
Case Report | DOI: https://doi.org/10.31579/2690-4861/093
*Corresponding Author: Eric Hsieh, MD, FACP, Vice Chair, Educational Affairs, Director, Residency Program Department of Medicine, Keck School of Medicine of USC, Los Angeles, CA.
Citation: S Quon, E Hsieh. (2020) HIV as A Cause of Acute Liver Injury. International Journal of Clinical Case Reports and Reviews. 4(5); DOI: 10.31579/2690-4861/093
Copyright: © 2020 Eric Hsieh, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 07 November 2020 | Accepted: 04 December 2020 | Published: 07 December 2020
Keywords: hepatology; hiv
While hepatitis is the most common infectious cause of acute liver injury, although rare, acute human immunodeficiency virus (HIV) infection should be considered in the workup for infectious causes of acute liver injury. We present a case of a 36 year old woman with no past medical history who presented to the hospital for 8 days of abdominal pain and nausea worsened with food. Labs were significant for lymphocytopenia, transaminitis, elevated alkaline phosphatase, and direct bilirubinemia. Viral hepatitis serologies were negative and imaging showed nonspecific gallbladder wall thickening, no gallbladder stones, no intra or extra-hepatic biliary ductal dilatation. No evidence of congestive heart failure. Serologies for cytomegalovirus (CMV), Epstein Barr virus (EBV), rickettsia, enterovirus, adenovirus, and parvovirus were negative. Workup for autoimmune liver disease was also negative. Liver biopsy was notable for a focus of granulomatous necrosis, suggestive of infectious or drug induced etiology. During this admission, patient was also found to have a new diagnosis of HIV with CD4 count of 235. Patient was started on bictegravir, emtricitabine, and tenofovir alafenamide with progressive improvement and eventual resolution of AST, ALT, alkaline phosphatase, and bilirubin elevation since starting anti-retroviral therapy.
The differential diagnosis of acute liver injury is broad, including ischemic, infectious, autoimmune, pancreatobiliary, drug induced, and malignant infiltration [1]. While hepatitis is the most common infectious cause of acute liver injury, acute human immunodeficiency virus (HIV) can also cause acute liver injury. Elevated liver enzymes in the setting of HIV is usually attributed to co-infection with hepatitis B and C, side effect of anti-retroviral medications, or opportunistic infections. However, acute liver injury can also be the result of direct toxicity of HIV [2, 3]. This is supported by evidence of HIV compartmentalization in liver tissue and identification of liver specific amino acids, which supports the presence of HIV variants replicating in the liver [4, 5]. Furthermore, there is a significant correlation between AST and ALT elevation and HIV viral load in patients without concomitant hepatitis infection or ART use [6]. Acute HIV infection should be considered in the workup for infectious causes of acute liver injury.
Case:
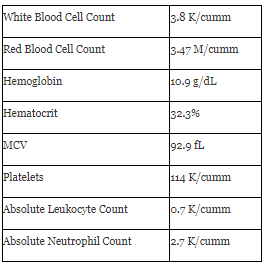
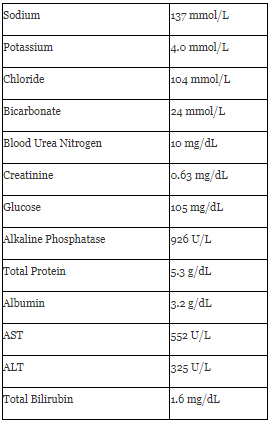
A 36 year old woman with no past medical history presented to the hospital for 8 days of abdominal pain and nausea worsened with food. Patient was clinically well appearing, and abdominal exam, cardiac, and pulmonary exam was unremarkable. Patient was afebrile, normotensive, no tachycardia, no tachypnea or hypoxia. Abdominal exam was unremarkable. Labs were significant for lymphocytopenia, normocytic anemia, transaminitis, elevated alkaline phosphatase, and elevated bilirubin (Table 1).
Complete Metabolic Panel
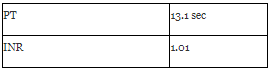
Coagulation studies
Patient denied medications or supplements, alcohol use, smoking, or recreational drug use, and was monogamous with one male partner. Initial workup included negative viral hepatitis serologies and abdominal ultrasound with nonspecific gallbladder wall thickening, pericholecystic edema/trace fluid, no gallbladder stones, no intra or extra-hepatic biliary ductal dilatation. Patient’s BMI was 19, hemoglobin A1c 4.9. A transthoracic echocardiogram showed an ejection fraction 60-65%, no diastolic dysfunction, and no valvular abnormalities. Magnetic resonance cholangiopancreatography also showed nonspecific gallbladder wall thickening, small amount of pericholecystic fluid, no gallstones, intra or extra hepatic bile duct dilatation. Workup for infectious causes of acute liver injury, including cytomegalovirus (CMV), Epstein Barr virus (EBV), rickettsia, enterovirus, adenovirus, and parvovirus serologies, was negative. Antinuclear antibody, liver kidney microsome antibody, smooth muscle antibody, and anti-mitochondrial antibody were negative. Ceruloplasmin level was also within normal. Liver biopsy was performed and pathology was notable for a focus of granulomatous necrosis. There was no portal fibrosis, no steatosis or Mallory bodies, no alpha-1-antitripsin inclusions, no tumor, normal bile ducts, trace to 1+ iron staining in hepatocytes, and absent to mild lymphocytic infiltrates. Stains for fungus, acid fast bacilli, and cytomegalovirus on liver biopsy were also negative. As part of workup for nonspecific abdominal pain and nausea in reproductive age female, screening for sexually transmitted infections was also performed. Urine gonorrhea and chlamydia was negative, but HIV antibody/antigen screen and HIV 1 RNA qualitative screen were positive. HIV 1 viral load was greater than ten million, and CD4 count was 235. Patient was started on bictegravir, emtricitabine, and tenofovir alafenamide with progressive improvement and eventual resolution of AST, ALT, alkaline phosphatase, and bilirubin elevation since starting anti-retroviral therapy.
We present a case of acute HIV infection presenting with nonspecific abdominal pain and elevated liver enzymes in a mixed cholestatic and hepatocellular pattern. Patient had no known medication exposures concerning for drug induced liver injury. Given patient had normal A1c and BMI, there was low suspicion for non-alcoholic fatty liver disease. Patient had normal cardiac function on transthoracic echocardiogram, therefore unlikely to have congestive hepatopathy. Imaging was negative for portal vein thrombosis or obstructive causes of acute liver injury. Serologies for common infectious causes of liver injury, including hepatitis were negative. Autoantibodies for autoimmune liver disease were also negative. Liver biopsy findings were nonspecific, however findings consistent with alcoholic hepatitis or nonalcoholic fatty liver disease, alpha-1-antitripsin deficiency, malignancy, hemochromatosis, and hemophagocytic lymphohistiocytosis were notably absent. Given nonspecific pathology findings, negative workup for other etiologies, and new diagnosis of HIV, patient was diagnosed with acute liver injury secondary to acute HIV infection. Furthermore, patient had progressive improvement and resolution of transaminitis and alkaline phosphatase elevation correlating with initiation of anti-retroviral therapy.
Conclusion:
While less common than other causes, HIV is associated with several mechanisms of acute liver injury including toxicity associated with anti-retroviral therapy, opportunistic infection, co-infection with hepatitis viruses, and direct injury from HIV. Evaluation for acute HIV infection should be included in the workup for acute liver injury.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
