
Case report | DOI: https://doi.org/10.31579/2578-8868/341
Department of Neurosurgery Tokyo Metropolitan Tama Medical Center 2-8-29 Musashidai, Fuchu, Tokyo 183-8524, Japan.
*Corresponding Author: Nobuhiko Aoki, Department of Neurosurgery, Bethlehem Garden Hospital 3-14-72 Umesono, Kiyose, Tokyo 204-0024, Japan.
Citation: Nobuhiko Aoki, (2024), Holohemispheric Hemorhhage in Infantile Acute Subdural Hematoma: Serial Neuroimaging Analysis, J. Neuroscience and Neurological Surgery, 16(3); DOI:10.31579/2578-8868/341
Copyright: ©, 2024, Nobuhiko Aoki. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 07 October 2024 | Accepted: 18 October 2024 | Published: 31 October 2024
Keywords: infantile acute subdural hematoma; shaken baby syndrome; abusive head trauma; benign enlargement of the subarachnoid space; large sylvian fissure; dural border cell layer; holohemispheric subdural hematoma
Background: An acute subdural hematoma (ASDH) in infants without any external sign of trauma is differently recognized as shaken baby syndrome (SBS) / abusive head trauma (AHT) in the United States or as infantile acute subdural hematoma (IASDH) due to minor head trauma in Japan. The present case report aimed to demonstrate that IASDH can occur after a mild head impact if the dural border cell layer is disrupted in an infant with cranio-cerebral disproportion (CCD).
Case description: A 5-month-old, male patient fell from a baby bed and struck his occiput against a mat. He began to cry and soon thereafter demonstrated signs of altered consciousness. He was taken to a pediatric hospital where computed tomography (CT) revealed a thin subdural hematoma (SDH) surrounding the entire right cerebral hemisphere. Fundoscopy found a right-sided retinal hemorrhage. Magnetic resonance imaging (MRI) on hospital day 4 revealed a thin, high-intensity ASDH surrounding the entire, cerebral convexity on the right side. In addition, benign enlargement of the subarachnoid space (BESS) and large sylvian fissure (LSF) were noted. On hospital day 12 and 18, follow-up MRI revealed a residual SDH with minimal reduction. The patient had an uneventful clinical course and met all the normal, developmental milestones as of his current age of 3 years.
Conclusion: The present case is invaluable because it demonstrates that ASDH can occur as a result of a mild, occipital impact. Particularly relevant here is the thin, holohemispheric appearance of the hematoma on neuroimaging studies, which has been suitably termed, holohemispheric subdural hematoma (HHSDH).
Also noteworthy is the long-term presence of the HHSDH with minimal reduction of the SDH. The HHSDH may be caused by entrapment of the hematoma in the dural border cell layer in the absence of any communication with the surrounding structures.
An acute subdural hematoma (ASDH) accompanied by retinal hemorrhage (RH) is often diagnosed without question worldwide as shaken baby syndrome (SBS) / abusive head trauma (AHT). [1] However, this tendency is based exclusively on the assumption that a short fall is unable to cause ASDH [2]. Because infantile ASDH (IASDH) cases have been reported to date mostly in Japan [3] and rarely occur outside the home, the accidents resulting in the trauma are seldom witnessed by a third party.
The present case report aimed to demonstrate that IASDH can occur if the dural border cell layer (DBCL) is disrupted in an infant with cranio-cerebral disproportion (CCD). The newly proposed term, holohemispheric subdural hematoma (HHSDH), is indispensable for describing such cases [4, 5]. The present report includes a description of the serial neuroimaging characteristics of HHSDH.
A 5-month-old, male patient fell from a baby bed and struck his occiput against a mat. His mother noticed that the infant began crying and soon thereafter showed signs of altered consciousness. He was taken to a pediatric hospital where he seemed alert and his baseline activity was normal. Although no neurological abnormalities or external signs of trauma were observed, CT revealed a thin subdural hematoma (SDH) surrounding the entire, right cerebral hemisphere (Figure. 1). Fundoscopy on the same day found unilateral, multiple multilayered retinal hemorrhages on the right side. The patient was hospitalized for further clinical observation.
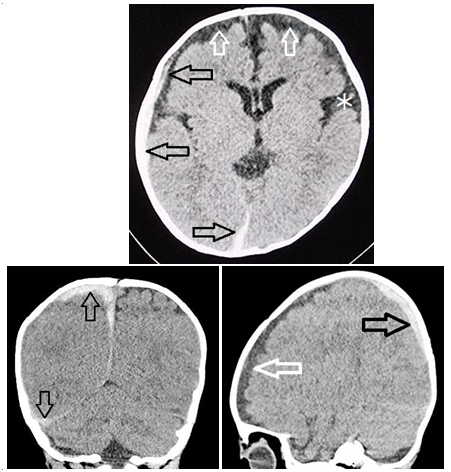
Upper : axial view. Middle : coronal view. Lower : sagittal view
Thin subdural hematoma (SDH) surrounding the entire cerebral hemisphere on the right side. (black arrows)
Benign enlargement of the subarachnoid space (white arrows)
Large sylvian fissure on the left side (asterisk)
Figure 1: Computed tomography on arrival
Magnetic resonance imaging (MRI) on hospital day 4 revealed a thin, high-intensity ASDH surrounding the entire right cerebral convexity. In addition, benign enlargement of the subarachnoid space (BESS) and large sylvian fissure (LSF) were noted. (Figure. 2 upper) On hospital days 12 and 18, follow-up MRI revealed minimal reduction of the ASDH (Figure. 2 middle & lower). The patient had an uneventful clinical course and has met all the normal, developmental milestones as of his current age of 3 years.
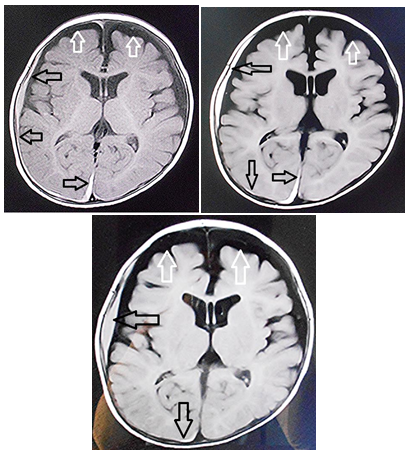
Upper : Day 4. Middle : Day 12. Lower : Day 18 after occipital impact
Subdural hematoma (SDH) (black arrows) surrounding the entire cerebral hemisphere (i.e, the holohemispheric SDH).
Large subarachnoid space (white arrows) indicating benign enlargement of subarachnoid space.
Note the minimal reduction of SDH (black arrows) between days 4, 12, and 18.
Figure 2: Magnetic resonance imaging (fluid-attenuated inversion recovery)
Based on the biophysiological characteristics of infants, IASDH was originally defined in 1984 as an acute, infantile subdural hematoma apparently caused by minor head trauma without loss of consciousness and not associated with a primary brain injury [3]. IASDH has been reported in Japan since the 1960’s [6]. However, because most cases were published in Japanese-language journals and accusations that the diagnosis was an attempt to conceal child abuse were frequently raised, the concept of IASDH has not been widely accepted in the English-speaking world. Indeed, a previous case study of 24 IASDH cases published in 1984 was critically reviewed in a Letter to the Editor as follows: “While not totally pathognomonic of shaking, the constellation of subdural hematoma and retinal hemorrhage in the context of a historically trivial injury should be regarded as whiplash shaken baby syndrome unless another etiology can be determined” [2]. However, recent Japanese reports have demonstrated that patients with IASDH can be distinguished from those with SBS/AHT through multidisciplinary assessment, including an evaluation by child abuse pediatricians and pediatric neurosurgeons [6 -11]. Moreover, neuroimaging studies can rule out a cerebral parenchymal injury, including cerebral contusion and diffuse axonalinjury (DAI), when diagnosing IASDH.
Table 1 lists the differing features of IASDH and SBS/AHT.
Table 1: Comparison of infantile acute subdural hematoma (IASDH) and shaken baby syndrome (SBS) /abusive head trauma (AHT)
| IASDH | SBS/AHT | |
| Applied force | Minor head trauma | Abuse (high energyimpact) |
| Main etiology | Disruption of bridging vein | Cerebral contusional tears |
| Primary brain injury | None | Common |
| Age distribution | Peak in 6 ~ 10 months | Widely distributed (Including less than 3months) |
| Sex | Marked preponderance in male | No preponderance |
| Recurrence | Rare | Not rare |
| Prognosis | Depending on volumeof hematoma (mostly, benign clinical courses) | Poor |
| Retinal hemorrhage | Frequent | Common |
(Cited from Ref. 6 with permission of the Japanese Society of Pediatric Neurosurgery)
There are three, distinct differences between these conditions. First, IASDH generally has a benign clinical course, with approximately 80% of the patients recovering well [ 3, 6, 11-15].
Second, IASDH is strictly age-specific and occurs mostly in male infants between the ages of 6 and 12 months. As a result, accidents occurring outside the home are extremely rare and seldom witnessed by a third party.
Recently in the United States, ASDH was diagnosed in eight patients younger than 24 months who were witnessed by family members suffering a short fall that resulted in an occipital impact [16]. Together with their favorable outcome, clinical features in their series are coincide with IASDH in Japan. Even in cases with fulminant-type (most severe form of IASDH) can be followed by good recovery after emergency surgery because of absence of cerebral parenchymal injury. [3,11]
The third, most important, distinctive difference of IASDH from SBS/AHT is the absence of encephalopathy (i.e., a primary cerebral parenchymal injury, which is a fundamental element in the triad of SBS symptoms and signs.
These pathological features of IASDH, including the fulminant type, as confirmed by imaging studies and surgery, are compatible with the mostly benign clinical course following conservative management or rapid surgical intervention. [3,11] Thus, it is highlighted that favorable outcome in IASDH patients is derived from the absence of a primary cerebral parenchymal injury. To the best of my knowledge, however, there are no reports in the English-language literature focusing on the presence or absence of a primary cerebral parenchymal injury indicative of the fundamental pathology of SBS.
The dural border cell layer (DBCL), a distinct, soft-tissue layer at the dura-arachnoid interface, is composed of a loose conglomeration of cells having enlarged, extracellular spaces and no extracellular collagen [17]. ASDH occurring in this environment results from the disruption of the DBCL by pooled blood. Furthermore, in the superficial compartment of the DBCL, there is a well-developed dural venous plexus which fills the venous sinuses. Because the DBCL is easily disrupted, a hemorrhage originating in the inner dural plexus may be chiefly responsible for the non-traumatic symptoms of this condition [18]
A unique feature of the HHSDH in the present patient was the persistent ASDH, as visualized by serial MRI on days 4, 12, and 18 after onset.
ASDH is known to resolve more quickly when a mixture of cerebrospinal fluid (CSF) resulting from the rupture of the arachnoid membrane is present [19]. Given this fact, it is possible that the ASDH in the present patient was trapped in an anatomical compartment without admixture of CSF. As indicated by the MRI findings of the HHSDH, the location of the ASHD in the present case may be said to coincide with the DBCL.
The present case is invaluable because it demonstrates that IASDH can result from a mild, occipital impact. Particularly relevant here is the thin holohemispheric appearance on neuroimaging studies, which has been suitably termed holohemispheric subdural hematoma (HHSDH). Also noteworthy in the present case is the long-term presence of HHSDH with minimal reduction of the ASDH. The mechanism underlying this phenomenon may involve the entrapment of the hematoma in the DBCL in the absence of any communication with the surrounding structures. This phenomenon may indicate that a fluid collection in the DBCL existed before the development of the HHSDH, which was induced by a non-traumatic or mild head impact.
Nobuhiko Aoki (corresponding author with no coauthors) conceived the study and conducted a search of the literature.
This article does not include any data or material that can be provided.
This study was approved by the ethics committee of Bethlehem Garden Hospital and Tokyo Metropolitan Tama Medical Center. No funding was obtained for this study. The parents/legal guardians provided consent to publish the details of the case described in this report.
The author consents to the publication of identifiable details, which can include photographs, case history, and other details.
None
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
