
Review Article | DOI: https://doi.org/:10.31579/2639-4162/131
1 Sofia University, University Hospital “Sofiamed” Sofia, Bulgaria,
2 University Hospital “Sofiamed” Sofia, Bulgaria.
*Corresponding Author: Iveta Tasheva, Sofia University, University Hospital “Sofiamed” Sofia, Bulgaria.
Citation: : Iveta Tasheva, Irina Koleva- Ignatova, Nikolay Serafimov, Viktoriya Stancheva, (2023), Hepatocellular Carcinoma with Right Atrial Metastasis, J. General Medicine and Clinical Practice, 7(1); DOI:10.31579/2639-4162/131
Copyright: : © 2023, Iveta Tasheva. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 06 December 2023 | Accepted: 26 December 2023 | Published: 03 January 2024
Keywords: cardiac tumours; hepatocellular carcinoma; right atrium invasion
Cardiac tumours may be primary or secondary-metastatic (malignant).
Secondary cardiac tumours are much more common than primary cardiac tumours. Their frequency on large anatomical studies varies between 3.4% and 13.9%. Though cardiac metastases may originate from any malignant tumor, melanomas have the greatest propensity for cardiac involvement, and also carcinomas of the thorax, including breast, lung, and esophageal [12,13]. The routes of metastasis include direct invasion, hematogenous, lymphatic, or transvenous, especially through the inferior vena cava [9,10]. Cardiac involvement should be suspected or sought in any patient with a known malignancy who develops new cardiovascular signs or symptoms. Imaging methods - echocardiography, computed tomography (CT) and MRI, are essential in establishing the diagnosis and the invasion of the tumour in the cardiac cavity. The severe evolution of secondary cardiac tumors depends on the extension of the primary tumour, but also on the severity of the clinical cardiac manifestations. Generally, the treatment is surgical. A correct diagnosis is important in the clinical setting since cardiac metastases are able to induce sudden cardiac death1.
Primary hepatocellular carcinoma (HCC) is the sixth cause of cancer in the world and the second cause of cancer mortality worldwide, with more than 830,000 deaths recorded annually2.
We present a case of HCC growth into the vena cava inferior (VCI) and invasion into the right atrium (RA).
HCC- Hepatocellular carcinoma
VCI-vena cava inferior
RA-right atrium
TTE- transthoracicechocardiogram CT- computed tomography
A 60-year-old man recently diagnosed with cirrhosis and HCC, secondary to hepatitis B, presented to the cardiology department for dyspnea and new onset bilateral lower extremity edema, rapidly progressing over 2 weeks. The patient is receiving treatment with Lamivudine 100mg.
The patient`s hemodynamic parameters showed regular sinus rhythm of 74 beats per minute, blood pressure of 130/80 mm Hg, heart sounds without murmurs and bilateral lower limb edema. There was no jugular venous distension, and his lungs were clear to auscultation.
Initial laboratory findings:

The ECG showed normalsinus rhythm.
The transthoracic echocardiogram (TTE)registered normal left ventricle systolicfunction without wall motion abnormality or significant valvular abnormality. Large echogenic 45/37mmmass, extending from the intrahepatic VCI to the RA, with no obstruction of the right ventricle. (Figure1,2)
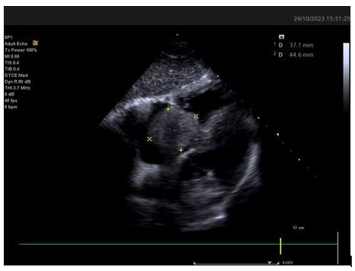
Figure 1: Huge right atrialmass

Figure 2: Mass extending from the intrahepatic VCI to the RA
CT scan of the chest and abdomen showed a large heterogeneous and roundedmass in the liver, with an axialdiameter of 13.54 cm (Figure3) and a coronary diameter of 13.84 cm (Figure 4); evidence of tumor extension to the adjacent VCI, reaching the RA (Figure5); thrombosis of the two common iliac arteries, the external and internal iliac veins on the right, as well as the proximal4.71 cm of the VCI (Figure 6); small amountof perihepatic ascites,and pulmonary nodules.
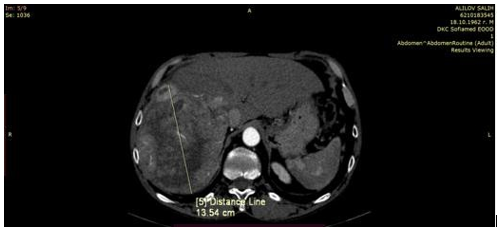
Figure 3.

Figure 4.

Figure 5.

Figure 6.
The CT scan was followed by a multidisciplinary discussion. Due to the advanced stage of the disease, it was concluded that the patient is indicated for palliative care. Tumor resection and liver transplantation are some of the treatment methods used in such cases, but their prognosis remains poor, with a median survival of only a few months [3,4,5]. Some of the limiting factors of surgical intervention include poor hepatic reserve, potential postoperative complications, and early recurrence [6,7].
Тransarterial chemoembolization, chemotherapy and radiotherapy are some of the potential treatment options, to relieve symptoms and improve quality of life [4,5,11]. The multimodality of cardiac imaging is important, because the diagnosis may be overlooked due to non-specific symptoms. Screening TTE is recommended in patients with HCC, even in the absence of cardiac manifestations. HCC with right atrial metastasis is associated with a high risk of cardiopulmonary complications, tricuspid stenosis or insufficiency, ventricular outflow obstruction, cardiac arrhythmias, pulmonary embolism, pulmonary metastases, heart failure or sudden death.
HCC with VCI and RA invasion has a poor prognosis and leads to an increased risk of cardiacdeath. It is rare and difficult to diagnose and treat8, because of the absenceof cardiac manifestations. Severe myocardial damagecaused by the tumor mass may occur, impairing cardiac function gradually without specific symptoms. Our clinical case shows that intrahepatic HCC can disseminate and invade the heart. This aims to highlight the importance of maintaining regular screening TTE for metastases in patients with HCC, so that we can detect the early stagesof the disease and initiatethe treatment
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
