
Research Article | DOI: https://doi.org/10.31579/2639-4162/094
Hand Surgery Department, University Hospital of Martinique, Fort-De-France, 97200, Martinique, France.
*Corresponding Author: L. Stratan, Hand Surgery Department, University Hospital of Martinique, Fort-De-France, 97200, Martinique, France.
Citation: L. Stratan, M. Mastacaneanu, (2023), How the COVID 19 Pandemic Forced us to Adopt the Wide Awake Combined with Office Surgery in our Hand Surgery Department, J. General Medicine and Clinical Practice, 6(4); DOI:10.31579/2639-4162/094
Copyright: © 2023, L. Stratan. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 16 May 2023 | Accepted: 20 June 2023 | Published: 30 June 2023
Keywords: wide awake; walant; office surgery; covid 19 pandemic; ambulatory setting; hand surgery
Introduction: The COVID-19 pandemic has had a dramatic impact on hospitals worldwide. Like many others, our department was forced to halt all scheduled surgeries and transform surgical departments into COVID units. Two years later, we have still not returned to our previous "normal" activity. We, as hand surgeons, were compelled to adapt and promote ambulatory surgery, and most notably, office surgery using the WALANT (Wide awake local anesthesia with no tourniquet) techniques.
Method: We realized a monocentric retrospective study, comparing our ambulatory surgical activity two years before and after the COVID-19 pandemic was officially declared in France (16th of March, 2020).
Results: Examining hand trauma treated in Office Surgery with WALANT (Figure 2), we find that the COVID-19 pandemic did not significantly change the number of hand accidents. We managed 2097 minor hand trauma cases two years before the pandemic and 2005 patients during the two years of the pandemic. Notably, during 2020 and 2021, we treated more patients for minor hand trauma than in 2019.
On the other hand, the scheduled Office Surgery combined with WALANT increased by 235% (from 299 to 705 patients) and the whole Ambulatory Surgery by 132% (from 855 to 1135 patients) (Figure 3).
Conclusions: The COVID-19 pandemic was an opportunity for our Hand Surgery Department to transfer entirely some of the minor scheduled procedures, outside the Main OR to the Office Surgery combined with WALANT.
The COVID-19 pandemic, which began in France in March 2020, dramatically altered hospital activities [21-25, 31]. The majority of human and material resources were redirected towards addressing COVID-19 [25, 26, 27]. Consequently, the Hand Surgery Department at the University Hospital of Martinique had to reduce its bed capacity from 18 to 10 beds only and suspend all of its scheduled activities in the Operating Theater during the pandemic's five waves. Even during the pandemic's "calm" periods, we never had access to more than 40% of our normal operative capacity, excluding emergencies. Fortunately, our Hand Department had established a small Office Surgery setting in 2007 to address minor hand emergencies. Two years before the onset of the COVID-19 pandemic, we successfully opened a second setting dedicated to scheduled surgeries. Our staff was greatly inspired by the presentations and publications of Dr. Donald H. Lalonde from Saint John, Canada, a staunch advocate for Wide Awake and Office Surgery, and we sought to implement his valuable advice [3, 6, 8, 9, 10, 11, 12, 13, 14, 16].Our emergency activity was not significantly impacted by the COVID-19 pandemic; we still had access to a primary Operating Room for patients with severe hand and upper limb trauma, and we were already organized to treat minor hand traumas using Wide Awake and Office Surgery techniques [7, 13, 14, 15].
The transformation and adaptation of our scheduled surgical activity were necessary because, since March 2020, we had very limited resources, and sometimes none at all (during the waves of the COVID19 pandemic), to operate on our patients. This unique situation compelled us to suddenly adopt Dr. Lalonde's philosophy and to perform surgeries without our anesthesiologist colleagues and outside the "hyper-sterile" Operating Theatre [16]. Initially, we were apprehensive and hesitant, as we were entering uncharted territory. However, two years later, we have successfully transitioned small pathologies (carpal tunnel, trigger finger, De Quervain tenosynovitis, ganglion cysts, small tumors, pins removal) to Office Surgery, which now represents 62% of our whole Ambulatory Surgical activity.
In this article, we realized a monocentric retrospective study, comparing our ambulatory surgical activity for two years before and after the fateful date when the COVID-19 pandemic struck our territory.
Since 2007, our Hand Surgery Department had an isolated minor procedure room within its premises, dedicated to small trauma cases (emergencies only). At the beginning of 2018, we successfully opened a second room equipped with an air filter, dedicated to clean scheduled surgeries. In both locations, we employed field sterility principles: only masks, sterile gloves, and a small sterile wound drape with an area of 40 cm by 40 cm or less were used around a wound. We never used sterile gowns, full patient draping, head covers, or footwear for either the medical staff or the patients [7, 13, 14, 15].
We did not have an anesthesiologist; initially, we only performed local anesthesia. Since 2017, we introduced the WALANT technique for small procedures [16, 31]. Wide-awake Local Anesthesia No Tourniquet (WALANT) is a surgical technique that relies on local anesthetic and hemostatic agents to provide conditions suitable for hand surgery without sedation and tourniquet. The use of WALANT leads to decreased cost and enhanced patient safety [21, 24, 26, 32]. In our department we inject Xylocaine 10mg/ml § Adrenaline 0,005 mg/ml associated to Bicarbonate of Sodium 0,42g/10 ml in the proportion 10:1 (Figure 4.)

Figure 4: In our department we inject Xylocaine 10mg/ml § Adrenaline 0,005 mg/ml associated to Bicarbonate of Sodium 0,42g/10 ml in the proportion 10:1
Canadian plastic hand surgeon Dr. Lalonde first implemented WALANT to decrease wait times for surgery. He formally proposed the concept in 2005 and has since internationalized it [8, 9, 10, 11, 12, 13, 14, 15, 16]. We adopted entirely all the 10 pieces of advice recommended by Dr. Lalonde et al. in order to obtain a painless anesthesia:
Before the COVID-19 pandemic impacted our medical activity, our department had sufficient access to the main operating room (OR). Therefore, even though we had the capability, we chose to perform the majority of our scheduled procedures, including minor ones, in a real operating theater using loco-regional anesthesia. In March 2020, hospital rules changed dramatically. The majority of the Operating Rooms were closed, with a few remaining open for emergency pathology cases. Almost half of the hospital's bed capacity was dedicated to COVID-19 patients, forcing many departments to close or transform. Our Hand Surgery Department's capacity decreased from 18 to 10 beds, which was insufficient even for our trauma activity alone. Over the past two years (March 2020 – February 2022), we experienced five waves of the COVID-19 pandemic, during which we had no access at all to the Main OR for our scheduled patients. Between the waves, we were allocated less than 40% of the normal OR time. None of our surgeons was transferred in a COVID-19 Unit. Nationwide, 80% of the Orthopedic Departments have stopped completely the scheduled activity, when the COVID-19 Pandemic started [25]. The Orthopedic Department of the Universitary Hospital of Nice decreased its total surgical activity by 4 times (from 772 to 194 patients) [26]. In France, 40% of the Orthopedic Departments were transformed in COVID-19 Units. 28% of the Orthopedic surgeons were forced to abandon their specialty and to work in other medical Departments under tension. 41% of the Orthopedic surgeons adopted the tele-consultation. 54% of them presented at least one sign of psychologic symptoms. In India, 34% of the Orthopedic surgeons stopped operating and 10% of them worked in the COVID-19 Departments. In USA, 10% of the Orthopedic Seniors and 25% of the residents worked in the COVID-19 Units. [25, 23]. This challenging situation forced us to increase our Ambulatory activity due to the lack of bed capacity. Additionally, the limited access to the Main Operating Room prompted us to rapidly adopt Dr. Lalonde's philosophy and transfer a significant portion of the ambulatory scheduled pathology to the minor procedure room, which was not affected by the COVID-19 situation [11, 20].Our article compares, in a monocentric retrospective study, our ambulatory activity (the type that could be transferred to the minor procedure room) for two years before the COVID-19 pandemic (March 2018 – February 2020) with the two years during the COVID-19 pandemic (March 2020 – February 2022). We emphasize that our minor hand trauma surgery had already been performed using WALANT since 2017 and Office Surgery since 2007. We have to recognize that we offered few informations to our patients about the changes that we were obliged to adopt. We briefly announced, every one of them, that the Main Operation Room was closed and that we have to adapt our surgical activity due to COVID-19 pandemic. We didn’t ask them to sign any patient consent form and we didn’t present the disadvantages of the WALANT technique. Only 4 patients, being afraid that they would have more pain with WALANT procedure, refused the local anesthesia and delayed their surgery, in order to have a loco-regional or even a general anesthesia.
We observed significant differences between the two periods, explained solely by the reduced medical resources imposed by the COVID-19 pandemic. We didn’t exclude any patient treated in Office Surgery from our study, no matter the age, the sex, the pathology or the result, neither before, nor after the Pandemic. Our total scheduled ambulatory activity increased by 32% (855 patients in the first period, versus 1135 in the second one). Our scheduled surgical activity performed with WALANT § Office Surgery increased by 235% (from 299 to 705 patients).
Before the pandemic, we performed WALANT and Office Surgery only for pin removals (not all of them) - 299 patients in two years. After March 2020, we began to perform Office Surgery for other minor pathologies (carpal tunnel, trigger finger, De Quervain tenosynovitis, ganglion cysts, MCP and PIP teno-arthrolysis, small tumors, etc.) [17, 18, 19] and completely transferred pin removals outside the Main OR – 705 patients in two years (235.7% more than the previous period) (Figure 1)
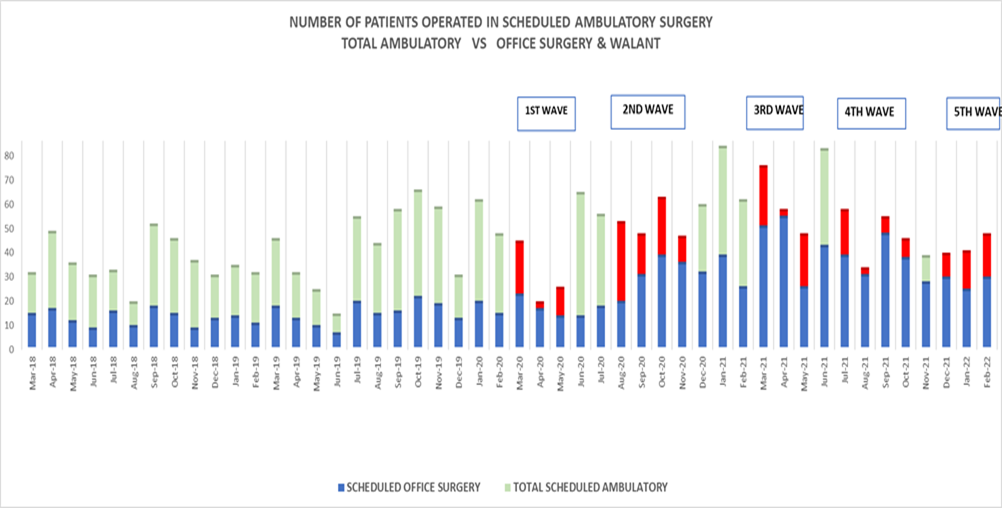
Figure 1: Number of patients operated in scheduled ambulatory surgery (in green) compared with the ones operated in Office Surgery with WALANT technique (in blue). We have colored in red the COVID 19 waves periods, when the access to the Main OR was restricted.
We even stopped treating distal radius fractures with pin fixation (almost 40% of them before the pandemic) and exclusively used plate fixation afterward, to avoid overburdening the Office Surgery with pin removal patients.
During the pre-COVID-19 period, only 35% of our ambulatory scheduled procedures were performed with WALANT in the minor procedure room. However, during the COVID-19 pandemic, we increased not only the ambulatory activity but also the proportion of WALANT procedures performed outside the Main OR, up to 62%.
Examining hand trauma treated in office Surgery with WALANT (Figure 2), we find that the COVID-19 pandemic did not significantly change the number of hand accidents. We managed 2097 minor hand trauma cases two years before the pandemic and 2005 patients during the two years of the pandemic. Notably, during 2020 and 2021, we treated more patients for minor hand trauma than in 2019.

Figure 2: Number of Hand Surgery Emergencies operated in Office Surgery with WALANT technique (in blue). We have colored in red the COVID 19 waves periods.

Figure 3: Evolution of the Hand Surgery 2 years before comparing to the 2 years of the COVID-19 PANDEMIC
Although the difference between the two periods seems substantial, we were cautious and reserved in expanding our WALANT indications. The first COVID-19 wave compelled us, due to the lack of access to the Main OR, to transfer our scheduled ambulatory patients to the Office Surgery Room. We also observed that patients themselves stopped seeking surgery, as the shock of the pandemic was so dramatic. After the first wave, our department reverted to old habits, performing small scheduled surgeries back in the Main OR. It was only during the second wave, which lasted almost four months, that we truly understood the need for a long-term safe, alternative, and independent solution for our scheduled ambulatory surgery. Consequently, we fully embraced WALANT as an Office Surgery technique. It took time to break old habits, and as Figure 1 shows, we completely adopted the WALANT technique only after the 4th wave. Although we recognized that the pandemic would persist and that only the WALANT technique combined with Office Surgery could provide a long-lasting safe solution, we chose to remain within a safe domain, performing only simple and relatively localized operations (pin removal, carpal tunnel, trigger finger, etc.), as described in Table 1
| Surgical Technique | No. of Patients |
| Pins Removal | 367 |
| Carpal Tunnel Release | 144 |
| Trigger Finger Release (1 or more) | 108 |
| Carpal Tunnel Release + Trigger Finger Release | 24 |
| De Quervain Stenosis Tenosynovitis Release | 23 |
| Ganglion Cyst of the Wrist/Hand Resection | 17 |
| Dorsal MCP & PIP Arthrolysis | 11 |
| Benign Tumors of the Hand Resection | 11 |
| TOTAL | 705 |
Table 1: The pathology and the number of patients operated using WALANT & Office Surgery, during the 2 years of COVID 19 Pandemic
The impressive number of pin removals (52% of the ambulatory scheduled patients treated in Office Surgery) is due to our department being the primary Hand Surgery Center of the French Western Indies Territories and that nearly 70% of our patients are emergency cases (hand and upper limb trauma).
Examining hand trauma treated in Office Surgery with WALANT (Figure 2), we find that the COVID-19 pandemic did not significantly change the number of hand accidents. We managed 2097 minor hand trauma cases two years before the pandemic and 2005 patients during the two years of the pandemic. Notably, during 2020 and 2021, we treated more patients for minor hand trauma than in 2019.
Our results were different than those of other Hand Departments on the Continental France. Nationwide, the Hand Departments decreased their Trauma activity by 35% in the COVID-19 areas and by 25% in the non-COVID-19 areas. Despite this fact, the complex wounds and the open fractures increased during the COVID-19 pandemic [27, 28, 29, 30]. We attribute this phenomenon to the fact that people in confinement engaged in more gardening and small construction renovations, which exposed them to more accidents than their regular work. Martinique has very few industries with high accident exposure. The island's main activity, agriculture, was not interrupted by the pandemic.
Thus, even though we were cautious with our Office Surgery indications, we have gained experience and confidence in WALANT techniques two years later. We are now prepared to transfer other operations to the minor procedure room: cubital tunnel release, lacertus syndrome release, palmar tenolysis or arthrolysis, and even Dupuytren fasciectomy [2, 3]. We are also beginning to shift more emergency cases to the Wide-Awake domain: digital nerve and flexor tendon sutures, pyogenic tenosynovitis, phalanx percutaneous pin fixation [8, 9, 10, 11, 12, 31].
We observed that Wide-Awake surgery does not have more complications than classic surgery, despite the less sterile conditions present in the minor procedure room. In carpal tunnel release cases, we had only three superficial infections in 144 cases (2%), which is comparable with the international literature, reporting an infection rate of 0.39 – 1,34% [4, 17, 19, 21, 31]. No additional surgery was needed for the superficial infections; only suture removal, oral antibiotics, and close monitoring were required, without significant harm to the patient.
Our department typically places pins under the skin in hand trauma cases. Sometimes, the hand volume decreases after a few weeks, and a pin becomes prominent or migrates and pierces the skin. We systematically remove such pins in emergency, but this superficial infection is not a complication of the WALANT technique; instead, WALANT resolves the septic complication.
We have not experienced other septic complications in other pathologies. Finally, surgical site infection rates in Wide Awake surgeries are similar for the same procedures when performed in the Operating Room [4, 17, 19]. Moscato and al., in a recent article from RCTO proved an increased satisfaction of the patient, for the carpal tunnel release, in the case of the WALANT associated with Office Surgery, comparing with the WALANT in the Main OR, which offers also more satisfaction comparing with the loco-regional anesthesia in the Main OR [31]. It explains the success of the WALANT associated with Office Surgery in the Hand Surgery Departments, all over the world, years before the COVID-19 pandemic, but even more because of the pandemic.
We fully understand that the advantages offered by the WALANT technique are significant and numerous:
The Wide-Awake techniques combined with Office Surgery can be considered, for the Hand Surgery, a safe, economical, ecological, and comfortable solution, preferred not only by the surgeons, but also by the patients [31]. Each surgeon has their own motivations for adopting the WALANT procedure. Our surgical team, even though it was already convinced of the efficacy of Wide Awake, needed a significant medical crisis (the COVID-19 pandemic) as a catalyst to implement it in practice. Today, after two years of experience and over 700 minor scheduled surgical operations performed with WALANT, we have enough confidence to expand Wide Awake to other surgical indications and more complex procedures, including those involving the forearm and elbow. The entire surgical team wishes to express its gratitude to Dr. Donald H. LALONDE, the true pioneer of the Wide-Awake technique, which is now adopted on an international scale.
Informed consent and patient details
The authors declare that the work described does not involve patients or volunteers.
The authors declare that they have no known competing financial or personal relationships that could be viewed as influencing the work reported in this paper.
Funding
This work did not receive any grants from funding agencies in the public, commercial, or not-for-profit sectors.
Author contributions
All authors attest that they meet the current International Committee of Medical Journal Editors (ICMJE) criteria for authorship.
Conceptualization, S.L.; Methodology, S.L.; Validation, S.L. and M.M.; Formal analysis, S.L.; Investigation, S.L. and M.M.; Resources, S.L.; Data curation, S.L.; Writing—original draft preparation, S.L.; Writing—review and editing, S.L.; Visualization, M.M.; Supervision, S.L.; Project administration, S.L.;
All authors have read and agreed to the published version of the manuscript.”
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
