
Case Report | DOI: https://doi.org/10.31579/2690-1897/135
Department of Thoracic Surgery, Sureyyapasa Chest Diseases and Thoracic Surgery Training and Research Hospital, Istanbul, Turkey.
*Corresponding Author: Onur Derdiyok. Department of Thoracic Surgery, Sureyyapasa Chest Diseases and Thoracic Surgery Training and Research Hospital, Istanbul, Turkey.
Citation: Onur Derdiyok. (2023). Hepatothorax: a rare entity in blunt trauma, Journal of Surgical Case Reports and Images 6(1) DOI: 10.31579/2690-1897/135
Copyright: © 2023. Onur Derdiyok. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 14 November 2022 | Accepted: 29 December 2022 | Published: 02 January 2023
Keywords: diaphragmatic hernia; hepatothorax; diaphragmatic rupture
Post-traumatic right -sided diaphragmatic hernia occurring after diaphragmatic rupture is a very rare condition because the right diaphragm is protected by the liver. However, its incidence increases after severe trauma on the right side. Liver herniation through ruptured diaphragm is one of the causes of severe atelectasis in the right lung which may cause respiratory distress and hemodynamic impairment. Diaphragmatic rupture is an emergency. Herein, we present a 56-year-old male patient with right-sided diaphragmatic rupture and hepatothorax developed three years after a traffic accident happened three years
Diaphragmatic rupture is a clinical condition that occurs after a sudden increase in intra-abdominal pressure. Diaphragmatic rupture is detected in 1-7% of patients with major blunt, and 10-15% of patients with penetrating trauma. Left diaphragmatic ruptures are more common [1]. Intrathoracic herniation of abdominal organs following diaphragmatic injury is rare and difficult to identify. Stomach, spleen, and colon are mostly herniated organs [2]. In this study, we present a 56-year-old male patient who was operated for Right-sided diaphragmatic rupture and hepatothorax.
A 56-year-old male patient was admitted to our clinic with shortness of breath and pain on his right side. He was hemodynamically stable despite the presence of hypertension. The patient's heart rate ( 98 bpm: sinus rhythm), blood pressure (110/70 mmHg), and arterial oxygen saturation (93%) were as indicated. He had a motor vehicle accident three years previously.. His breathing sounds decreased during auscultation of the right hemithorax. Elevated right hemi-diaphragm was seen on posterior anterior chest radiograms (Figure 1).
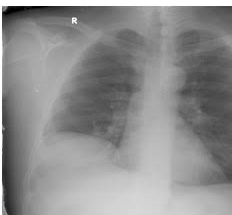
Figure 1
The subsequent thoracic CT demonstrated the rupture of the right hemi-diaphragm and hepatic herniation into the right hemithorax (Figure 2). Due to this life-threatening emergency situation of the hemodynamically unstable patient, thoracotomy was performed through the 6th intercostal space. Diaphragmatic dislocation was observed extending from the hemidiaphragmatic chest wall to the anterior lateral rib cage. The liver was completely surrounded by the chest wall, with the upper part of the chest wall facing upwards (Figure 3). After positioning the liver back into the abdominal cavity, the diaphragmatic rupture side was closed with silk 2-0 sutures, and the diaphragm was then repositioned in the rib cage. Any adverse event was not detected during the 14-month follow-up period.
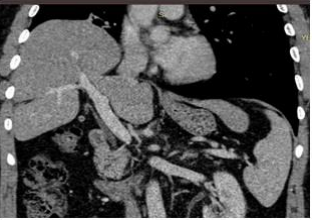
Figure 2

Figure 3
Diaphragmatic rupture is a rare complication of abdominal or thoracic trauma. It has been reported in 10-15% of penetrating trauma, and 10-15% of blunt trauma patients. Approximately 1% of all diaphragmatic tears occur spontaneously and occur with sudden increase in abdominal pressure due to severe physical exertion, sudden bending movements, birth and severe cough. The incidence of diaphragm rupture after thoracoabdominal trauma is 0.8-5% in the early period and 30% in the late period. ' stop [3]. The case also occurred late after the traffic accident. A systematic review of the literature shows that there were only 6 cases of right-sided diaphragmatic rupture and 13 cases of liver hernia, and a delayed rupture of 24 hours to 50 years from trauma in the literature. In studies of non-traumatic diaphragmatic rupture, the overall rupture of the diaphragm is approximately 1% [4]. Right-sided diaphragm ruptures are a rare condition with nonspecific clinical and radiological findings and rapid diagnosis. Interestingly, early detection can often lead to serious complications. Various hypotheses have been made for late diaphragm rupture. The first hypothesis suggests that the diaphragm muscle develops a process of lifelessness that occurs several hours or days after trauma. The most likely explanation is that diaphragmatic injuries occur clinically only after intrathoracic herniation of the abdominal organs [5]. The case presented with pain complaints in the right abdominal region. The radiological images were compatible with the clinic. Complicated with intrathoracic herniation of an abdominal organ, diaphragmatic rupture was first described by Sennertus in 1541 by autopsy of a patient who died of a herniated colon due to a diaphragm defect caused 7 months ago [6]. The clinical features of patients with diaphragm rupture are asymptomatic or non-specific. In the acute phase, patients are often considered an emergency with existing injuries that may impair their diagnosis. Chest pain, cough, mania, and shortness of breath are the most common symptoms [7]. There is shortness of breath and pain on the right side of the patient. Computed tomography is a very special tool for the preoperative diagnosis of abdominal thoracic scans in the acute phase. Therefore, if right diaphragm rupture is suspected, a direct abdominal CT should be performed. In this case, abdominal tomography and abdominal USG Surgical repair of hepatotrax should be urgent and should consist of transthoracic or transabdominal approach and liver reduction and diaphragmatic defect repair. The use of intrathoracic or intrathoracic sutures in thoracic tubes represents a classic strategy [8]. The diaphragm was repaired with 2-0 silk sutures. In conclusion, we present a delayed rupture of the right diaphragm complicated by hepatothorax. Pre-operative detection of diaphragm rupture is very important in preventing life-threatening complications such as hepatothorax. Therefore, physicians should develop a later detective trial for rare cases and meet patients with respiratory distress or abdominal symptoms who show signs of sudden abdominal symptoms beginning a few days, months, or years later.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
