
Case Report | DOI: https://doi.org/10.31579/2641-0419/129
*Corresponding Author: Kristin Ellison, MD Division of Cardiovascular Medicine; The Gill Heart & Vascular Institute 900 South Limestone Street, CTW 326 Lexington, KY 40536.
Citation: Kristin Ellison., Andrew Kolodziej., Sateesh Kesari., Karam Ayoub., Ethan Fry., Aaron Hesselson., (2021) His Bundle Pacing with Recruitment of Right Bundle Branch after Orthotopic Heart Transplant. J. Clinical Cardiology and Cardiovascular Interventions, 4(3); Doi:10.31579/2641-0419/129
Copyright: © 2021 Kristin Ellison, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, sand reproduction in any medium, provided the original author and source are credited.
Received: 22 January 2021 | Accepted: 01 February 2021 | Published: 08 February 2021
Keywords: orthotopic heart transplant; primary graft failure; his bundle pacemaker; myocardial biopsy
The incidence of permanent pacemaker implant after orthotopic heart transplant is between 2-24%. We present a 63-year-old male with ischemic cardiomyopathy who underwent orthotopic heart transplant. His post-operative course was complicated by recurrent asystole from sinus bradycardia and complete heart block. He had baseline right bundle branch block and right ventricular dysfunction. The decision was made to proceed with His-bundle pacing to provide physiologic cardiac activation, and provide anatomical benefit for subsequent endomyocardial biopsy. He did well after receiving a His bundle pacemaker with recruitment of his right bundle branch.
AF - Atrial Fibrillation, AV-Atrial ventricular, PPM - Permanent Pacemaker, SND - Sinus node dysfunction, HBP - His bundle pacing, CHB – Complete Heart Block, POD - Post-Operative Day, RBBB - Right Bundle Branch Block, LBBB - Left Bundle Branch Block, OTH - Orthotopic Heart Transplant, RV - Right Ventricle, CRT -Cardiac Resynchronization Therapy
Introduction
The incidence of permanent pacemaker implant after orthotopic heart transplant is between 2-24%. Most early implants are for sinus node dysfunction (SND), while atrioventricular block (AVB) contributes to later implants [1,2]. His bundle pacing allows for physiologic cardiac depolarization and can be beneficial compared to traditional pacing techniques [3,4]. His bundle pacing can also overcome bundle branch block from His-purkinje disease by recruiting bundle fibers beyond the level of block [5,6]. We present a 63-year-old male with ischemic cardiomyopathy who underwent orthotopic heart transplant. His post-operative course was complicated by recurrent asystole from sinus bradycardia and complete heart block with baseline right bundle branch block and right ventricular dysfunction. He did well after subsequent His bundle pacemaker with successful recruitment of the right bundle branch.
Case Report
A 63-year-old male with past medical history of hypertension, diabetes, coronary artery disease, ischemic cardiomyopathy with an ejection fraction (EF) of < 20% on continuous infusion of intravenous Milrinone, chronic obstructive lung disease, and pulmonary hypertension, underwent orthotopic heart transplant (OHT) with bi-caval anastomosis. Immediately following surgical anastomosis, the donor’s left ventricle became dilated and hypokinetic in addition to significant right ventricular (RV) failure. During reperfusion, he had several episodes of ventricular fibrillation that were successfully treated with defibrillation. Twenty minutes after coming off bypass, his condition deteriorated necessitating placement back on bypass. After starting inotropic and vasoactive agents, Milrinone and norepinephrine, patient was able to be slowly weaned off of bypass. Temporary epicardial pacer leads were placed secondary to sinus bradycardia and the sternotomy site was closed appropriately.
He received induction immunosuppressive therapy with intravenous Basiliximab and Methylprednisolone. On postoperative day one (POD 1), vasoactive agents were weaned off, and he was successfully extubated. His post-operative course was complicated by acute renal failure requiring intermittent renal replacement therapy. His intrinsic rhythm was normal sinus rhythm with rates between 73 and 110 beats per minute (BPM), up until POD 13. At that time, patient had an episode of feeling poorly while standing and was placed back in bed, but subsequently suffered transient loss of consciousness. Patient’s telemetry during this episode revealed sinus bradycardia followed by complete heart block (CHB). He had several minutes of a ventricular escape rhythm which then converted into atrial fibrillation (AF) lasting several minutes, before spontaneous converting back to normal sinus rhythm at 80-90 beats per minute. Patient was not on any atrialventricular (AV) nodal blocking agents, and all RV endomyocardial biopsies were negative for acute rejection.
The following morning, he had another episode of sudden onset sinus slowing and CHB leading to asystole requiring transcutaneous pacing for nearly 10 minutes. Due to recurrent episodes of unexplained sinus bradycardia and CHB the decision was made to proceed with implanting a dual chamber His bundle permanent pacemaker (HBP).
The left cephalic vein was accessed by cut down. A C315-His non-deflectable sheath was used with the 3830 Medtronic His bundle lead. Mapping of the His bundle was done through unipolar hook up of the pacing lead and electrograms before and after fixation are shown in (figures 1A and B).
The implanted lead values were threshold 0.75 Volts at 1 millisecond, R wave of 2.8 millivolts, and an impedance of 663 Ohms. Pacing from this sight also recruited the right bundle as shown in (figure 1C).
Figure 1: Electrograms during His Bundle Lead Placement

The sheath was slit, and the lead was secured. The atrial lead was placed. During the case, the patient had another episode of sinus bradycardia and CHB associated with hypotension. HBP pacing rate was increased to 90 bpm with immediate improvement of blood pressure. Electrocardiograms (ECGs) before and after HBP placement are provided in Figure 2, which demonstrate the patients underlying right bundle branch block (RBBB) (figure 2A) with favorable narrowing following HBP (figure 2B).
Figure 2: 12 lead ECGs Before and After His Bundle Pacing

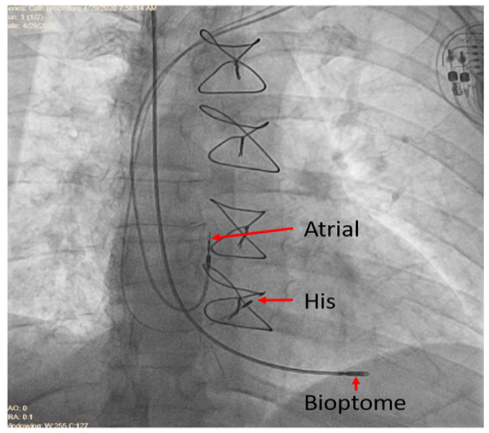
He continued to undergo RV endomyocardial biopsies as part of allograft rejection surveillance program without complications. The location of the bioptome relative to the His lead is shown with fluoroscopy in (figure 3). Patient continued to recover after HBP placement and was successfully discharged from the hospital.
Figure 3: Fluoroscopic Image during Myocardial Biopsy
Indications for permanent pacing after OHT are bimodal with early and late implantations [1, 2]. In adults, early implants tend to be for SND. Surgical trauma, surgical technique, myocardial preservation and reperfusion, cardiac denervation, and donor characteristics all play a role in post-transplant SND. SND may resolve with limited pacing required after 6 months. Late PPM implantations, 1-6 months post-transplant, are for both SND and AVB and may correlate with acute rejection or transplant vasculopathy. The bicaval technique introduced in the early 90’s has been associated with decrease PPM requirements [2]. A study by Mallidi in 2017, correlated pre-transplant ischemic cardiomyopathy, increased donor age, and number of treated rejection episodes with greater PPM implantation [1]. Our patient experienced episodic asystole resulting from both SND and CHB with baseline RBBB on Milrinone for primary graft failure. Patient had pulmonary hypertension pre-operatively and RV failure post-operatively.
Significant data has been emerging regarding the clinical benefits of HBP compared to traditional RV pacing [3, 4]. HBP results in the activation of the heart through the intrinsic conduction system. When achieved, this avoids the harmful consequences imposed by standard RV pacing such as: ventricular dyssynchrony, impaired contractility, increased mitral regurgitation, decline in ejection fraction, and increased burden of atrial fibrillation [7-9].
HBP can also be utilized to recruit/activate the left or right bundle branches beyond the level of the block within the His bundle. Which subsequently narrows the QRS and provides cardiac resynchronization therapy (CRT) [5,6,10]. HBP for LBBB was shown to be equivalent to CRT with Biventricular pacing at the late-breaking trial presented at the Heart Rhythm Society in May 2019 [6]. While HBP in an OHT with underlying LBBB has previously been described in the literature [11], HBP with underlying RBBB has not. Sharma, et al. presented data on patients with low EF and RBBB, with successful HBP achieved in 37/39 patients. In 78% of these patients, the RBBB was narrowed with resultant improved heart failure outcomes. As RBBB is associated with RV asynchrony, the proposed benefit of RBBB narrowing was resynchronization of the RV. The other possibility is AV optimization without deleterious effects of conventional RV pacing [6].
Our patient had potential need for ventricular pacing with episodic CHB and baseline RBBB. HBP avoided the harmful consequences of RV pacing in this patient with primary graft failure. Our patient also suffered from RV failure in setting of pulmonary hypertension and recruitment of the RBBB provided the potential to synchronize and optimize RV function. An additional merit to HBP in transplant populations is the proximal position of the His lead, leaving the full RV septum available for biopsy (Figure 3). Two months out from his transplant, his pacer requirements at a rate of 90 BPM are 87% in the atrium and 99.2% in the ventricle. Thresholds remain stable at 1.65 volts at 0.4 milliseconds with R wave of 4.4 millivolts and impedance of 399 ohms.
Conclusions
Pacemakers are occasionally indicated post OHT. Due to the complex nature of transplant graft function, HBP is an attractive pacing technique in this population. Our patient received a dual-chamber, His bundle pacemaker. The atrial lead provides atrial rate support and facilitates the management of atrial fibrillation, while the His bundle lead provides physiologic pacing and recruitment of the RBBB in a patient with primary graft failure. Use of His bundle pacing will prevent the deleterious effects of RV pacing, leave the RV septum available for biopsy, and the correction of his underlying RBBB may provide benefit to his RV function.
Disclosures all Authors: None
Conflict of interest: None
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
