
Research Article | DOI: https://doi.org/10.31579/2641-0419/205
1Programa de Pós-Graduação em Ciências da Saúde, Universidade Federal de Sergipe, Aracaju, Sergipe, Brasil.
2Núcleo de Pós-graduação em Enfermagem da Universidade Federal de Sergipe,1 Aracaju, SE – Brasil
3Departamento de Medicina, Universidade Federal de Sergipe, Aracaju, Sergipe, Brasil.
4Departamento de Nutrição da Universidade Tiradentes,7 Aracaju, SE – Brasil
5Programa de Pós-Graduação em Biometria e Estatística Aplicada, Universidade Federal Rural de Pernambuco, Recife, Pernambuco, Brasil.
6Departamento de Fármacia da Universidade Tiradentes, 7 Aracaju, SE – Brasil
7Clínica e Hospital São Lucas, Rede D'or, Aracaju, Sergipe, Brasil.
8Setor de Cardiologia, Hospital Universitário, Universidade Federal de Sergipe, Aracaju, Sergipe, Brasil.
*Corresponding Author: Jussiely Cunha Oliveira, Universidade Federal de Sergipe - Cidade Univ. Prof. José Aloísio de Campos Av. Marechal Rondon, s/n. CEP 49100-000, Jd. Rosa Elze, São Cristóvão, SE – Brasil.
Citation: Jussiely C. Oliveira , de Jesus NC., Jeferson C. Oliveira., Munareto Lima TCR., Carvalho Barreto IDD., et al. (2021) Hospital Pharmacological Treatment of Acute Myocardial Infarction with st Supra: Sus x Private.. J. Clinical Cardiology and Cardiovascular Interventions, 4(16); DOI:10.31579/2641-0419/205
Copyright: © 2021 Jussiely Cunha Oliveira, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 28 July 2021 | Accepted: 24 August 2021 | Published: 30 August 2021
Keywords: cardiovascular diseases; myocardial infarction; clinical protocols therapeutics
Objectives: To compare the adequacy of drug therapy in STEMI in public and private hospitals.
Methods: Prospective analysis of 471 patients admitted with STEMI in public and private hospitals in the state of Sergipe.
Results: Clopidogrel usage fee (91% vs 36% ; p < 0.001 ) and ACE inhibitors (66% vs 22 %; p < 0.001 ) was higher among SUS patients, however, use of ticagrelor (61% vs 1% ; p < 0.001 ) and BRA II (24% vs 9 %, p = 0.002 ) was higher among those treated in the private sector. In the pooled analysis, SUS patients received more IECA and/or BRA II than those with indication an absolute for its use (76% vs 30%; p < 0.001).
Conclusions: A significant difference was observed in the use of ACE inhibitors and/or ARBs among patients in both groups, a higher rate of use of these drugs was showed amongst SUS patients.
Due to the incidence of Coronary Arterial Death (CAD), it is high in the whole world, and not Brazil, it is the second main cause of death in Brazil and you have indicated that 97 thousand deaths, due to ischemic heart disease, in a year, responsible for 210,046 hospital admissions in Brazil and 29% two deaths (99,408 deaths or 55.11 deaths / 100 thousand inhabitants [9] corresponding to 19% of total custody with hospital internment, a sum of R $ 1.9 bilhão [1].
The taxa of morbidity and mortality due to acute myocardial infarction (AMI), not Brazil, are related to the difficulty of not accessing specialized services and lack of attendance and delay in not attending primary care and the elderly is associated with death, in both sexes, besides, older Death taxa, sejam identified in homens [2].
In addition to high mortality from heart attack, analyze two registries of the Swedish Web System for the Development and Development of Care Based on Evidências em Doenças Cardíacas endorsed by agreement with the Registry of Recommended Therapies (SWEDEHEART) will indicate which treatments based on events, as interventions Primary percutaneous coronary arteries (PCI), reperfusion therapies, aspirin, P2Y12 inhibition, beta-blocker, angiotensin-converting enzyme inhibitor / angiotensin receptor blocker and statins will collaborate with our results of total and cardiovascular survival [3].
No country is the most populous in the world, a study on AMI management, identified that more than 90% of these patients were treated with aspirin, clopidogrel and statin, with approximately two patients receiving β-blockers and / or ACEI / ARB4, but not after discharge, patients who survive, with type I myocardial infarction, derived from acute coronary syndrome, use more aspirin, statin and antiplatelet therapy. [5]
Other important discussions on treatment and therapeutic regimen, address cardiovascular safety of long-term treatment with oral anticoagulant, in this context, a meta-analysis, evidence that anticoagulant escorts, also expose anticoagulated patients to a higher risk of myocardial infarction, and risk of myocardial infarction, and risk of myocardial infarction. , I study or compare some anticoagulants, or risk of heart attack was minor with rivaroxabana6, direct inhibitor of the factor of coagulation Xa.
In addition, we have seen intense efforts in recent years to save on heart attack treatment both during acute hospitalization and secondary prevention in outpatient care. Therefore, despite two significant benefits of pharmacological measures, it is not known that these drugs are prescribed adequately for patients. Therefore, this study aims to compare the adequacy of pharmacological treatment in IAMCSST in public and private hospitals in the state of Sergipe according to the Guideline of ACCF / AHA7 for treatment of IAMCCST.
It deals with a coorte study with a quantitative approach carried out in two hospitals of the public network and three private hospitals of the state of Sergipe with access to angioplasty outside the state of Sergipe, all located in the capital of Aracaju, no period of outubro from 2013 to April 2015. Foram included patients older than 18 years, with STEMI evidenced by electrocardiogram according to the defining criteria of the Guideline of ACCF / AHA7 and that assinaram or TCLE. Foram including patients admitted to two hospitals of the public health network.
It was shown to be composted by 471 patients, since 387 foram cared for in a public health network and 84 in a private network. The data collected by a research group called VICTIM (Via Crucis para o Tratamento do Infrto do Miocardio) composed by doctors, nurses, medicine and pharmacy students and patients will respond to a questionnaire on demographic data, prodromal symptoms and presentation, gatilhos for infarction, premature pathological history, cardiovascular risk factors and previous pharmacotherapy. The clinical data for the collection of hair records two records with information on physical examination of admission, complementary tests, pharmacotherapy used 24 hours and the last prescription before discharge from hospital, plus two hospital injuries.
This investigation was submitted to the Ethics and Research Committee of the Federal University of Sergipe UFS and approved under the number 2,099,430. All population studied assinou or TCLE, agreeing to participate in the investigation. In cases where the patients are not able to assassinate or thermo, or responsible or fez. Illiterates will be authorized through digital printing, followed by the assumption of two tests.
Foram included 403 (86.62%) patients admitted to non-public service and 68 (14.44%) non-private, totaling 471 patients with acute myocardial infarction with ST-segment elevation (STEMI). The patients who are users of the public network, were maioria homens (65%), with lower social class (at least 2 salaries 60%), lower grade of schooling (ensino fundamental 49%) and who declared themselves to be of non-white ethnicity (62% ).
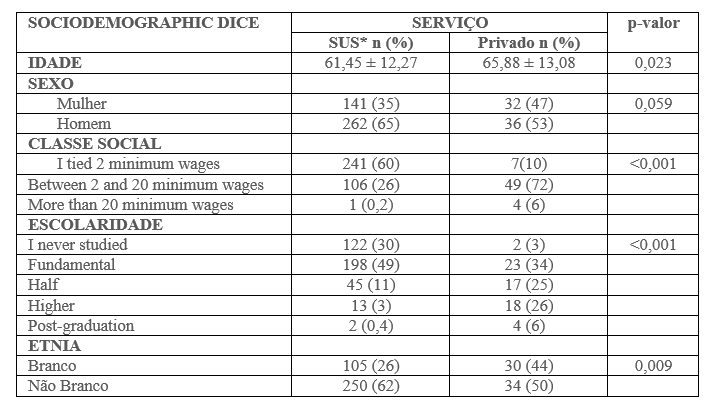

Table 2 illustrates the use of medications for the first 24 hours of hospitalization. In a comparison between the patients seen not in the SUS and in the private service, the first ones used Clopidogrel more frequently (91% vs 36%; p <0 xss=removed>
When the use of beta-blockers is validated in patients who are not contraindicated (Table 3), there is no statistically significant difference between patients in the public service and in the private service. For this analysis, we excluded patients who presented a heart rate without a physical examination of admission below 60 beats per minute, systolic arterial pressure below 100 millimeters of mercury, or Killip> 1.
When using the platelet antiaggregation pair for the first 24 hours of hospitalization (Table 3), expressive taxa of patients who used aspirin (ASA) associated with a platelet antiplatelet is evidenced. Chama atenção also ao fate of 6% of both the groups (SUS and private) não terem feito use of AAS.

Já or use of ACE inhibitors and / or ARBs at the first 24 hours of hospitalization, in patients with previous AMI, ST segment supra-leveling in V3 / V4 evidenced by no ECG, and / or Killip> 1, observed higher taxa of use we attended SUS hair when compared with patients seen in private hospitals (76% vs 30%; p <0>
Our prospective and observational study of the drug treatment prescribed for the first 24 hours, compared between the public and private hospitals with the capacity to perform primary angioplasty in Sergipe, using data from the VICTIM registry, verified that there was a significant difference in any way. that the patients seen in a private hospital were presented with a mais avançada (65.88 ± 13.08 vs 61.45 ± 12.27; p = 0.023).
When comparing the use of drugs in the first 24 hours of care of two patients in the study, it was verified that there was a statistically significant difference in the prescription of antiplatelet drugs. The public service patients had more use of Clopidogrel (91% vs 36%; p <0>
Since I studied CLARITY - Clopidogrel as Adjunctive Reperfusion Therapy (n = 3,491), published in 2005, which validates the importance of associating another antiplatelet antiaggregant to or ASA in patients with STEMI8, or Clopidogrel was or antiaggregant more used, or that it corroborates Given that we are studying when raised in consideration of the patients of the public service. Furthermore, the use of ASA and Clopidogrel was higher in our study than the 87.2% cited by Bahall et al10, when evaluating or in-hospital treatment of patients with AMI in a country with limited resources
In our study, when the first 24 hours antiaggregation treatment was validated or used, associating the use of ASA with any other antiplatelet agent, it was not demonstrated statistically significant difference between the patients attended not in comparison with the private sector. In both groups, there was no record of ASA prescription for the first 24 hours of hospitalization for 6% of two patients.
Some limitations of the study will end up hampering the analysis of the given. It should be mentioned that there was no question or a research instrument regarding allergy to a drug or other contraindications to its use. Furthermore, patients may have received a recommended initial dose of 200 mg of ASA in the pre-hospital phase, and therefore no record of ASA in the intra-hospital prescription within the first 24 hours or given may have been underestimated.
When I was comparing or general use of two other medications, it was also shown that patients give the public health network in Fez plus use of ACE inhibitors for the first 24 hours (66% vs 22%, p <0 xss=removed>
The ACCF / AHA7 guideline also recommends the use of an ACEI / ARB in all patients with STEMI with contraindications for its use, as a recommendation grade IIa and level of evidence A. Also, it is presented as recommendation grade I, level of Evidência A or use of ACEI / ARB in the first 24 hours for all patients with STEMI in the anterior wall, heart failure or failure of execution less than 40%, is not contraindicated. In this way, an analysis was performed as patients who presented anterior AMI hair ECG (ST segment supra-leveling in V3 / V4), or presented Killip> 1 no physical examination of admission. It was not used or criteria for EF <40>
It was also observed that the use of beta-blockers in the first 24 hours in patients with contraindications for such. Studies and guidelines [7,9] indicate that oral beta-blocker should be started in the first 24 hours in patients with STEMI who do not present two following criteria: no heart failure, evidence of low-output state, increased risk for cardiogenic shock, or other Contraindication for its use (PR interval greater than 0.24 seconds, cardiac block of second or third grau, active asthma or effective dose of airways). There are limitations to the evaluation of all the contraindications to the use of beta-blockers that are not an instrument of the research group. Therefore, we selected the patients whose physical examination gives admission to present HR> 60, BP> 100 and Killip = 1. Furthermore, there is no statistically significant difference from this analysis.
When it comes to intra-hospital pharmacological treatment of STEMI, the public health network appears to be a better tax on the use of ACEI / ARB in relation to the private sector, drug classes that are important in the acute phase of this condition. However, both present a reduced taxa for the use of some medications as an indication of use for the first 24 hours post-AMI second or more recent guideline from ACCF / AHA, published in 2013, showing that there is space for no in-hospital pharmacological treatment. do IAMCSST not state of Sergipe.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
