
Research | DOI: https://doi.org/10.31579/2693-4779/055
*Corresponding Author: Anthony Kodzo-Grey Venyo. North Manchester General Hospital, Department of Urology, Delaunays Road, Crumpsall, Manchester, United Kingdom.
Citation: Anthony K-G Venyo. (2021) Hydatid Cyst of the Breast: A Review and Update of the Literature. Clinical Research and Clinical Trials. 4(2); DOI: 10.31579/2693-4779/055
Copyright: © 2021 Anthony Kodzo-Grey Venyo, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 02 July 2021 | Accepted: 06 August 2021 | Published: 16 August 2021
Keywords: hydatid cyst of breast; echinococcus; eosinophilia; mammogram; ultrasound scan of breast; computed tomography scan; magnetic resonance imaging; complete excision; recurrence; spillage; rupture, albendazole
Hydatid cyst of the breast is a rare infection of the breast that tends to be reported sporadically in Echinococcus infection endemic areas; nevertheless, because of increasing global travel hydatid cyst of the breast may be encountered in a non-endemic area of the world where clinicians may not be familiar with the manifestation and biological behaviour of the disease. Hydatid cyst of the breast has been reported sporadically in females whose ages have ranged between 16 years and 87 years and these cases only represent 0.27% of all cases of hydatid cyst encountered globally. Hydatid cyst of the breast does present as a lump/mass in the breast which quite often tends to be painless but it could be associated with pain/discomfort. Hydatid cyst of the breast tends to present insidiously and the lump tends to be present for a long time before attention is sought by the patient because it had behaved innocuously and had either been growing slowly with a recent noticeable increase in size over a few months. A history of previous contact with dogs and sheep as well as present or previous residence in an echinococcus endemic area tends to be helpful in alerting the clinician to the possibility of the diagnosis of hydatid cyst. A past history of treatment for echinococcal infection elsewhere in the body would also be helpful in alerting the clinician to the diagnosis of the disease. There tends to be no family history of breast cancer, and no history of previous hormone replacement therapy. The general and systematic examinations of most of the patients tend to be normal unless they have other non-related medical conditions. Clinical examination usually tends to reveal a swelling that tends to be well-circumscribed with clear margin that may be non-tender but at times there may be tenderness associated with the lump. The clinical examination findings tend to be non-specific and would usually mimic fibroadenoma, phyllodes tumour, or intra-cystic carcinoma of the breast. Usually the results of routine haematology and haematology blood tests would tend to be normal unless there is a non-related disease but there could be eosinophilia. Echinococcus hemagglutination test and Elisa test for Echinococcal IgE test would tend to be positive in cases of hydatid cyst of the breast. Various radiology imaging modalities tend to be utilized to assess hydatid cyst of the breast including mammogram, ultrasound scan of the breast, computed tomography (CT) scan of the breast, thorax, and abdomen, magnetic resonance imaging (MRI) scan of breast, thorax, and abdomen. Diagnosis of hydatid cyst of the breast tends to be diagnosed by undertaking fine needle aspiration biopsy of the breast lesion for cytology/histopathology examination or histopathology examination of excised hydatid cysts of the breast. Successful treatment of hydatid cyst of the breast requires complete excision without spillage of the hydatid cyst and additionally to minimise recurrence of disease Albendazole medication tends to be given. When there is spillage of the hydatid cyst or rupture of the hydatid cyst during the process of the excision, a thorough lavage of the operating field and excision of the surrounding tissue to ensure any possible residual daughter cysts are completely removed and utilization of Albendazole medicament would help to minimize or avoid development of recurrence. Because of the possibility of recurrence of disease a period of follow-up assessment with clinical examination and radiology imaging assessment as well as echinococcus hemagglutination tests would be recommended.
Masroor et al [1], Stated that Echinococcal (hydatid) cysts do represent a manifestation of infestation at a larval stage at the larval stage of Echinococcus granulosus and that Echinococcosis is caused by the larval stage of tapeworms. Four species of Echinococcus exist and out of these four species of Echinococcus granulosus, most of the human being infections are attributable to Echinococcus granulosum which does cause cystic Echinococcus. Echinococcus multilocularis does cause alveolar disease which tends to be encountered less frequently in human beings. It has been iterated that with regard to cystic echinococcus, the human being tends to be an aberrant host and does get infected by the oral ingestion of excreta from an infected dog [2].
It has been documented that hydatid cyst has been encountered in all continents globally with the highest prevalence in parts of Eurasia especially within the Mediterranean countries, the Russian Federation, as well as its adjacent states and also in China; North and East Africa; Australia; and South America [1, 3]. The commonest organs of the body that tend to be infected by hydatid cyst include the liver which occurs in 75% of cases, the lungs in 15% of cases, and only 10% of hydatid cyst infections occur in other organs of the body [1,4,5]. It has been iterated that the breast is a rare site for the development of hydatid cyst, which does constitute 0.27% of all cases of hydatid cyst affecting human beings [1, 6].
Hydatid cyst of the breast could manifest as a well-circumscribed lesion for which the differential diagnosis does include: a simple cyst within the breast, fibroadenoma, phyllodes tumour, as well as intra-cystic carcinoma [1]. It has been stated that within endemic areas, hydatid cyst of the breast should be a differential diagnosis of well-circumscribed breast masses [1] It has also been recommended that in view of increasing travel between countries globally it would be important that hydatid cyst of the breast is regarded as a differential diagnosis of well-circumscribed breast lesions in echinococcal infection non-endemic countries of the world [1]. It has additionally been iterated that a global high index of suspicion of hydatid cyst of the breast is required in order to avoid complications and morbidity that tends to be associated with an undiagnosed case of hydatid cyst of the breast.
Considering that hydatid cyst of the breast is uncommon in many parts of the world majority of clinicians in the non-echinococcus infection endemic areas may probably be unfamiliar with the manifestations and treatment of this rare disease. In view of the increasing global travel, there is the likelihood that patients who have hydatid disease of the breast might present to a clinician in a non-endemic area. For this reason it is important for all clinicians globally to be aware and familiar with the manifestation, diagnosis and treatment of the disease.
The ensuing article contains a review and update of the literature on Hydatid cyst of the breast which has been divided into two parts: (A) Overview of the literature which has discussed general aspects of Echinococcus infection and Hydatid cyst and (B) miscellaneous narrations and discussions related to some case reports, case series and studies related to hydatid disease of the breast.
To review and update the literature on hydatid disease of the breast.
Internet data bases were searched including Google, Google scholar, Yahoo, and PUBMED. The search words that were used included: Hydatid cyst of the breast; Echinococcal infection of the breast, Echinococcus granulosis infection of the breast, Hydatid cyst of the mammary gland, Echinococcus infection of the mammary gland. Eighteen references were identified which were used to write the article that has been divided into two parts (A) Overview which has discussed general aspects of Echinococcus infection including hydatid cyst of the breast and (B) miscellaneous narrations and discussions related to some case reports, case series, and studies related to hydatid cyst of the breast.
Results / Review and Update of Literature
(A) Overview
General Comments / Definition
Echinococcal cyst of the breast refers to infestation of the breast by the larval form of Echinococcus granulosus [7].
Even though Hydatid cyst of the breast is rare, it has been recommended that hydatid cyst of the breast should be considered in the differential diagnosis of breast masses within Echinococcus Granulosus endemic areas.
Terminology
Echinococcal cyst of the breast is also referred to as Hydatid cyst of the breast [7].
Epidemiology
It has been documented that Echinococcal infection of the breast does occur worldwide but it does tend to occur especially within sheep rearing communities [7].
It has been stated that hydatid cyst of the breast does affect women whose ages have ranged between 30 years 50 years [7]. Despite this it would be envisaged that hydatid cyst of the breast could affect women of any age group in sheep rearing echinococcal infection communities of the world.
It has been documented that Hydatid cyst does most commonly affect the liver and the lung [7].
It has been stated that hydatid cyst of the breast does constitute 0.27% of cases of hydatid cysts generally [7].
Ouedraogo reported the largest series of hydatid cyst of the breast which were encountered between 1969 and 1982 [7, 8].
Pathophysiology
It has been documented that the definitive host for Echinococcal organism is the dog and that the intermediate host of the organism is the sheep [7].
Aetiology
It has been stated that the consumption of soil, food, or water which has been contaminated by faeces of a dog which has been infected by Echinococcus granulosum does lead to infestation by the larval forms of Echinococcus granulosus [7].
Presentation
It has been stated that hydatid cyst of the breast may present as a slow-growing breast lesion/lump/mass [7].
It has been documented that hydatid cyst of the breast could simulate fibroadenoma, phylloides, or on rare occasions it could mimic intra-cystic carcinoma of the breast [7].
It has been iterated that hydatid cyst of the breast could become infected and that infected hydatid cyst of the breast could tend to be indistinguishable from a breast abscess with regard to the radiology imaging features of the disease [7].
Diagnosis
The ensuing summations have been made relating to the diagnosis of hydatid cyst of the breast: [7].
It has been stated that with regard to the diagnosis of hydatid cyst of the breast, a high degree of suspicion would be required.
The diagnosis of hydatid cyst of the breast would require:
Evidence of peripheral eosinophilia. Upon blood test.
Evidence of positive echinococcal antigen immunofluorescence test.
Evidence of positive hemagglutination test.
A history of exposure of an individual to Echinococcus within an echinococcal endemic area of the world would provide a clue to the diagnosis hydatid cyst of the breast in association with a breast lesion/mass/swelling.
Laboratory investigations
Urine examination
Urinalysis, urine microscopy and urine culture that are routinely undertaken in the general assessment of patients who have hydatid cysts of the breast but the results would not be diagnostic of the disease but if there is evidence of urinary tract infection, it would be treated appropriately based upon the antibiotic sensitivity pattern of the organism that is cultured to improve upon the general condition of the patient.
Haematology blood test
Full blood count and coagulation screen are general assessments that are undertaken in cases of hydatid cysts of the breast and this would tend to show evidence of eosinophilia but this would not be diagnostic of the disease but within echinococcus endemic areas eosinophilia would tend to make the clinician have a high index of suspicion for the disease.
Biochemistry blood tests
Serum urea and electrolytes, estimated glomerular filtration rate, liver function tests, and blood glucose are general tests that are undertaken for the assessment of individuals who have hydatid cysts of the breast but the results would not diagnose the disease. Nevertheless, if there is any impairment in the biochemistry test, it would be investigated appropriately and treated to improve upon the general condition of the individual.
Serum Echinococcus hem agglutination test
Serum Echinococcus hem agglutination test is an investigation that is undertaken and when it is positive it would lead the clinician to consider the diagnosis which can be confirmed by pathology examination of the breast lesion [7].
Elisa test for Echinococcal IgE
Elisa test for Echinococcal IgE is an investigation that is undertaken and when it is positive it would lead the clinician to consider the diagnosis which can be confirmed by pathology examination of the breast lesion [7].
Radiology investigations
Mammography
Mammography tends to be undertaken in cases of breast lumps or suspected breast lesions as initial screening assessment tests to ascertain if there are any abnormal areas to be suspicious of malignancy and in cases of hydatid cysts of the breast, mammography would tend to show: [7].
Well-circumscribed breast lesions.
Oval or spherical densities.
The breast lesions would usually be associated with smooth lobulated margins.
Peripheral calcification may be seen in hydatid cyst of the breast.
Ultrasound scan of the breast
It has been stated that that several classic signs of hydatid cyst of the breast upon ultrasound scan of the breast have been described including: [7, 9, 10].
Double wall sign in which the hydatid cyst wall is seen as 2 echogenic areas.
Snowstorm sign which is seen as a result of movement of scolices within the hydatid cyst.
Waterlily sign which is seen because of floating membranes due to detached endocyst / daughter cyst.
Scroll sign due to the folding of the detached endocyst.
Computed tomography (CT) scan
CT scan can be utilized to provide detailed features of hydatid cyst of the breast and CT scan of thorax, abdomen and pelvis with also indicate whether or not there other hydatid cyst lesions anywhere else within the thorax, abdomen and pelvis and CT scan of thorax, abdomen and pelvis would establish whether or not there is a recurrent hydatid cyst lesion in the breast, thorax or abdomen.
Magnetic resonance imaging scan
MRI scan can be utilized to provide detailed features of hydatid cyst of the breast and MRI scan of thorax, abdomen and pelvis with also indicate whether or not there other hydatid cyst lesions anywhere else within the thorax, abdomen and pelvis and MRI scan of thorax, abdomen and pelvis would establish whether or not there is a recurrent hydatid cyst lesion in the breast, thorax or abdomen.
MRI scan of the breast can establish if there is infection within the hydatid cyst of the breast.
Prognostic factors
The prognostic factors associated with the treatment of hydatid cysts of the breast have been summarized as follows: [7].
Complete excision of hydatid cyst of the breast tends to be curative.
It has been documented that the recurrence rate of hydatid cyst of the breast has ranged between 7% and 14% of cases.
It has been noted that spillage of protoscolices during the process of surgical excision of hydatid cyst of the breast could lead to implantation of the Echinococcal disease.
It has been stated that pursuant to surgical excision of hydatid cyst of the breast serological titres could fall slowly and that a positive serological titre may not imply recurrence of hydatid cyst of the breast but rising serological titres would be suggestive of recurrent hydatid disease of the breast.
Treatment
The approach to the treatment of hydatid cyst of the breast has been summarized as follows: [7].
Complete surgical excision of hydatid cyst of the breast is the treatment that is undertaken.
Pre-operative albendazole could be given in order to reduce the size of the hydatid cyst of the breast pre-operatively.
Microscopic histopathology features [7].
The microscopy examination features of hydatid cyst of the breast have been summated as follows: [7].
Microscopy examination of hydatid cyst of the breast does show a cyst which is comprised of 3 layers: [7].
The outermost peri-cyst which is a fibrous layer.
The middle ectocyst layer which is laminated, hyaline and acellular.
The inner endocyst which is the germinative layer that consists of daughter cysts and brood capsules with scolices.
There could be granulomatous palisading reaction and pseudocyst formation as is visualised in cutaneous lesions.
Cytology examination features
It has been stated that examination of aspiration of hydatid cyst may produce specimen that yield clear fluid that contain particulate material which could contain scolices with hooklets which tend to be PAS and acid fast positively stained as well as bits of the laminated membrane [7].
Differential diagnoses
Some of the documented differential diagnoses of hydatid cyst of the breast include the following: [7].
Granuloma annulare which tends to be characterised by palisading granulomatous inflammation predomination.
Pseudocyst / fibrous capsule which tends to be due to previous surgical procedure, trauma or foreign body and in which no trilaminar cyst wall is seen upon microscopic examination as well as in which there in no PAS positive staining material.
(B) Miscellaneous narrations and discussions from some case reports, case series and studies related to hydatid cyst of the breast
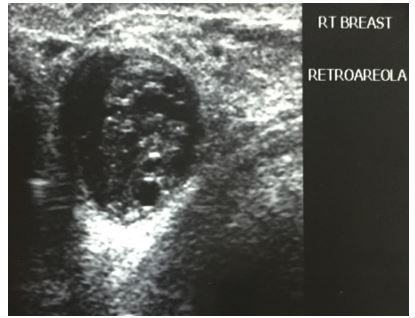
Singh et al [11]. reported a 24-year-old lady who had presented with a right-sided painless, palpable, cystic lump in the breast which was superior to the nipple within the retro-areolar region for 6 months, which was surgically excised. On examination Singh et al. [11] did find a linear incision mark over the right breast of the patient which was superior to her nipple (see figure 1).

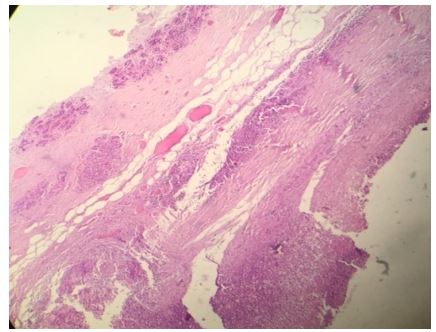
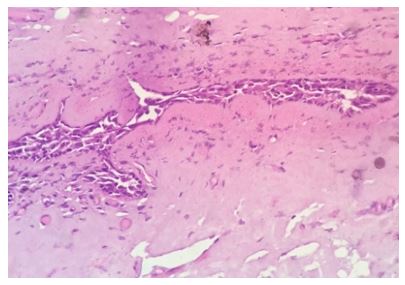
She had pre-operative ultrasound scan of the breast which showed a round hypo-echoic lesion (see figure 2). Histopathology examination of the excised specimen showed a cyst that contained folds of laminated chitinous layer which was partly lining the wall of the cyst and the encompassing areas did show chronic inflammation with sheets of foamy macrophages (see figures 3 and 4). The microscopic examination of the specimen also showed foreign body giant cell reaction as well as occasional ill-formed granuloma and the surrounding normal breast tissue was also visualised (see figures 5 and 6). She was sent for further treatment.


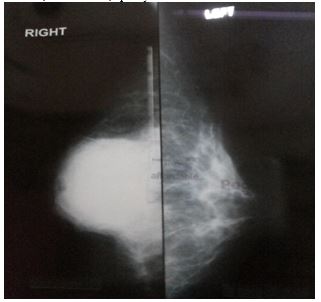
Kumar et al. [12] reported a 31-year-old lady who had presented with a gradually progressive, painless lump within her right breast over a period of one year. She did not have any past medical history of injury, discharge from her nipple, or a family history of carcinoma of the breast. She was a housewife who did not disclose having had any close contact with any animal. She was found upon examination to have a non-mobile, firm lump that measured 5 cm x 5 cm within the sub-areolar region of her right breast which was predominantly located within the upper quadrants of the breast. The nipple of her right breast was noted to be retracted. The left breast and nipple were found on examination to be normal and there was no evidence of axillary or cervical lymph adenopathy. She had mammogram which showed a large, smooth walled, well-defined, opacity in the right sub-areolar region (see figure 7). The left breast was normal. She had ultrasound scan of her breasts which showed a thick walled cystic lesion with floating membranes as well as internal echoes within the sub-areolar region of her right breast. She also had chest x-ray and ultrasound scan of her abdomen and which were normal. She underwent excision of the right breast lump in which the right breast lump was removed completely via a curvilinear incision just above the areolar margin (see figures 8 and 9). The excised cyst was found on gross examination to be oval in shape and it had measured 5 cm x 4.5 cm x 3 cm. upon opening of the cyst, endocysts were visualised which did confirm that the cyst was a hydatid cyst (see figure 10).



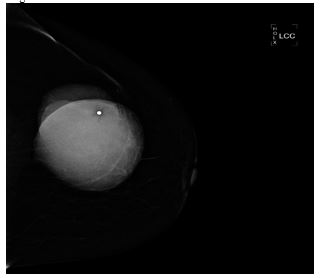
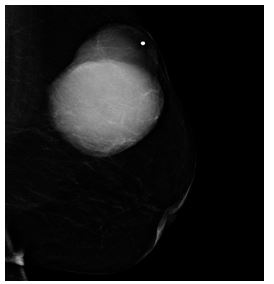
Alamer et al. [13] reported a 66-year-old lady who was known to have hypertension and diabetes mellitus who had presented with a palpable mass within her left breast that was associated with pain over a period of a long time. She did not have any nipple discharge or fever. She also did not have any history of breast trauma, hormone replacement therapy, or a family history of carcinoma of the breast. Her clinical examination showed a large palpable mass which was identified within her left breast with regular borders. Her nipple, areolar, and skin were normal. There was no evidence of palpable lymph node enlargement in her left axilla. Her general examination, systemic examinations and examination of her right breast and right axilla were normal. The results of her investigations including haematology blood tests, biochemistry blood tests, and chest x-ray were normal except elevated serum glucose result. She had a mammogram which showed a large oval and dense mass in the upper outer quadrant of her left breast (see figures 11 and 12). The mass was noted to be lobulated and well-circumscribed in its contours and to have measured 9.2 cm x 7.5 cm. No microcalcification was noted. The nipple, areolar, and skin were normal. The axillary lymph nodes were normal and the right breast was normal. Based upon the mammography examination features of the lump an impression of an usual large dense mass within her left breast was made and coded as BIRAD4A, taking into consideration the age of the patient, and further assessment with ultrasound scan was recommended. The differential diagnoses that were considered included: Phyllodes tumour, pseudo-angiomatous stromal hyperplasia (PASH), and well circumscribed carcinoma of the breast.
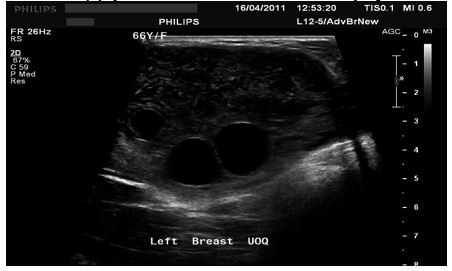
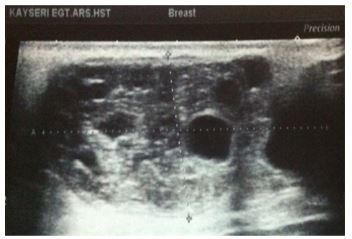
She had ultrasound scan of the breast which showed a large heterogeneous and lobulated mass within the upper quadrant of her left breast which had corresponded to the mammographic features. Few internal anechoic cysts were visualized within the peripheral aspects of the breast lesion. Doppler interrogated images did not show any internal vascularity within the mass (see figures 13, 14, and 15). There were no enlarged associated axillary lymph nodes found. She had ultrasound scan-guided biopsy from the lesion. She did have computed tomography (CT) scan for further assessment of the breast lump which did reveal a large hypo-dense mass within her left breast. It also revealed very tiny and thin internal septations were visualized. There was no peripheral enhancement and no internal enhancement. The mass did measure 6.8 cm x 6.2 cm x 9 cm in maximum dimensions (see figures 16 and 17). No axillary lymph nodes were found. The rest of the intra-thoracic and abdominal structures were found to be normal. Pathology examination of the biopsy specimen showed scanty material which had consisted of fragmented eosinophilic membranes that had laminated appearance in keeping with the diagnosis of hydatid cyst. A final diagnosis of hydatid cyst of the breast was made. The patient was referred to the surgeons for surgical excision of the hydatid cyst of the breast at the time of the report of the article. The lesson that needs to be learnt from this case report is the fact that diagnosis of hydatid cyst can be established pre-operatively with careful history taking, clinical examination radiology imaging including ultrasound scan, CT scan, and ultrasound scan-guided biopsy for histopathology/cytology examination which would guide the surgeon to undertake a careful complete surgical excision of the without spillage of the contents of the hydatid cyst.




Alam and Goel [14] reported a 24-year-old lady who had presented with a history of a painless lump of two months duration. She did not have any past history of trauma, discharge of pus, itching, loss of weight, fever, or hormonal treatment. She did not have any family history of carcinoma of the breast. She had had fine needle aspiration from her right breast lump which upon pathology examination was diagnosed as cysticercosis of her right breast. Her clinical examination had demonstrated a 5 cm x 4 cm mass within the upper inner quadrant of her right breast, which was firm, non-tender, mobile, and associated with a clearly defined margin as well as the overlying skin was found to be normal. The left breast was found on examination to be normal. Both of her nipples were normal and she did not have any axillary or supra-clavicular lymph node enlargement. She had chest radiograph which was normal. Her abdominal examination was normal. The results of her blood tests were normal. The lump was excised surgically and the specimens were submitted to the pathology department as two separate tissues of which one was solid and the second one was a pearly white cystic piece of tissue. Upon gross examination, the solid piece of tissue did measure 4 cm in its maximum dimension with a firm greyish-white cut surface. The second piece of tissue was pearly white, semi-translucent and shiny inner surface which gave it a boiled egg albumin-like appearance that measured 6 cm in length and which was unilocular. Microscopy examination of the solid tissue revealed breast lobules that contained mild round cell infiltrates here and there. At one edge was found a dense infiltrate which had consisted of round cells, many eosinophils, and some neutrophils and also at the free border of the section, there were many protoscolices of larva of Echinococcus granulosus and in some scolices, hooklets were visualised. Sections from the membranous tissue revealed classical laminated wall of the cyst and also the germinal layer from which many brood capsules that contained had arisen. Based upon the pathology features of the specimen a diagnosis of hydatid cyst of the right breast was made. The original FNA slides which had been diagnosed as cysticercosis were requested for and re-examined and pathology examination of the specimen showed hooklets of the parasite. She was discharged on the 3rd post-operative day and failed to attend for follow-up.
Moazeni-Bistgani [15] reported a 61-year-old lady who did not have any significant past medical history who had presented with a mass within her right breast that was associated with pain. She stated that she had noticed a small mass within her right breast just pursuant to completion of breast feeding, and since then the mass had gradually increased in size over a period of 25 years. She did not have any nipple discharge, fever, history of trauma to the breast, hormone replacement therapy, or a family history of carcinoma of the breast or ovarian carcinoma. She had had close contact with sheep and dogs. She had a clinical examination which showed a large palpable mass that had regular borders within her right breast. Her nipple, areola, and skin were found to be normal upon examination. Examination of her right axilla was normal. Her left breast and axilla were normal, and her systematic examinations were normal. She had mammograms which revealed two, including a large and a small, oval and dense masses in the upper outer quadrant of her right breast. The largest mass measured 4 cm x 3 cm and multi-lobulated, and the small mass measured 1 cm x 1 cm that was well-circumscribed with regard to its contours. Calcifications were found at the periphery of the large lesion as well as diffuse linear micro-calcifications within other areas of the breast. The left breast was normal. She had ultrasound scan of the breast which showed a large heterogeneous and lobulated mass which contained mixed hypoechoic and hyperechoic degenerative contents with a small internal anechoic cyst within the periphery of the lesion within the upper outer quadrant of her right breast. The axillary lymph nodes were not enlarged. The results of her haematology and biochemistry blood tests were normal. The results of her Echinococcus hemagglutination test was positive. She had a chest x-ray as well as ultrasound scan of abdomen and pelvis which were normal. She underwent complete excision of the cyst in her right breast without spillage of the contents upon suspicion of hydatid cyst in view of the fact that she came from an Echinococcus epidemic area. When the cyst was opened, endocysts were visualised which confirmed the diagnosis of hydatid cyst. Pathology examination of the specimen showed eosinophilic membranes that had a laminated features and massive calcifications that had been considered to be characteristic for the diagnosis of hydatid cyst of the breast. The case was reported without any follow-up information. A lesson learnt from this case report is that the presentation of hydatid cyst of the breast could be insidious and could be diagnosed 25 years after the onset.
Masroor et al. [1] reported a 20-year-old Afghanistan lady who had presented with a lump within her left breast for 3 years, which had gradually increased in size and had become painful. Her clinical examination had shown that the overlying skin of her left breast was erythematous, and the lump was tender upon palpation, as well as there was thickening of the skin in association with peau d’orange as well as within the upper half of the left breast a palpably lumpy area was identified. She had ultrasound scan of the breasts which showed a well-defined lesion within the upper outer quadrant of her left breast that was cystic with echogenic debris and a thick echogenic area in the dependent position as well as many swirling membranes. A provisional diagnosis of left breast abscess was made. An incision and drainage of the abscess was undertaken under general anaesthesia in the operating theatre and clear fluid was aspirated during the procedure. The cyst was excised intact and the wound was packed pursuant to irrigation with normal saline. During the post-operative period the patient was put on albendazole and a daily dressing of the wound with 4% formalin. Histopathology examination of the specimen confirmed the diagnosis of hydatid cyst of the left breast with daughter cysts. Pursuant to removal of the cyst the lady developed wound dehiscence for which she underwent wound debridement under general anaesthesia and a corrugated drain was left in situ. She was put on albendazole 400 mg. The lady was put on three cycles of albendazole 400 mg four times per day for two weeks. She had post-operative chest x-ray and ultrasound scan of abdomen which were normal. She had ultrasound scan of the breast at her 1-month follow-up which was normal. She had remained disease-free for three years pursuant to treatment of her hydatid cyst of the left breast at the time of publication of the case report. The lesson to learn from this case report is that wound dehiscence can develop pursuant to excision of hydatid cyst which is followed by careful follow-up assessment of the patient and the wound to exclude wound dehiscence could be a way of ensuring recurrence of hydatid cyst of the breast is avoided or detected early.
Erkan et al. [16] reported a 38-year-old woman who had presented with a 6-month history of epigastric pain which had been associated with nausea and vomiting. She did not have any history of weight loss, jaundice, abuse of alcohol, abdominal trauma, or previous pancreatitis or abdominal surgery. Her clinical examination was normal except for fullness of her within her epigastric area that was found. The results of her blood tests including serum amylase were normal and she had upper abdominal endoscopy which was normal. She had ultrasound scan of her abdomen which showed a multi-loculated cystic mass that measured 90 mm x 60 mm x 70 mm in diameter that was located anteriorly within the body of her pancreas. She had computed tomography (CT) scan of her abdomen which revealed a cystic mass that had internal septa that had originated from the body of her pancreas and which had bulged anteriorly and had distorted the lesser curvature of the stomach by its mass effect. The rest of the contents of the abdomen were normal. She underwent laparotomy which revealed a cystic mass that was bulging from the pancreas anteriorly and which had been encompassed by the stomach, the transverse colon, left lobe of the liver, and by the omentum. The cyst was freed from the encompassing structures. Upon puncturing of the cyst with a syringe a transparent fluid was aspirated. A scolicidal agent was introduced first based upon a suspicion of hydatid cyst of the pancreas and the cyst was opened from its anterior wall. The germinative membrane was seen and the daughter vesicles were seen which were all removed. No communication was visualised between the pancreatic duct and the cavity of the cyst. Partial cystectomy was undertaken leaving behind only the base of the adventitial cyst wall and the cavity of the cyst was obliterated with a patch of omentum. She had a post-operative CT scan of her thorax which was normal. She did receive albendazole treatment at a dose of 10 mg / kg / day for 2 months. She had remained well and she had a CT scan of her abdomen at her one year follow-up. She presented with a painless mass lesion within her left breast 18 months pursuant to her surgery. Her clinical examination showed a soft and mobile mass that measured 5 cm in size within the upper quadrant of her left breast. She had ultrasound scan of her breast which showed one large as well as one small pure cystic lesion which were adjacent to each other. She also had mammmography which showed only one pure cystic lesion within her left breast which had measured 50 mm x 50 mm. She was planned to have complete excision of the cyst but during the procedure the cyst had ruputured and the germinative layer was visualised. The area and the remaining cavity had to be irrigated immediately with a scolicidal agent. A post-operative CT scan of the thorax and abdomen which was undertaken was normal. She was treated with albendazole post-operatively for six months. She had remained well during her follow-ups without any evidence of recurrence up to her 2-year follow-up at the time of the report of her case. A lesson learnt from this case report is that Hydatid cyst of the breast can develop following successful treatment of hydatid cyst anywhere else and hence if an individual has a past medical history of treatment for hydatid cyst elsewhere and presents with a breast lump, hydatid cyst of the breast should be suspected and kept in mind as a differential diagnosis.
Charfi et al. [17] reported a 56-year-old woman who had presented with a 3 cm breast mass. She had a mammogram which illustrated a dense, well-circumscribed lesion associated with calcifications. Fine needle aspiration of the mass was undertaken and pathology examination of the specimen confirmed the diagnosis of hydatid cyst of the breast. Charfi et al. [17] stated that complete excision of hydatid cyst of the breast is the treatment of choice and that the diagnosis of hydatid cyst of the breast by means of fine needle aspiration of the breast lump is controversial.
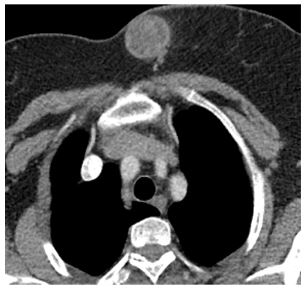
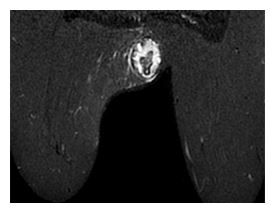
Koc et al. [18] reported a 59-year-old lady who had presented with a palpable, longstanding mass in the periphery of her left breast of more than 10 years that was remarkable for pain over the preceding 8 months. She did not have any history of trauma to her breast, hormone replacement therapy, family history of malignancy. Her clinical examination did reveal a palpable non-fixed mass on her anterior chest wall that was located peripherally in her left breast with regular borders. Her nipple, areola and her overlying skin were normal. There were no palpable lymph nodes in her axillae. The results of her routine blood tests were normal. She had mammography with craniocaudal (CC) and medial lateral oblique projections which showed a dense mass that was located peripherally at 9’oclock, and which had a regular, lobulated contour in her left breast and which did not have any identifiable micro-calcifications and macro-calcifications. (see figure 18). She had ultrasound scan of breast which showed a lesion that was compatible with a semi-solid mass, and which had smooth border as well as moderately thickened wall that measured 4.5 cm x 3.3 cm x 2.9 cm and which did contain internal detached membrane that gave an appearance of “water lily.” The lesions did contain circumferentially oriented anechoic millimetric loculations which had been divided with septae that mimicked daughter cysts. The intercystic spaces had been filled with homogenous echogenic material that amounted to hydatid sand that were predominantly seen within the centre of the lesion which had created rosette appearance that is referred to as wheel-spoke pattern (see figure 19). Doppler ultrasound scan did not reveal any internal vascularity. There was no evidence of enlarged axillary lymph nodes. She also had CT scan of thorax and abdomen which did not reveal any abnormality within the chest and abdomen with the exclusion of her left breast. The left breast lesion was found on the CT scan to be heterogenous, hypodense, as well as thick walled that was smooth and it had septae internally. The density of the lesion was 35 HU (see figure 20). She had contrast-enhanced magnetic resonance imaging (MRI) scan which provided further details related to the characteristics of the lesion including focal rupture of the cyst. Dynamic contrast-enhanced magnetic resonance imaging (MRI) (1.5 Tesla) with contrast enhancement pattern was undertaken for additional assessment as well as detailed structural analysis of the breast mass lesion. The MRI scan had demonstrated that the capsular wall of the mass was smooth as well as moderately thickened. The MRI scan also demonstrated internally scattered, mostly circumferentially oriented small loculations that had been separated with thin septae, which gave it the semblance of rosette or wheel-spoke. The non-enhancing multiloculations did have low-signal intensity upon T1-weighted images and high-signal intensity upon T2 weighted images that was compatible with the daughter cysts. The MRI scan further demonstrated intercystic spaces that had been filled with material, which was iso-intense with muscle tussue on T1-weighted images and hyper-intense upon T-2 weighted images that had been suggestive of hydatid sand. The infolded membrane that was demonstrated on the MRI scan at the inferior pole of lesion did demonstrate an appearance of “water lily” sign. The MRI scan additionally demonstrated that the capsular wall as well as the infolded membrane were iso-tense upon T1-weighted images and hypo-tense on T2-weighted images where hypo-intensity had been remarkable with Short Tau Inversion Recovery (STIR) images. The MRI scan demonstrated other features including: that the capsular wall of the lesion did enhance marginally as a smooth rim with a gradually increasing pattern, on the contrary, the internal septae as well as the detached membrane had not enhanced on dynamic T1-weighted images (see figures 21(a), 21(b), and 21(c),. Superior and Inferior pole out pouches of the mass as well as defect in the capsule at the inferior edge of the mass were observed. The mass had been outlined with a curvilinear, minimal fluid collection near the defect, which had demonstrated focal rupture of the cyst (see figure 22).
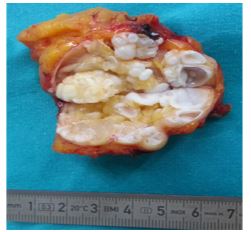
The cyst was surgically excised and the specimen did show characteristic daughter cysts of hydatid cyst (see figure 23). Koc et al. [18] made the following conclusions:
Hydatid cyst of the of the breast should be taken into consideration as a differential diagnosis of breast lumps.
Ultrasound scan and magnetic resonance imaging scan have an important diagnostic role with regard to providing additional information relating to the internal structure of hydatid cyst rather than CT scan and mammography.
STIR sequence T2-weighted MRI, especially does help in the identification of complications including rupture and secondary infection in cystic masses.



Hydatid cyst of the breast is a rare infestation that can be reported anywhere in the world because of global travel and not only in echinococcus endemic areas.
The disease does present insidiously with a swelling/mass in the breast that may be slow-growing or may be slow-growing but associated with recent more rapid increase in size.
Hydatid cyst of the breast does mimic other more common benign diseases of the breast as well as intra-cystic carcinoma of the breast.
There could be eosinophilia in some cases of hydatid cyst of the breast but quite often the results of routine haematology and biochemistry blood tests tend to be normal but Echinococcus hemagglutination test and Elisa test for Echinococcal IgE would tend to be positive.
Radiology imaging including mammogram, ultrasound scan, magnetic resonance imaging scan, and computed tomography scan tend to be undertaken in the assessment of hydatid cyst of the breast but magnetic resonance imaging scan additionally would be more effective with regard to identifying rupture of the cyst and infection of the cyst.
Confirmation of the diagnosis of hydatid cyst of the breast can be made by cytology/pathology examination of fine needle aspiration biopsy of the breast lesion or the completely excised cyst.
Complete excision of the cyst avoiding spillage does constitute adequate treatment to avoid recurrence but utilization of albendazole medicament post-operatively does ensure minimization or reduction of recurrence and at times utilization of albendazole pre-operatively could reduce the size of the cyst to allow for complete excision of the cyst.
Adequate follow-up assessments with clinical history taking and examination, blood tests, and radiology imaging would be required to ensure there is no recurrence of disease.
Acknowdledgements to:
Case Reports in Medicine Volume and Hindawi Publishing Ltd for granting copyright permission for reproduction of figures and contents of their journal to be reproduced under copyright © 2017 Ali Koc et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distrivbution, and reproduction in any medium, provided the original work is properly cited.
The Pan African Medical Journal for granting permission for reproduction of figures and images from the journal under copy right This is an Open Access article distributed under the terms of the Creative Commons Attribution License which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Accessed 2019 Aug 03
Int J. Surg. Case Rep. for granting permission for reproduction of figures and contents of the journal under copyright © 2014 The Authors. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/3.0/). https://www.ncbi.nlm.nih.gov/ pmc/articles/PMC4336384/
International Journal of Surgical Research for granting permission for reproduction of figures and contents of the journal under copyright © 2016 Scientific & Academic Publishing. All Rights Reserved. This work is licensed under the Creative Commons Attribution International License (CC BY). http://creativecommons.org/licenses/by/4.0/
None
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
