
Review Article | DOI: https://doi.org/10.31579/2640-1053/191
1Pathology Department of the Mohammed VI University Hospital of MARRAKECH-Morocco.
2Faculty of Medicine and Pharmacy of Guelmim; Ibn Zohr University Agadir.
*Corresponding Author: Imane Boujguenna, Research and Training Center ‘Physical and Chemical Materials Science’ Under Kyiv Taras Shevchenko University and NAS of Ukraine, Kiev, Ukraine.
Citation: Halima. EL KHADRAOUI, Imane. BOUJGUENNA, Chafiaa. BENALLAL, Hind. RACHIDI, Anass. FAKHRI, Hanane. RAIS, et. al., (2024), Hodgkin Lymphomas: Experience of the University Hospital Center Mohammed Vi of Marrakech from January 2011 to February 2024, J Cancer Research and Cellular Therapeutics, 8(3); DOI:10.31579/2640-1053/191
Copyright: © 2024, Imane Boujguenna. this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 14 March 2024 | Accepted: 22 March 2024 | Published: 29 March 2024
Keywords: hodgkin lymphomas (hl); diagnosis; histopathology; immunochemistry
Hodgkin lymphomas (HL) represent 1% of all malignant tumors. It is composed of large mononucleated and multinucleated dysplastic cells, surrounded by a variable mixture of mature, non-neoplastic inflammatory cells. We report a retrospective study, spread over 134 months, involving 218cases collected at the Mohammed VI University Hospital in Marrakech between January 2011 and February 2024. HL is a disease that remains curable in the majority of cases but situations of therapeutic failure and relapses severely compromise the prognosis. Recent research on the molecular abnormalities of tumor cells or background cells has helped guide the therapeutic choice.
Hodgkin lymphomas (HL) represent 1% of all malignant tumors. It is composed of large mononucleated and multinucleated dysplastic cells, surrounded by a variable mixture of mature, non-neoplastic inflammatory cells [1]. On the basis of the immunophenotype and morphology of the neoplastic cells and the cellular background, two major types of HL are recognized: classic HL (CHL) and lymphocytic-predominant nodular Hodgkin's lymphoma (NLPHL). The aim of this work is to study the epidemiological and pathological characteristics of Hodgkin lymphoma.
We report a retrospective study, spread over 134 months, involving 218cases collected at the Mohammed VI University Hospital in Marrakech between January 2011 and February 2024.
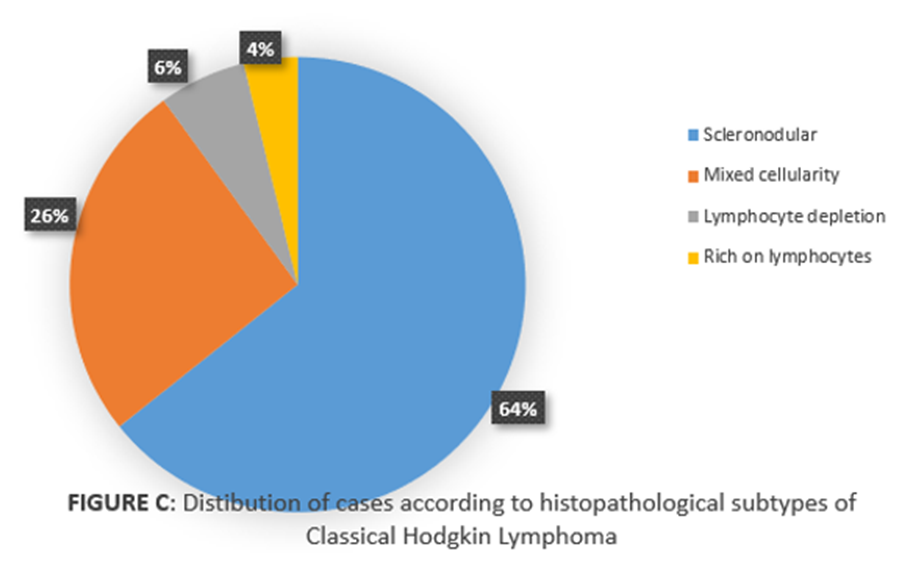
Our results showed 2 frequency peaks in two age groups, the 1st between 15 and 30 years old noted in 56% of cases and the 2nd in patients aged over 50 years in 25.5% of cases. The sex ratio M/F was 1.4. The study material mainly focused on lymph node biopsies, whether superficial or deep (89.9% of cases), the cervical location of which was found in 77% of cases. Extranodal material represented 10.1% with an osteomedullary location in 6.5% of cases, three cases at the skin level, 3 cases at the pulmonary level and 2 cases at the tonsillar level. The histological and immunohistochemical study showed a percentage of 96.1% of tumors were classical Hodgkin lymphoma (CHL) (figureA) and 3.9% were nodular Hodgkin lymphoma with lymphocytic predominance (figureB). Concerning classical Hodgkin lymphoma; the scleronodular subtype is predominant, diagnosed in 135 patients or 64% of cases, the mixed cellularity subtype is diagnosed in 54 patients or 26%, then the lymphocyte depletion subtype is diagnosed in 13 patients (6% of cases) and the subtype rich on lymphocytes is the rarest in our series, found in 8 patients or 4% (figure C).
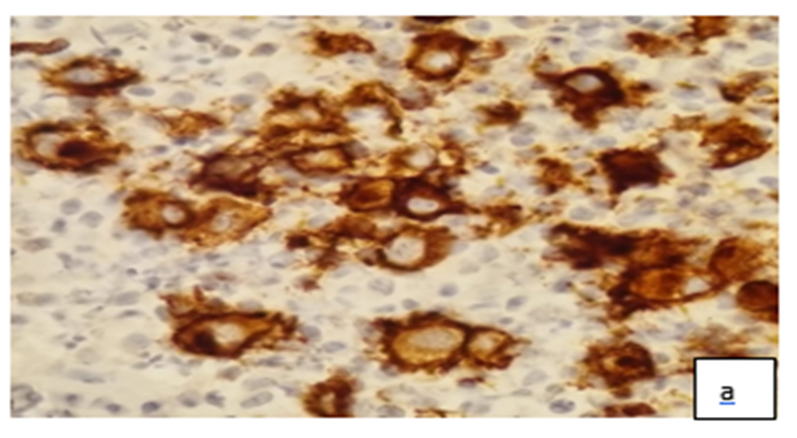

Figure A: a -Reed-Sternberg cells (black arrow). The background is made by small round lymphocytes, plasma cells and eosinophils (x20). b- Membrane expression of Reed-Sternberg cells to the anti CD30 antibody (x40)

Figure B: large tumor cells having a multilobed nucleus describing a popcorn appearance (black arrow)
Hodgkin lymphoma (HL) is a tumor of the lymphatic system representing one of the most common cancers in young adults (2). Histopathologically and immunohistochemically, 95% of HL cases are classified as classic HL (CHL), including nodular sclerosing, mixed cellularity, lymphocyte-rich, and lymphocyte-depleted HL subtypes (1,3). In 5% of cases, NLPHL is diagnosed (1,3, 4, 5). Classic HL is characterized by the presence of Hodgkin and Reed–Sternberg (HRS) cells expressing the anti-CD30 antibody and which are surrounded by variable inflammatory cells, while the malignant cells of NPLHL are large cells with polylobed nuclei or multilobed called “popcorn” cells or “lymphocytic predominant cells”. They are surrounded by mature lymphocytes and are characterized by their CD20 positivity and CD30 negativity (1). Which agrees with our result. Hodgkin lymphoma most often involves in the lymph nodes. Their diagnosis is based on a study of an excisional biopsy, most often lymph node. Prognostic models to identify patients at high or low risk for recurrence have been developed (6,7,8). The initial treatment for patients with Hodgkin lymphoma is based on the histologic characteristics of the disease, the stage at presentation, and the presence or absence of prognostic factors associated with poor outcome (4, 9, 10). Patients with early-stage Hodgkin lymphoma commonly receive combined-modality therapies that include abbreviated courses of chemotherapy followed by involved-field radiation treatment. In contrast, patients with advanced-stage Hodgkin lymphoma commonly receive a more prolonged course of combination chemotherapy, with radiation therapy used only in selected cases. For patients with relapse or refractory disease, salvage chemotherapy followed by high-dose treatment and an autologous stem cell transplant is the standard of care (4).
HL is a disease that remains curable in the majority of cases but situations of therapeutic failure and relapses severely compromise the prognosis. Recent research on the molecular abnormalities of tumor cells or background cells has helped guide the therapeutic choice.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
