
Research Article | DOI: https://doi.org/ 10.31579/2640-1045/033
1 Department of Endocrinology,USA.
*Corresponding Author: Reshad Hassannezhad, Department of Endocrinology,USA
Citation: Reshad Hassannezhad, Hyperketonemia: Clinical features and diagnosis of Diabetic Ketoacidosis. J. Endocrinology and Disorders. Doi:10.31579/2640-1045/033
Copyright: © 2018. Reshad Hassannezhad. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 19 September 2018 | Accepted: 02 October 2018 | Published: 08 October 2018
Keywords: DKA Treatment; Insulin; Prevention
Diets that boost ketone production are increasingly used for treating several neurological disorders. Elevation in ketones in most cases is considered favorable, as they provide energy and are efficient in fueling the body's energy needs.Several physiological and pathological triggers, such as fasting, ketogenic diet, and diabetes cause an accumulation and elevation of circulating ketones. Complications of the brain, kidney, liver, and microvasculature were found to be elevated in diabetic patients who had elevated ketones compared to those diabetics with normal ketone levels.
Diabetic ketoacidosis is an acute metabolic complication of diabetes characterized by hyperglycemia, hyperketonemia, and metabolic acidosis. Hyperglycemia causes an osmotic diuresis with significant fluid and electrolyte loss. DKA occurs mostly in type 1 diabetes mellitus (DM). It causes nausea, vomiting, and abdominal pain and can progress to cerebral edema, coma, and death. DKA is diagnosed by detection of hyperketonemia and anion gap metabolic acidosis in the presence of hyperglycemia. Treatment involves volume expansion, insulin replacement, and prevention of hypokalemia.
Diabetic ketoacidosis (DKA) is a rare yet potentially fatal hyperglycemic crisis that can occur in patients with both type 1 and 2 diabetes mellitus. Due to its increasing incidence and economic impact related to the treatment and associated morbidity, effective management and prevention is key. Elements of management include making the appropriate diagnosis using current laboratory tools and clinical criteria and coordinating fluid resuscitation, insulin therapy, and electrolyte replacement through feedback obtained from timely patient monitoring and knowledge of resolution criteria. In addition, awareness of special populations such as patients with renal disease presenting with DKA is important. During the DKA therapy, complications may arise and appropriate strategies to prevent these complications are required. DKA prevention strategies including patient and provider education are important. This review aims to provide a brief overview of DKA from its pathophysiology to clinical presentation with in depth focus on up-to-date therapeutic management.
Pathophysiology
Diabetic ketoacidosis arises because of a lack of insulin in the body. The lack of insulin and corresponding elevation of glucagon leads to increased release of glucose by the liver (a process that is normally suppressed by insulin) from glycogen via glycogenolysis and also through gluconeogenesis. High glucose levels spill over into the urine, taking water and solutes (such as sodium and potassium) along with it in a process known as osmotic diuresis.This leads to polyuria, dehydration, and polydipsia. The absence of insulin also leads to the release of free fatty acids from adipose tissue (lipolysis), which are converted through a process called beta oxidation, again in the liver, into ketone bodies (acetoacetate and β-hydroxybutyrate). β-Hydroxybutyrate can serve as an energy source in the absence of insulin-mediated glucose delivery, and is a protective mechanism in case of starvation. The ketone bodies, however, have a low pKa and therefore turn the blood acidic (metabolic acidosis). The body initially buffers the change with the bicarbonate buffering system, but this system is quickly overwhelmed and other mechanisms must work to compensate for the acidosis.
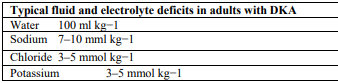
In various situations such as infection, insulin demands rise but are not matched by the failing pancreas. Blood sugars rise, dehydration ensues, and resistance to the normal effects of insulin increases further by way of a vicious circle.As a result of the above mechanisms, the average adult with DKA has a total body water shortage of about 6 liters (or 100 mL/kg), in addition to substantial shortages in sodium, potassium, chloride, phosphate, magnesium and calcium. Glucose levels usually exceed 13.8 mmol/L or 250 mg/dL.
Diagnosis of DKA followed the criteria of the ISPAD. Blood samples were taken on admission for clinical chemistry and full blood count. An acid-base status was assessed by capillary blood gas analysis. Urine ketones were measured by reflection photometry Siemens, Germany) with a detection limit of 15 mg/dl.
Patients were treated according to a written in-house protocol which followed the ISPAD consensus guidelines 2000 and its updates:
a)Fluid replacement:Intravenous fluid substitution was started with normal saline solution (NaCl 0.9 %). When blood glucose level fell below 250 mg/dl, it was changed to half-electrolyte solution (NaCl 0.45 % / Glucose 5 %).
b) Insulin administration:A dilution of regular insulin was administered intravenously at 1 IU/ml by an infusion pump. The initial substitution dose varied between 0.05 and 0.1 IU/kg/h. A reduction in blood glucose between 50 and 100 mg/dl/h was achieved by adapting insulin and fluid infusion rates. Intravenous insulin application was switched to subcutaneous insulin application once ketoacidosisresolved (pH ≥ 7.3) and the patients returned to a stable clinical condition.
c) Potassium replacement: Potassium was administered from the beginning of insulin treatment when oliguria and hyperkalemia were excluded. We started an overall substitution of 2 to 3 mmol/kg/24h. Potassium substitution was administered continuously by a separate infusion pump,which allowed adjustment of replacement independently of the fluid replacement. The substitution dose was adjusted hourly depending on the serum potassium levels.
d) Correction of acidosis:Correction of acidosis was performed by substitution of insulin and fluid alone. The use of sodium bicarbonate was considered only in case of decreased cardiac contractility or life-threatening hyperkalemia. The blood pH level did not serve as criteria for the use of bicarbonate.
e) Monitoring:Vital signs and ECG were monitored continuously. Capillary blood gases as well as blood glucose and electrolytes were initially checked every hour.
Treatment
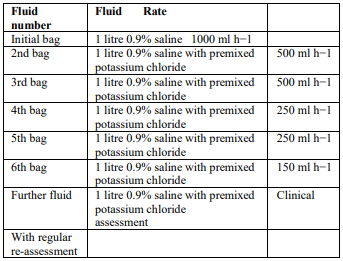
The therapeutic goals of DKA management include optimization of 1) volume status; 2) hyperglycemia and ketoacidosis; 3) electrolyte abnormalities; and 4) potential precipitating factors. The majority of patients with DKA present to the emergency room. Therefore, emergency physicians should initiate the management of hyperglycemic crisis while a physical examination is performed, basic metabolic parameters are obtained, and final diagnosis is made. Several important steps should be followed in the early stages of DKA management:
collect blood for metabolic profile before initiation of intravenous fluids;
infuse 1 L of 0.9% sodium chloride over 1 hour after drawing initial blood samples;
ensure potassium level of >3.3 mEq/L before initiation of insulin therapy (supplement potassium intravenously if needed);
Initiate insulin therapy only when steps 1–3 are executed.
Correction of hyperglycemia and Acidosis
Hyperglycemia is corrected by giving regular insulin 0.1 unit/kg IV bolus initially, followed by continuous IV infusion of 0.1 unit/kg/h in 0.9% saline solution. Insulin should be withheld until serum potassium is ≥ 3.3 mEq/L ( Hyperosmolar Hyperglycemic State (HHS) : Treatment). Insulin adsorption onto IV tubing can lead to inconsistent effects, which can be minimized by preflushing the IV tubing with insulin solution. If plasma glucose does not fall by 50 to 75 mg/dL (2.8 to 4.2 mmol/L) in the first hour, insulin doses should be doubled. Children should be given a continuous IV insulin infusion of 0.1 unit/kg/h or higher with or without a bolus.
Ketones should begin to clear within hours if insulin is given in sufficient doses. However, clearance of ketones may appear to lag because of conversion of beta-hydroxybutyrate to acetoacetate (which is the “ketone” measured in most hospital laboratories) as acidosis resolves. Serum pH and bicarbonate levels should also quickly improve, but restoration of a normal serum bicarbonate level may take 24 h. Rapid correction of pH by bicarbonate administration may be considered if pH remains < 7>
Hypokalemia prevention
Hypokalemia prevention requires replacement of 20 to 30 mEq potassium in each liter of IV fluid to keep serum potassium between 4 and 5 mEq/L. If serum potassium is < 3> 5 mEq/L, Potassium supplementation can be withheld.
Initially normal or elevated serum potassium measurements may reflect shifts from intracellular stores in response to acidemia and belie the true potassium deficits that almost all patients with diabetic ketoacidosis have. Insulin replacement rapidly shifts potassium into cells, so levels should be checked hourly or every other hour in the initial stages of treatment.
Complications
Hypoglycemia is the most frequent complication of DKA and can be prevented by timely adjustment of insulin dose and frequent monitoring of blood glucose levels. Hypoglycemia is defined as any blood glucose level below 70 mg/dL. If DKA is not resolved and blood glucose level is below 200–250 mg/dL, decrease in insulin infusion rate and/or addition of 5% or 10
Monitoring and replacement of electrolytes
Initial serum potassium may be normal, raised or low in DKA. However, there is a total body potassium deficit. Potassium loss is caused by a shift from the intracellular to extracellular space in exchange for hydrogen ions which accumulate in acidosis. The extracellular potassium is then lost through osmotic diuresis.
The initial litre of fluid should not have potassium added. Provided the serum potassium is <5>
Adequate fluid, potassium and insulin therapy will resolve the acidosis in DKA, but there may be disturbances of other electrolytes including bicarbonate, sodium, and phosphate. Generally, these electrolyte imbalances improve as the DKA is treated effectively. Typical fluid and electrolyte deficits are summarized in (Table 2)
Pathophysiology-driven DKA management is complex and requires careful selection of approaches aimed at restoring deficiencies in insulin, fluids, and electrolytes. Available clinical practice recommendations and guidelines offer solid foundations for achieving successful DKA resolution. However, we advise that individualized decisions should be made, as DKA patients may have unique clinical and biochemical characteristics. Safe strategies to restore volume deficit and replace insulin should be implemented, with frequent evaluations of the patient’s status aimed at monitoring for DKA resolution and avoiding potential complications. Recent studies showing clinical benefits and safety of subcutaneous insulin administration in patients with mild DKA and utility of protocol-driven care offer new pathways to reducing the cost of DKA care while maintaining quality of clinical outcomes. Also, resources should be directed toward the education of primary care providers and patients and their families so that they can identify signs and symptoms of uncontrolled diabetes earlier. With the increasing focus on health disparities, access to medical care is a major focus in determining better care in diabetes, which would ultimately contribute to decreasing the occurrence of hyperglycemic crises of diabetes.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
