literature. This yielded seven articles comprising an observational study (114 patients), a randomized control trial (9 patients), five small case series (21 patients), and a single case abstract, together documenting the experience of 145 published children who met established criteria for the diagnosis of PANDAS and were treated with IVIg therapy for neuropsychiatric symptoms. An analysis of their findings was performed contrasting and combining clinical characteristics and outcomes of cases in each study, and generalizing information with mean values for continuous variables and percentages for character values.
Results: Sixty percent of children showed overall clinical improvement, 24
A search for publications related to the case reports of children with PANDAS who underwent treatment with IVIg therapy was carried out on-line in PubMed. This yielded seven articles [8-14] to which an eighth study [15] was added. Together the papers document 145 children who met established criteria [5] for the diagnosis of PANDAS and received treatment with IVIg therapy for neuropsychiatric symptoms. The cohort of 145 children described in Table 1 was comprised of one large observational study of 114 children all of whom were treated with IVIg [15], a single randomized control trial (RCT) of nine children comparing IVIg to placebo and plasma-exchange (PE) [9], three small case series totaling 21 children [8,11-14]; and a case abstract [10]. Treatment with IVIg was generally deemed necessary because of neuropsychiatric symptoms refractory to maximal conservative management that typically included prophylactic antibiotics and psychotropic medications.
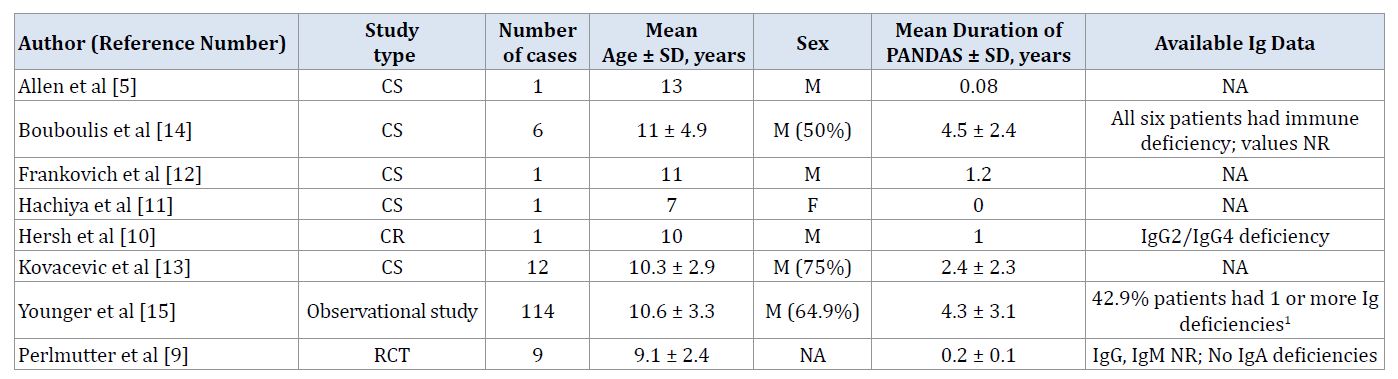
Clinical demographical characteristics at baseline such as age, sex, duration of PANDAS and IVIg treatment, dosage, regimens, and patient outcomes were abstracted in different studies and analyzed for mean values and associated percentages for continuous, categorical and discrete values.
Literature Review
Allen and colleagues [8] reported successful treatment of symptomatic tics and OCD in a child with GABHS infection complicating Tourette’s syndrome with IVIg in conjunction with penicillin prophylaxis. Perlmutter and colleagues [9] conducted a RCT comparing the outcome of OCD and tics among 29 children with PANDAS randomized to plasma exchange PE (10 children), IVIg (nine children) or saline solution placebo (10 children). The authors noted global score changes of 48% and 41% respectively at one month after treatment with 10 to 12 days of PE or 2 days of IVIg, compared to 87.5% and 77.7% in those respectively treated with PE or IVIg in open label at one year. Harsh and colleagues [10] reported a child with PANDAS in whom immunologic evaluation disclosed low IgG2/IgG4 subclass levels, suboptimal response to pneumococcal vaccine and rapid decline of pneumococcal antibody titers with low levels of proinflammatory cytokines (tumor necrosis factor [TNF]-a, interleukin [IL]1-b, and 12p40) to liposaccharide without Toll-like receptor (TLR)4 polymorphisms (Asp299Gly and Thr399lle). Treatment with IVIg was associated with near complete resolution of Sino pulmonary infection and symptoms of PANDAS. Thirty-two additional children with PANDAS treated successfully with IVIg were reported in five cases series [11-14]. Bouboulis and Mast [14] noted the favorable impact of IVIg on neuropsychiatric manifestations of PANDAS and humoral deficiency in the patients however the nature and extent of the latter was not described. Younger and colleagues [15] extended the findings of Bouboulis and Mast [14] noting low serum immunoglobulin levels in any category in 52.56%, and the favorable prognosis of children with baseline Ig deficiencies presumably in which IVIg acted as both replacement therapy and immune modulator.
Statistical Analysis
Table 1 and Table 2 summarize the clinical characteristics and outcome of the combined cohort of study patients. The male: female ratio was 1.9:1 with mean age 10.5 years, and mean duration of neuropsychiatric symptoms of 3.7 years before treatment with IVIg. Among the 145 children that comprised the study cohort, 120 (83%) received IVIg therapy at doses between 1.0 and 2.0 grams per kilogram administered every 1 to 2 months for a mean duration of 15.3 months (range 0.03 - 61.79 months) for refractory neuropsychiatric symptoms associated with PANDAS; 19 (13%) children received a single course of therapy in the first month.
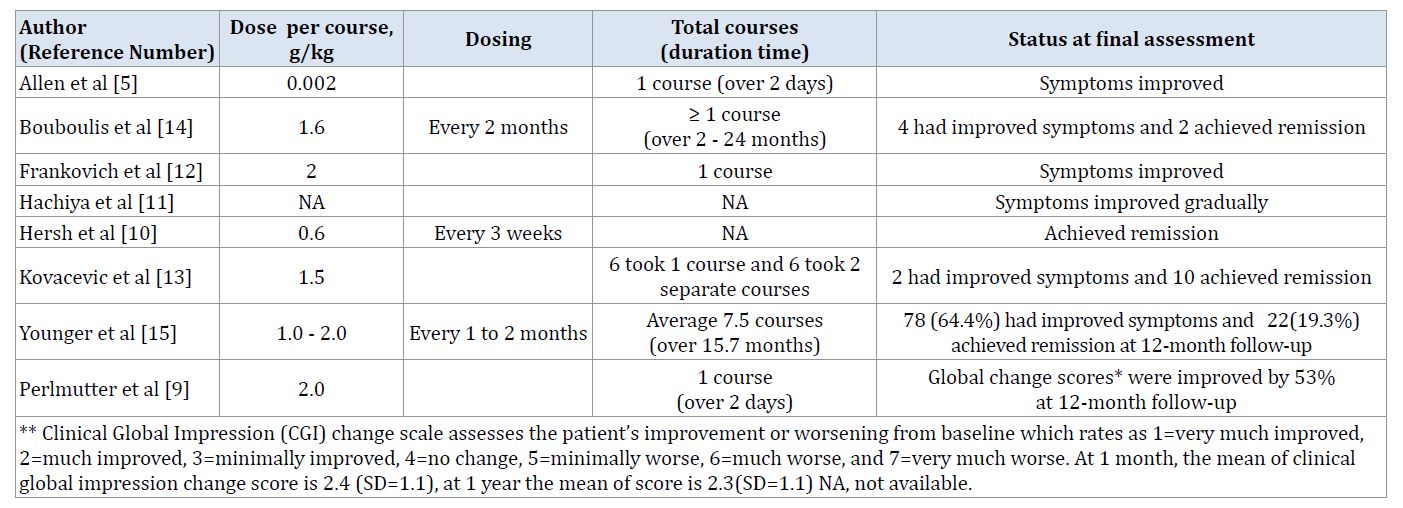
Altogether, 87 (60%) were clinically improved, 35 (24%) achieved remission, and 14 (10%) were unchanged or worse at final assessment in the one large observational study [15]. Baseline Ig levels were documented in only two studies showing low IgG subclass 2 and 4 levels [10], and low levels of serum IgG subclasses, total IgG, IgM and IgA respectively in 26.47%, 25.51%, 16.28%, and 10.48% of cases [15]. Among 114 patients [15], 49 (35%) had low baseline Ig levels. Of 22 patients (19.3%) who achieved remission, all 22 (100%) had low baseline IgG (20 patients) or IgG subclass levels (2 patients), alone (8 patients) or together (6 patients) or in association with reduced IgA or IgM levels (8 patients), indicative of humoral deficiency prior to IVIg treatment [15]. One reported patient who achieved remission [10] had combined IgG2/4 subclass deficiency.
Low levels of IgA (p < 0>
Mild adverse effects of treatment so noted in 16% of patients in the one large observational study [15] included exacerbation of migraine headache or flu symptoms at the beginning of therapy that did not preclude ongoing treatment and was generally managed with slowing the rate of infusion, vigorous hydration, or a change in IVIg product.
Intravenous Ig provides replacement Ig in immunodeficiency and immunomodulation in the treatment of inflammatory autoimmune pediatric diseases [16]. From immunodeficiency to autoimmunity, the dynamic immunologic basis of PANDAS highlights the broad potential of high-dose IVIg therapy. One small early published RCT [9] and clinically similar case reports [8;10-14] demonstrated improvement or remission similar to a recent large observational study [15] that showed benefit of IVIg for up to 84% of children with PANDAS concomitant with, or following treatment at one-year final assessment [15].
Our study had several limitations mainly associated with lack of uniformity within and among the published cases of PANDAS that precluded statistically meaningful comparisons. First, the dose, duration of treatment and timing of IVIg therapy was not uniform with some patients treated for one month and others repeatedly. Second, there was lack of uniform assessment of response to IVIg with employment of different methods of scoring. A change in a global assessment score summing OCD symptoms, tic severity, global measures of symptoms severity and psychosocial functioning were used in the RCT [9], while quartile scales of percentage improvement were employed in the observational study [15] in assessing response to treatment at one month and one-year follow-up. None of the patients described in case reports were objectively scored at onset or after one month or 12 months of treatment. Third, it was not possible to ascertain the beneficial effects of concomitantly prescribed medications such as chronic or prophylactic antibiotics or psychotropic agents in the response to IVIg. Fourth, there were no data in regard to patient's clinical status between the long intervals of assessment. Neither was it possible to ascertain whether unrelated bouts of exacerbation and improvement may have influenced the response attributed to IVIg. Fifth, with a mean treatment period of 15.7months (SD = 13.8 months) in the observational study [15], nearly half of patients were assessed while receiving IVIg leading to a possible excess of positive cases compared to those treated for a shorter time. Lastly, baseline Ig status was described in only two studies [10,15], including one that selected patients for treatment with IVIg because of immune deficiency [14] but did not provide further detailed information relevant to it.
The nosology and classification of autoimmune neuropsychiatric disorders is rapidly evolving [17], and the recognition that some affected children have infectious and immunologic triggers emphasizes the importance of new avenues of treatment. Intravenous Ig is a safe and useful adjunctive therapy in the treatment of refractory neuropsychiatric symptoms due to PANDAS and its variants. Children with PANDAS, often with baseline humoral immune deficiency derived a favorable response to IVIg in PANDAS at 12 months follow up consistent with its role in Ig replacement and immune modulation. While its use has not been substantiated in a large RCT, our findings support the use of IVIg early in the course of the disease and continued until significant improvement or remission is achieved often without serious side-effects. There is an urgent need for standardized guidelines to address the selection of patients and the most appropriate dosing regimens in those with refractory neuropsychiatric symptoms due to PANDAS.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
