
Clinical Image | DOI: https://doi.org/10.31579/2690-4861/222
1 Gastroenterology department, Hotel Dieu de France Hospital, Saint Joseph University, Beirut, Lebanon
2 Medical school, Saint Joseph University, Beirut, Lebanon
3 Pathology department, Hotel Dieu de France Hospital, Saint Joseph University, Beirut, Lebanon
4 Radiology department, Hotel Dieu de France Hospital, Saint Joseph University, Beirut, Lebanon
*Corresponding Author: Rita SLIM, Gastroenterology department, Hotel Dieu de France Hospital, Saint Joseph University, Beirut, Lebanon.
Citation: SLIM R, ASSAF A, KARAM M, Smayra V, MENASSA L. (2022) Hypereosinophilia with IgG4 Associated Cholangiopathy. International Journal of Clinical Case Reports and Reviews. 11(3); DOI: 10.31579/2690-4861/222
Copyright: © 2022 Rita SLIM, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 13 May 2022 | Accepted: 16 May 2022 | Published: 24 May 2022
Keywords: IgG4 cholangitis; hypereosinophilia; sclerosing cholangitis
IgG4-related sclerosing cholangitis (IgG4-SC) belongs to the spectrum of IgG4-related disease which encompasses many medical conditions. We report a case of a 59-year-old man who presented with clinical and radiologic features of primary sclerosing cholangitis but where hypereosinophilia along with an extremely high blood level of IgG4, liver infiltration with IgG4-positive plasma cell and a spectacular response to corticoids treatment, confirmed the diagnosis of IgG4-SC.
IgG4-related disease encompasses a variety of conditions, including Mikulicz's syndrome, chronic sclerosing sialadenitis, hypophysitis, Riedel thyroiditis, chronic interstitial pneumonitis, interstitial nephritis, autoimmune pancreatitis, retroperitoneal fibrosis, sclerosing cholangitis, and lymphadenopathy. [1] The present article reports the case of a 59-year old man who presented jaundice and hypereosinophilia in the setting of IgG4-related disease.
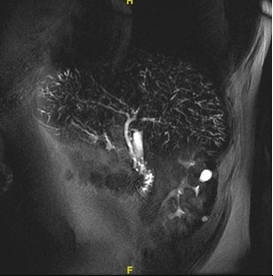
A 59-year-old man from Iraq presented with a 6 month history, of asthenia, progressive weight loss of 20 Kg, jaundice and pruritus. Laboratory tests revealed hypereosinophilia with a total count of 9680, elevated creatinine (212 µmol/l), with cholestasis (GGT = 770 U/L, alkaline phosphatase = 706 U/L, and Bilirubin level at 3.7 mg/dl). A non-enhanced MRCP showed a normal common bile duct with mild dilatation of the intrahepatic bile ducts and a diminished arborization of the biliary tree (FIG 1). Viral, autoimmune and metabolic workup was strictly normal. A bone marrow biopsy was performed to rule out a hypereosinophilic syndrome. It only revealed hypercellularity with eosinophilia. Stool analysis for parasitic infection and serologies for Fasciola hepatica, Distomatosis and Toxacara canis were negative.
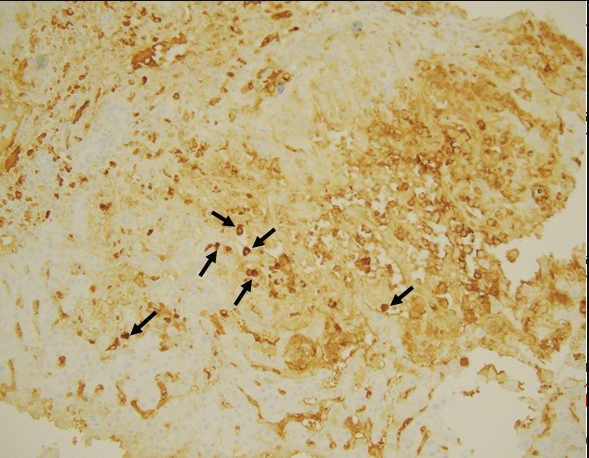
Subsequently, the patient underwent liver biopsy. Microscopic examination of the liver biopsy showed portal tracts edema, mixed inflammatory infiltrate with numerous plasma cells and neoductular proliferation. On immunostaining, the plasma cells were positive for IgG4. (FIG 2). IgG4
blood level was elevated to more than 6640 mg/100 mL, confirming the diagnosis of IgG4-associated cholangiopathy with hypereosinophilia as an associated feature.
Treatment with oral prednisone 0.5mg/kg/day has normalized the eosinophil count, as well the liver enzymes and the creatinine levels. Two months after starting treatment, IgG4 level fell to 992mg/100ml and eosinophils count normalized. The patient was kept on maintenance therapy with Azathioprine 50 mg/day and 5 mg/day of prednisone.
IgG4-related sclerosing cholangitis (IgG4-SC) belongs to the spectrum of IgG4-related disease which encompasses many medical conditions with the Type 1 autoimmune pancreatitis, the most common associated condition [1]. Five histological patterns are described in IgG4-SC: portal inflammation, large bile duct obstructive features, portal sclerosis, lobular hepatitis and canalicular cholestasis in perivenular areas [2]. More than 10 IgG4 -positive plasma cells/HPF is a commonly used threshold to suggest the diagnosis. A high IgG4 level can be observed in cholangiocarcinoma, primary sclerosing cholangitis (PSC), atopic dermatitis, and other cholangio-pancreatic malignancies. However, a cutoff level fourfold higher than the upper limit of normal had 100% specificity for IgG4-SC. Moreover, Torre et al revealed that peripheral hypereosinophilia and elevated serum IgE levels may be present in 27% and 35% of patients respectively. These two features are not related to atopy but inherent to IgG4 disease itself (3).
The clinical, biological and MRI features in our patient, couldn’t discern between IgG4-SC and PSC especially in the absence of any features of autoimmune pancreatitis. Liver infiltration with IgG4-positive plasma cell as well as the extremely high blood level of IgG4 and the spectacular response to corticoids treatment, confirmed the diagnosis of IgG4-SC
The present case illustrate well the fact that hypereosinophilia is a feature of IgG4 related disease.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
