
Review Article | DOI: https://doi.org/10.31579/2692-9406/127
*Corresponding Author: Ashok Chakrborty, Allexcel. Inc. Shelton, CT, USA.
Citation: Ashok Chakraborty, and Anil Diwan Allexcel. In. Shelton, CT. (2022). How and Why Macrophages are Connected with the Parkinson’s Disease: A Short Review to Develop a Therapeutic Strategy for PD. J. Biomedical Research and Clinical Reviews. 7(2); DOI:10.31579/2692-9406/127
Copyright: © 2022 Ashok Chakrborty, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 27 July 2022 | Accepted: 12 August 2022 | Published: 16 August 2022
Keywords: macrophages;parkinson’s disease; neurons; inflammation; polarization
Chronic neuro-inflammation cause the neural cell death including dopaminergic cells and ultimate results Parkinson’s disease (PD). In an MPTP-induced PD animal model an increased peripheral pro-inflammatory M1 macrophages (M1- MFs) were found. Polarization of this M1-type of MFs to anti-inflammatory M2-type revealed a potential therapeutic benefit for PD patients. Here we highlight the concept of MFs re-education as a method of PD therapies, and how we can deploy our knowledge to find out therapeutic regimen for PD treatment.
Parkinson's disease (PD) is a 2nd most prevailing progressive neurodegenerative disorder in the world, characterized by death of dopaminergic (DA-ergic) neurons in the substantia nigra pars compacta (SNpc) [1]. Though it is primarily considered as an age-related staring from 50 onwards, the onset has also been found at the very early age of life. Symptomatically it is well recognized by slow movement of the muscle, soft voices, posture problems and ultimately loss of memories. Deaths have also been recorded from this disease. Among all the mechanisms and factors so far involved for PD generation, like aging, genetic as well as environmental factors, including toxin, brain injury are recorded [2].
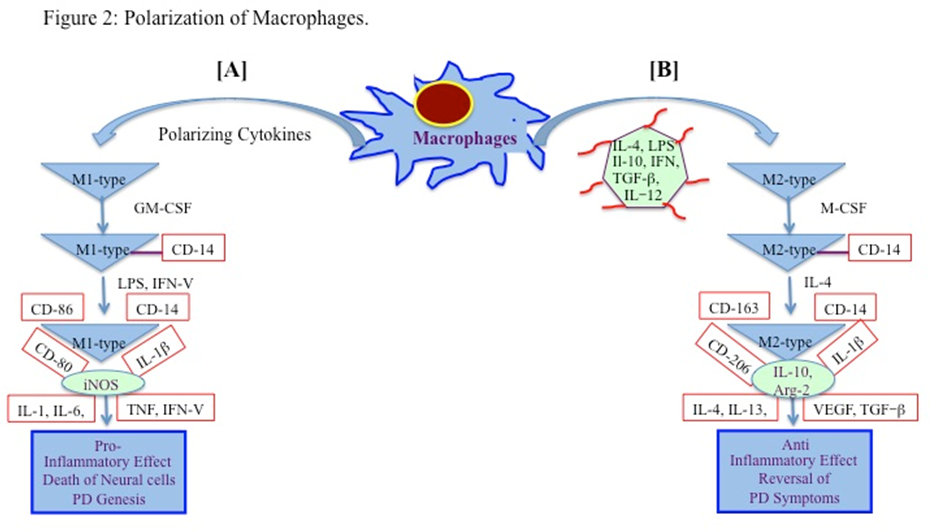
Chronic inflammation is universally thought to play a central role in the initiation and progression of PD [3, 4]. MFs are the main regulatory immune cells in the periphery [5]. One of the important features of MFs is their ability to polarize in its different forms (M1-or M2- MFs and adopt a variety of different activities in response to their environmental factors. M1 type of MFs is pro-inflammatory, and releases inflammatory factors and chemokines, such as interleukin-1β (IL-1β), tumor necrosis factor-α (TNF-α), and monocyte chemotactic protein-1 (MCP-1), and iNOS, etc. [6, 7]. In contrast, M2- MFs can produce anti-inflammatory cytokines including IL-10, IL-4, IL-13, and promote tissue damage repair [8, 9].
Differential abundances of M1- and M2- MFs have also been found to be associated with different disease phenotypes, including lung disease, diabetes, obesity, cancer, and atherosclerosis, etc. [10, 11]. As the inflammatory diseases progress, M1- MFs are gradually replace the M2-type [12]. It would be logical to investigate whether and how the MFs in the brain are polarizes to M1-type during the pathogenesis of PD, and further whether this phenomenon happened to all PD victims irrespective of their causative factors, including gene-defect.
As a part of innate immunity, MFs and neutrophils are known to cross the leaky blood brain barrier, and secrete cytokines (e.g., interleukins, tumor necrosis factor, interferon-g), which can initiate the inflammatory responses causing to PD development [13].
MFs
1.1: The Role of Peripheral Macrophages in the Pathogenesis of PD:
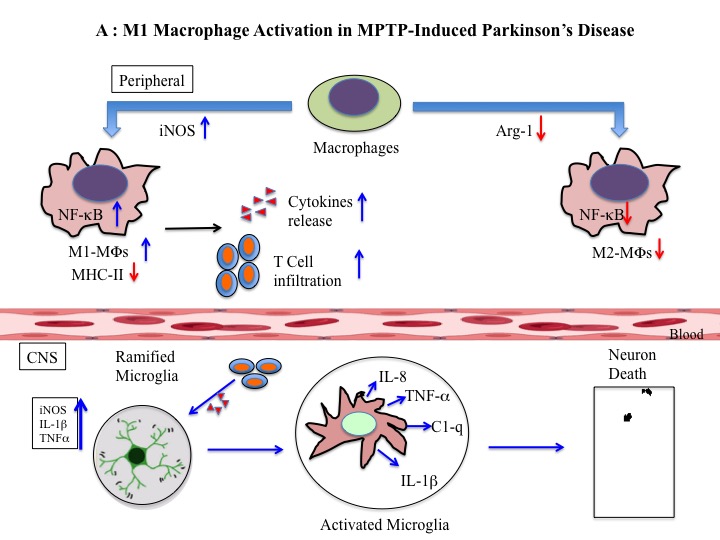
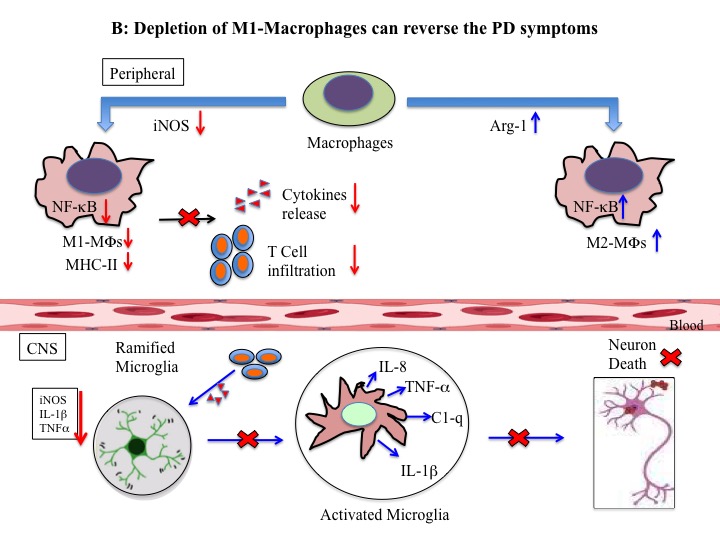
In an MPTP (1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine)-induced PD animal model, counts of M1-MFs are found at higher level. Clodronate liposomes treatment on them depletes M1-MFs level and increase its M2 type along with the reduction of neuro-inflammation and dopaminergic neuro-degeneration [14]. Parkinson’s disease symptoms can be controlled by intra-peritoneal injection of a stress reducer, clodronate liposomes which depletes the level of M1-MFs and increase its M2-type [15-17]. Some researchers have reported that treatments with clodronate liposomes preferentially induce apoptosis of M1 monocytes/macrophages and protected against MPTP-induced neuronal death in the SNpc [18, 19]. The ratio of M1 phenotype (CD11b+ MHC IIhi) to the alternatively activated M2 phenotype (CD11b+ MHC IIlow) decreased after clodronate liposome treatment [14].
1.2: The Decrease in M1-MFs Inhibits Activation of NF-κB Signaling Pathway and Expression of MHC II:
M1- MFs can be activated by pro-inflammatory stimulants via induction of NF-κB signaling pathway [18-20]. In one study it was found that MPTP when induced the PD development in mouse model, they also increased the phosphorylation of NF-κB and the expression of MHC II. [14]. Clodronate liposomes injection, however, was shown to reduce the MPTP- induced NF-κB phosphorylation and MHC II expression, as well as the PD symptoms. Therefore, the notion of macrophage polarization from M1-type to M2-type may be the plausible factor for slowing the progression of PD symptoms [3, 21, 22].
Niacin, a vitamin, was shown to play a role via its receptor, hydroxycarboxylic acid receptor 2 (HCAR2), in inducing the anti-inflammatory responses in animal model as well as in humans [23]. In fact, it is suggested that the niacin effects may be mediated via its receptor HCAR2, which is highly expressed in macrophages [24-26]. At the molecular level it was shown that the activation of niacin receptor HCAR2, down-regulates the NF-κB signaling pathway, antioxidant mechanisms, and does the induction of mitochondrial NAD, which may re-educate M1-MFs to M2-type and results the neuro-protective effects in PD patients [3].
1.3: Inflammatory Cytokine Expression and Microglial Activation were Inhibited After M1 Macrophage Depletion in the Striatum and SNPc:
T cells infiltration into the SNPc of PD victims have been documented earlier [27]. They release inflammatory cytokines to further activate microglia [28], and the activated microglia further can re-stimulate the T cells [29]. Assessment of the effect of M1 macrophages on inflammatory cytokine expression revealed that a prominent increase in M1- MFs result the release of the inflammatory cytokines IL-1β, IL-6, and TNF-a in the striatum and SNpc. Further, the polarization of M1 to M2-type macrophages decreased the cytokine expression, microglial activation and reverses the PD symptoms in mouse model [14].
From the above information it revealed a relationship between macrophage polarization and neuronal damage in PD (Figure 1A, 1B).
From this standpoint, a strategic development for PD therapy may be possible by adopting any of the following two methods. One, injection of polymeric NPs loaded with M1- MFs repolarizing cytokines in the brain
They will re-educate the pro-inflammatory PD-causing M1- MFs to its anti-inflammatory M2-Type and ultimately help the PD patients to get rid of their disease symptoms (Figure. 2).
Secondly, macrophage repolarization to its M2-type can be done in cell culture dishes in presence of reprogramming cytokines. Then these reprogrammed cells either can be transplanted in the brain area directly or, can be co-cultured with NSCs to get an unique reprogrammed cells (For review, 30-32) which should express anti-inflammatory cytokines, as well as can produce dopamine, a main element for PD therapy (Figure. 3).

From the above research it is revealed that the number of M1 macrophages in the peripheral immune system when increased, PD symptoms appear, and depletion of M1 macrophages can reverse the inflammatory effects as well as prevents neuro-degeneration. During PD pathogenesis over-activated immune cells infiltrate towards the SN region of the brain, and produce neurotoxic pro-inflammatory cytokines. The similar phenomenon was also observed during MPTP-induced PD genesis in mouse model [1, 33, 34]. Recent research showed that inflammatory M1- MFs in peripheral immune system when repolarized to anti-inflammatory M2-type by clodronate liposome or niacin that can rescue from neurological deficits and neuron reduction in the SNpc [35, 36].
M1- MFs release more pro-inflammatory cytokines by activating the NF-κB signaling pathway [37], and have greater antigen-presenting capacity through the expression of MHC-II class of antigen [38]. All these effects in turn could activate T cells to infiltrate into the brain [37, 39], which ultimately activate the microglia. The activation of microglia produces inflammatory cytokines, which are detrimental to the neural cells [9]. However, depletion of M1- MFs by repolarizing it to M2-type reduces the phosphorylation of NF-κB and the expression of MHC II antigen, ultimately can restore the neural health. In conclusion, the neural cell death in PD can be restored by any factors like cytokines, vitamins, nanoparticles, which can polarize pro-inflammatory M1-type of macrophages to its anti-inflammatory M2-type.
Accumulation of M1 type of macrophages in the brain is the key player of PD onset, may there be any reason for that including genetic and/or sporadic factors. Repolarization to its M2-type is the strategy that could be deployed by cytokines, nanoparticles or both. NSCs also can be the vehicles of those cytokines and can be packed in polymeric nanoparticles for uninterrupted and safest delivery to CNS area. The DA-ergic NSC cells while will replenish the loss of neural cells the anti-inflammatory cytokines will re-educate M1 type to M2 type, and in combination therapeutic benefits could be achieved for PD victims.
We acknowledge all our colleagues for their help during the preparation of the manuscript by providing all the relevant information. We are also thankful to Ms. Bethany Pond (Analytical Chemist at AllExcel, Inc.) for editing the manuscript.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Both the authors have agreed to submit this paper for publication.
Ethical Approval
Not applicable
Conflict of Interest Statement
The authors declare no conflict of interests.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
