
Research Article | DOI: https://doi.org/10.31579/2690-1897/111
1 Cardiac Surgery Department, BP - A Beneficência Portuguesa de São Paulo, São Paulo, Brazil.
2 Intensive Care Unit, BP - A Beneficência Portuguesa de São Paulo, São Paulo, Brazil.
3 Nephrology Department, BP - A Beneficência Portuguesa de São Paulo, São Paulo, Brazil
*Corresponding Author: Tania Leme da Rocha Martinez, Nephrology Department, BP - A Beneficência Portuguesa de São Paulo, São Paulo, Brazil.
Citation: Rodrigo Moreira Castro, Rodrigo Freire Bezerra, Luis Bongiolo Mattos, Douglas Rossoni, André Luis V Gasparoto, Anita L R Saldanha, Ana Paula Pantoja Margeotto, Raoni Imada Tibiriçá,Juliana Torres Pacheco,Tania Leme da Rocha Martinez.(2022) Immediate Extubation Versus Extubation Within Six Hours: Analysis of Clinical Outcomes in The Postoperative Period of Cardiac Surgery J, Surgical Case Reports and Images 5(2); DOI: 10.31579/2690-1897/111
Copyright: © 2021, Tania Leme da Rocha Martinez, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 20 May 2022 | Accepted: 02 May 2022 | Published: 30 June 2022
Keywords: cardiac surgery; orotracheal intubation; hospital stay; pneumonia; reintubation; ICU readmission; delirium
The advances of the quality of anesthetics and of anesthetics techniques have facilitated the optimization of time for extubation in coronary heart disease graft.
Aim: Comparison of clinical outcomes between patients extubated in the operating room and extubated patients within 6 hours after Intensive Care Unit (ICU) admission in patients undergoing cardiac surgery using extracorporeal circulation.
Material and methods: A retrospective observational study of 194 patients submitted to cardiac surgery using extracorporeal circulation in one of the biggest tertiary hospitals in São Paulo. They were divided into two groups. In the first group, patient’s extubated in the operating room was composed of 95 patients. The second group of patients extubated within 6 hours of ICU admission from the intubated operating room, composed of 99 patients. We excluded 10 patients who were extubated after 6 hours of ICU admission.
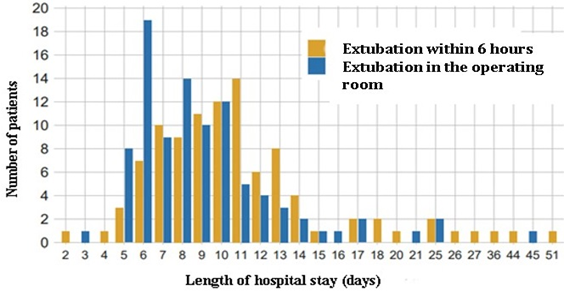
Results: Patients extubated in the operating room (median of 8 days, IQR 6 to 10) had shorter hospital stay time than patients extubated within 6 hours of ICU admission (median of 10 days, IQR 8 to 12.5), prevalence of similar delirium (2.0% x 2.1%), absence of pneumonia associated with mechanical ventilation (VAP) (0%), absence of non-caloric-protein readjustment (0%) and regarding safety, only one patient was reintubated for anesthetic recirculation in the group of extubated in the room and there was no difference in the rate of ICU readmission with the non-extubated group.
Conclusion: In this sample of patients, we found that extubation in the room was safe. Patients extubated in the operating room immediately after cardiac surgery have a lower chance of evolving with prolonged hospitalization when compared to patients who are extubated within 6 hours of ICU admission.
BMI: Body Mass Index
ICU: Intensive Care Unit
The intubation time in patients undergoing cardiac surgery alone is indicative of increased mortality [1]. Numerous studies have shown that early extubation between 6-8 hours can be safe and reduces the use of resources and hospital costs [2]. The improvement of anesthetic techniques facilitated early extubation [3] popularly known as "fast-track", the exact time of extubation in this technique is still a controversial subject, ranging from <12>
There are few services with extubation experience in the operating room, and this method is restricted for selected cases [4]. Current experience shows that extubation in the operating room did not increase the risk of reintubation, bleeding or cardiac arrhythmias [3]. In the literature, there are still few studies comparison the benefits of extubation in the room versus early extubation.
The objective of this work is to report the experience of a cardiac surgery team with extubation in the room and compare with patients extubated early in the Intensive Care Unit (ICU).
This is a retrospective, observational study conducted between August 2019 and March 2021 in one of the biggest tertiary hospitals in São Paulo.
We analyzed 194 patients submitted to cardiac surgery using pulmonary extracorporeal circulation. The patients were divided into two groups, in the first group, patients extubated in the operating room, composed of 95 patients. The second group of patients extubated within 6 hours of ICU admission from the intubated operating room, composed of 99 patients. We excluded 10 patients who were extubated after 6 hours of admission to the intensity therapy unit. The eligibility criteria in the extubation protocol in the room were: extracorporeal circulation time less than 120 minutes, smoking load less than 50 packs/year, tobacco abstinence greater than or equal to 6 months, Body Mass Index (BMI) < 30>
The exclusion criteria of the extubation protocol in the room were: bleeding above expected, presence of ventricular arrhythmias and/or gasometric changes at the desired time of extubation, need for total circulatory arrest and in those that did not fit the eligibility criteria.
The primary outcome was length of hospital stay in days. This outcome was analyzed with an ordinal logistic regression model [6], where an odds ratio (OR) lower than 1.0 means that patients in the "extubation in the operating room" group were less likely to have a longer hospital stay. In this model, the parameters age, BMI and euroSCORE II were treated as continuous covariates and adjusted using the restricted cubic spline, allowing greater flexibility in statistical modeling. Moreover, the parameters of sex, systemic arterial hypertension, diabetes mellitus and previous cardiac surgery were treated as categorical covariates and adjusted in this way.
Secondary outcomes were: [1] duration of ICU stay in days, [2] in-hospital mortality, [3] ventilator-associated pneumonia, [4] need for caloric readjustment, [5] need for orotracheal reintubation, and [6] delirium. Due to the low rate of events of these outcomes, statistical analysis was unfeasible due to low statistical power. Thus, only descriptive analysis of these outcomes was performed.
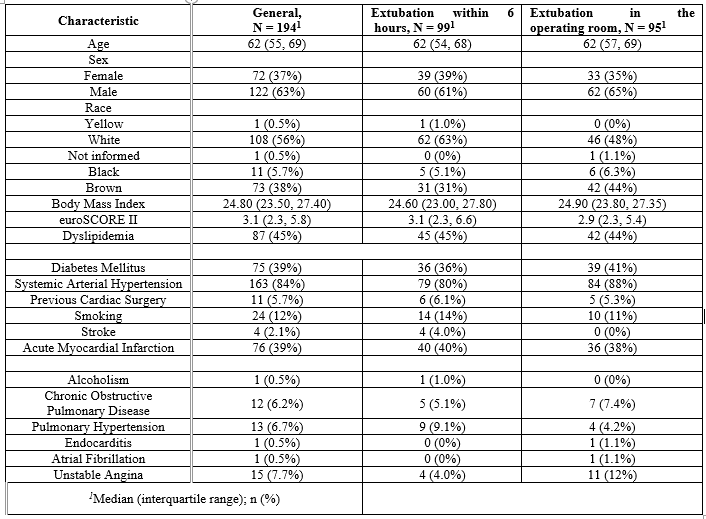
Among the patients analyzed (N=194), 122 were male (63%) and 72 were female (37%). The median age was 62 years, with an interquartile range from 55 to 69 (Table 1). The most frequent comorbidities were systemic arterial hypertension (84%), dyslipidemia (45%) and previous history of acute myocardial infarction (39%).
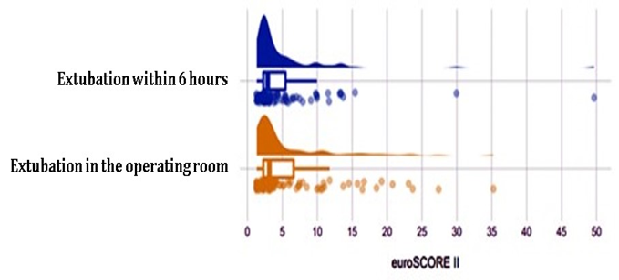
When stratified by exposure, the groups "Extubation within 6 hours" and "Extubation in the operating room" were similar in most of the baseline characteristics analyzed (Table 1). Patients extubated within 6 hours had a higher rate of preoperative pulmonary hypertension (9.1% vs. 4.2%), but lower rate of unstable angina (4% vs. 12%). Euro SCORE II was heterogeneous in both groups (Figure 1). However, the medians and interquartile intervals were similar (Table 2, Figure 1).
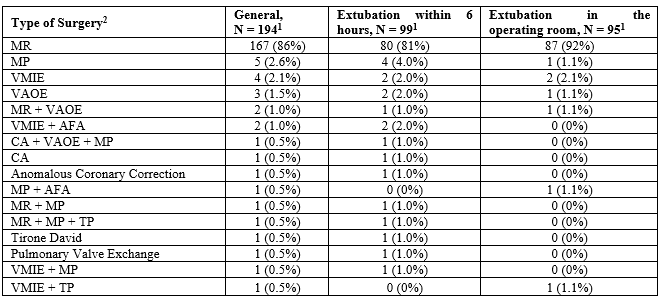
Seventy different types of surgery were performed (Table 2). The most common was myocardial revascularization (92% in the "Extubation in the operating room" group vs. 81% in the "Extubation within 6 hours" group). The other surgeries were less frequent.
1 number (%)
Subtitle: AFA: Atrial Fibrillation Ablation; CA: Correction of Ascending Aortic Aneurysm; MP: Mitral Plasty; MR: Myocardial Revascularization; TP: Tricuspid plasty; VAOE:Valvar Aortic Exchange; VMIE: Valvar Mitral Exchange.
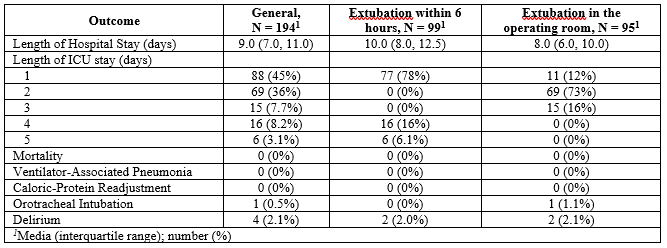
The length of hospital stay was shorter in patients who underwent extubation in the operating room (median of 8 days, IQR 6 to 10) compared to the other group (median of 10 days, IQR 8 to 12.5), as shown in Figure 2. In the analysis with ordinal logistic regression, the group "Extubation in the operating room" was less likely to have a longer hospitalization than the group "Extubation within 6 hours" (OR = 0.38, 95% confidence interval = 0.22 to 0.65, P value = 0.0004).
The length of ICU stay ranged from 1 to 5 days. The prevalence of delirium was similar between groups (2.0% x 2.1%). Only 1 patient was reintubated by anesthetic recirculation in the group of extubated in the operating room. There were no deaths, pneumonia associated with mechanical ventilation and caloric-protein readjustment
Although the literature shows that early extubation in patients undergoing cardiovascular surgery is safe and cost-effective, there is still a question not discussion fully answered regarding how early extubation should be. Intubation time is the strongest predictor of 30-day and 1-year mortality among patients with ischemic heart failure undergoing coronary artery
bypass grafting (CABG). Combining intubation time with other mortality risk factors may allow the identification of patients at the highest risk for whom the development of specific strategies may improve outcomes [7].
It is possible to observe in our study that both immediate extubation in the operating room and early extubation within 6 hours of ICU admission are safe, provided that the established criteria are respected. Previous studies have shown that immediate extubation in the operating room may or may not benefit patients after cardiovascular surgery [8,9]. Royse et al. did not observe reintubation in 100 patients extubated in the operating room [10,9]. Horswell et al., showed a 1.6% rate of reintubation for non-respiratory problems in 514 patients evaluated [9]. Our data corroborate the existing literature, because only 1.03% (N=1) of the extubation group in the operating room had to be reintubated.
Montes et al [11]. had a reintubation rate in extubated patients in an operating room of 8% and acute myocardial infarction of the postoperative period of 3%. This study was conducted in 2000, which demonstrates that the advancement of anesthetic techniques in recent years increased safety in early extubation.
Our study demonstrated that patients extubated in the operating room are less likely to have a prolonged hospitalization than patients who are extubated within 6 hours of ICU admission in the postoperative period of cardiac surgery. In the other adverse outcomes, we did not observe differences between the groups, such as ICU stay, presence of delirium, pneumonia associated with mechanical ventilation and the need for caloric-protein readjustment.
Immediate extubation in the operating room after cardiovascular surgery, provided that the eligibility criteria are met, is safe, and may decrease the hospital stay, when compared to early extubation by up to 6 hours in the ICU. In this set of patients the authors confirm the safety of immediate extubation. There were only significant differences as to hospital stay duration.
None.
No conflict of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
