
Research Article | DOI: https://doi.org/10.31579/2834-5142/021
1 Nephrology Department, Aristide Le Dantec University Hospital, Cheikh Anta Diop University, Dakar, Senegal
2 Nephrology Department, Dalal Jam Hospital, Cheikh Anta Diop University, Dakar, Senegal
*Corresponding Author: FAYE Maria, Department of nephrology, Aristide Le Dantec University Hospital, 30, Avenue Pasteur, BP: 3001, Dakar, Senegal.
Citation: Maria Faye, Ahmed T. Lemrabott., Moustapha Faye, Hussein Khadra, Mansour Mbengue. et all (2022). Hypertensive Nephropathy: Prevalence, Patient’s Profiles and Evolution in a University Hospital at Dakar. International Journnal of Clinical Nephrology. 4(2); DOI:10.31579/2834-5142/021
Copyright: © 2022 Maria Faye. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 17 December 2021 | Accepted: 30 May 2022 | Published: 10 June 2022
Keywords: hypertensive nephropathy; high blood pressure; chronic kidney disease; dakar; benign nephroangiosclerosis: prevalence; patients et evolution profiles dans un chu dakar
Background: Hypertensive nephrosclerosis is chronic impact of high blood pressure on the kidney. The objective of this study was to determine prevalence, clinical presentation, and evolution of hypertensive nephrosclerosis in patients admitting in our service.
Patients and Methods: We performed a retrospective, descriptive and analytical study in nephrology department of Aristide Le Dantec University Hospital in Dakar during a period of 05 years. Patients with long-term hypertension, hypertensive retinopathy, left ventricular hypertrophy, and progressive kidney failure were included.
Results: 461 patients were included. Hospital prevalence was 7.7%. Mean age was 56.95±13.23 years and sex ratio was 1.07. Uncontrolled high blood pressure has been found in 400 patients. Mean systolic blood pressure was 168.34 ± 27.57 mmHg. Mean diastolic blood pressure was 97.28±19.59 mmHg. On the urine dipstick, 44 patients had proteinuria (<2cross). Mean GFR, was 22.02±17.78 ml/min. Antihypertensive treatment was administered as bitherapy in 232 patients (50.3%). On admission, 47 patients (10.2%) had already started dialysis. At 12 months, 406 patients were regularly followed. Blood pressure was normal in 138 patients and serum creatinine decreased in 74 patients.
Advanced age (p=0.0001) and female gender (p =0.0001) were correlated with a low level of GFR. The high 24 hours proteinuria level was unfavorable factor on GFR (p = 0.004).
Conclusion: This study shows a high prevalence of hypertensive nephropathy in our study population. His evolution to end stage of kidney disease is inevitable, hence the importance of prevention and early management of hypertension in black subjects
Hypertensive nephrosclerosis is an important public health problem. It is resulting from long-standing hypertension untreated or poorly treated but its pathogenesis and pathophysiology are incompletely understood. Incident cases of ESRD attributed to hypertension continue to rise and are associated with significant morbidity and mortality, mostly due to cardiovascular complications. In the United States, hypertensive nephropathy is for about 27.5% of incident dialysis patients annually; it is also the second cause of end-stage renal disease (ESRD) [1]. Worldwide, the reported prevalence of hypertensive nephropathy varies, reportedly accounting for 27% of new ESRD patients in France, 21% in Italy, 7% in China, 6% in Japan and about 12% in the European Dialysis and Transplantation Association (EDTA) registry [2].
Due to the increasing morbidity and mortality and escalating costs associated with end-stage renal disease (ESRD), novel therapeutic strategies are needed urgently to maximally control blood pressure, and delay progression of hypertensive nephropathy to ESRD [1]. In Africa luck of data on hypertensive nephrosclerosis is noted.
It is in this context that this study was performed to evaluate the prevalence of hypertensive nephrosclerosis in Dakar and to determine the clinical-biological, therapeutic and evolution of this nephropathy.
Patients and Methods:
This is a retrospective, descriptive and analytical study in nephrology department of Aristide Le Dantec University Hospital in Dakar, from January 1, 2007 to December 31, 2016. All patients who received during this period with diagnosis of hypertensive nephropathy were included. The diagnosis of hypertensive nephrosclerosis was based on history, physical examination, urinalysis and serologic testing. So patients with long-term hypertension, hypertensive retinopathy, left ventricular hypertrophy, minimal proteinuria, and progressive kidney failure were included. We analyzed demographic, clinical, biological and therapeutic data. We also studied the evolution of these patients in terms of blood pressure and renal function at 6 months and 12 months.
Statistical analysis of data
The data was collected on a pre-established form. They were entered with Sphinx software version 5.1.0.2. Data analysis was performed with SPSS (Statistical package for Social Sciences) software version 18. The descriptive study was carried out with the calculation of frequencies and proportions for the qualitative variables and the calculation of means, standard deviation for the quantitative variables.
The analytical study was done with cross tables. To compare the frequencies, we used Pearson's chi-square test or Fisher's two-tailed exact test according to their conditions of applicability; the comparison of the means was made with the analysis of variance test with a threshold of significance p ≤ 0.05.
During the study period, 5978 patients were admitted to the nephrology department, including 461 cases hypertensive nephropathy (hospital prevalence of 7.71%). The mean age of patients was 56.95 ± 13.23 years. The 50-59 and 60-69 age groups were the most affected. Men were predominant (51.8%), with an M / F sex ratio of 1.07. The majority of patients came from the rural area (67.9%). Three hundred and ninety-one patients (84.82%) were referred for impaired renal function. Hypertension was known in 435 patients (94.36%) and 60 patients (13.02%) presented type 2 diabetes (Table 1).
On admission, 101 patients (21.9%) presented edema and 195 patients (42.3%) had anemia. Uncontrolled high blood pressure has been found in 400 patients. The mean systolic blood pressure was 168.34 ± 27.57 mmHg [range: 100 and 250 mmHg]. The mean diastolic blood pressure was 97.28 ± 19.59 mmHg [range 60 and 160 mmHg] (Table 1).
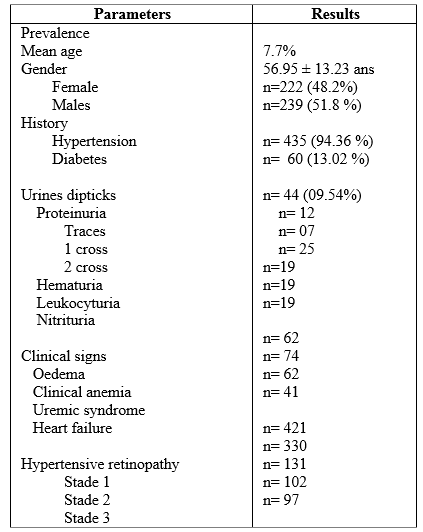
Fifty-seven patients (14.3%), had hypertension grade 1, 111 patients (27.8%), had hypertension grade 2. On the urine dipstick, 44 patients had proteinuria (<2cross>
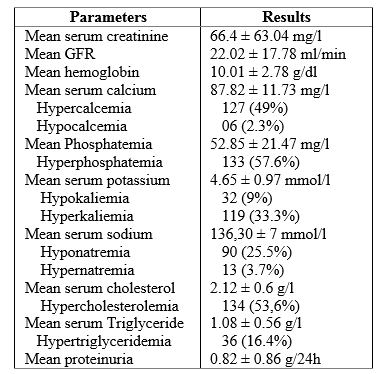
The mean serum urea was 1.23 ± 0.93 g/l [range of 0.14 and 6 g/l]. The mean serum creatinine was 66.4 ± 63.04 mg/l [range: 16.00 and 379.05 mg / l]. The mean GFR, estimated according to MDRD was 22.02 ± 17.78 ml/min [range: 1 and 56 ml/min] (Table 2).
A total of 244 patients (53%) were in stage 3, 105 patients (22.7%) in stage 4 and 112 patients (24.3)%) in stage 5 of chronic kidney disease.
On laboratory, anemia was found in 295 patients (74.3%), hyponatremia in 90 patients (25.5%), hyperkalaemia in 119 patients (33.3%) and hyperglycemia in 28 patients (11, 3%). One hundred and twenty-seven patients presented hypocalcaemia (49%) and 133 hyperphosphatemia (57.6%). Hypercholesterolemia was present in 134 patients (53.6%). HDL cholesterol was low in 79 patients (34.2%). LDL cholesterol was elevated in 66 patients (29.5%). Hypertriglyceridemia was present in 36 patients (16.4%). The mean proteinuria was 0.82 ± 0.86 g/24h [range: 0 and 2.37 g / 24h] (Table 2).
Nineteen cases of urinary tract infection were identified and Escherichia coli was the most common germ.
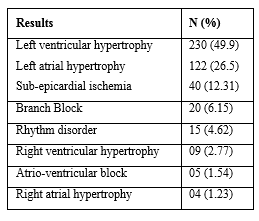
Renal ultrasound showed in 60 patients normal sized kidneys with poor cortico-medullary differentiation. In 176 patients small and poorly differentiated kidneys were found. On the electrocardiogram, left ventricular hypertrophy (LVH) and right ventricular hypertrophy (HAG) were found in 230 (49.9%) and 122 patients (26.5%), respectively (Table 3).
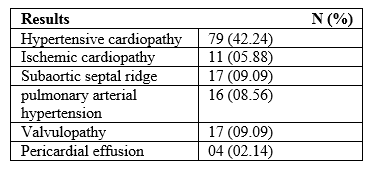
On cardiac ultrasound, 79 patients (42.24%) presented hypertensive heart disease and 11 patients or 5.88% presented ischemic heart disease (Table 4).
Basically, 70 patients (46.7%) had stage 1 hypertensive retinopathy, 77 patients (51.3%) had stage 2 hypertensive retinopathy.
Renal biopsy was performed in 7 patients. The indication in all patients was proteinuria greater than 2g/24 h in diabetes patients without diabetic retinopathy. The results concluded in all patients microscopic lesion like hyalinosis of afferent arterioles, glomerular ischaemia with retraction of the glomerular tuft with focal or global sclerosis, and interstitial fibrosis and tubular atrophy in some areas.
For treatment, antihypertensive drugs were administered as monotherapy in 92 patients (20%), as bitherapy in 232 patients, (50.3%), 114 patients (24.7%) were on tritherapy. ACE inhibitors and calcium channel blockers (CIs) were administered to 291 patients (63.1%), and 385 patients (83.5%) respectively. At admission, 47 patients (10.2%) had already started dialysis.
In terms of progression, at 6 months, 424 (92%) patients were regularly followed. For blood pressure (BP), evolution was favorable in 108 cases with BP numbers in the targets. For serum creatinine, evolution was favorable in 241 patients (57%) with 185 cases of stabilized serum creatinine and 56 (13.2%) cases of decrease serum creatinine. One hundred and eighty-three patients (43%) had a decrease in GFR with 15 new dialysis patients. Ten deaths were recorded (Table 5).
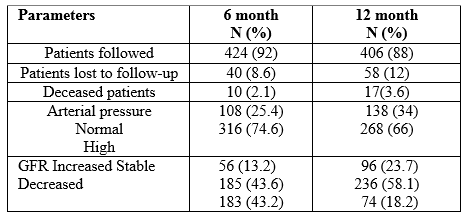
At 12 months, 406 patients were regularly followed. Blood pressure was normal in 138 patients. It remained consistently elevated in 268 patients. Serum creatinine decreased in 74 patients and stable in 236 patients. We recorded 7 more deaths (table5).
In bivariate analysis, advanced age was correlated with a low level of GFR (p = 0.0001), as was female gender (p = 0.0001). High level of proteinuria was an unfavorable factor of decreasing GFR (p = 0.004). Hypertension was not correlated with the level of GFR (p = 0.692). There was no correlation between stabilization of blood pressure and progression of GFR (p = 0.491).
During study period, 461 patients were admitted in our department for hypertensive nephrosclerosis with a hospital prevalence of 7.7%. This prevalence is lower than that of a study carried out in Mali in 2007 (12.9%) [3].
Worldwide, the reported prevalence of hypertensive nephropathy varies, reportedly accounting for 27% of new ESRD patients in France, 21% in Italy, 7% in China, 6% in Japan and about 12% in the European Dialysis and Transplantation Association (EDTA) registry [2]. This variation may reflect differences criteria and accuracy for diagnosis of hypertensive nephropathy [1]. The mean age of our study population was 56.95 ± 13.23 years. The 60-69 age group was the most representative at 27.5%. These results are in conformity with those of Touré [3] and Ndiaye [4] who found respectively an average age of 57 years and 53.23 years. In Burkina Faso, Tiendrebiogo [5] found an average age of 42.1 ± 11.4 years. In China, Kou [6] found an average age of 44.4 ± 10.7 years. In our series, we note male predominance with a sex ratio of 1.07. This male predominance of hypertensive nephropathy appears to be a constant [3, 4, 5, 7]. It could be explained by the fact that in these countries, men have more access to health care because their economic level is higher.
However, the opposite trend has been observed in France [8] and in the black American population [9].
Renal impairment was the most frequent reason for consultation in our series with 391 patients (84.82%). This result is similar with the findings of Coulibaly [10] but he found a lower rate (57.7%).
In terms of short-term evolution, our study had shown a decrease in blood pressure in 25.4% of cases. We noted a decrease in serum creatinine in 13.2% of cases. Our results differed from those of Ndiaye [4] who found normalization of blood pressure levels in 60% of patients and a drop in serum creatinine in 47.36% of patients.
This difference is probably due to the fact that our patients already had a very advanced stage of chronic kidney disease.
At 12 months, 55 patients (12%) were lost to follow-up. This could be explained by the high cost of care, but also by the difficulty of access to health structures.
In our study, there was a statistically significant association between gender and the level of GFR (p = 0.0001). There were more women than men in stage 5. Age was statistically correlated with GFR (p = 0.0001). In fact, the average age of the patients increased as the GFR decreased. Our results were consistent with the literature. In a study by Vikse, [11] age was a predictive factor in the development of GFR. Another study, by Klag [12] had shown that age and male gender were major factors associated with the development of CRD. Proteinuria was a factor in the progression of glomerular filtration rate. It was statistically significantly correlated with progression to CKD (p = 0.004). Our results corroborate with a number of studies in the literature. Vikse [11] had shown that proteinuria was a predictor of the pejorative development of hypertensive nephropathy and / or mortality.
This study shows a high prevalence of hypertensive nephropathy in our study population. His evolution to end stage of kidney disease is inevitable, hence the importance of prevention and early management of hypertension in black subjects
All authors declare no interest conflicts.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
