
Case Report | DOI: https://doi.org/10.31579/2768-2757/119
1Department of General, Visceral and Transplant Surgery, University Medical Center of the Johannes Guten-berg-University Mainz, 55131 Mainz, Germany.
2Department of Diagnostic and Interventional Radiology, University Medical Center of the Johannes Gutenberg-University Mainz, 55131 Mainz, Germany.
3Department of Pathology, University Medical Center of the Johannes Gutenberg-University Mainz, 55131 Mainz, Germany.
*Corresponding Author: Lisa-Katharina Gröger, Department of General, Visceral and Transplant Surgery, University Medical Center of the Johannes Guten-berg-University Mainz, 55131 Mainz, Germany.
Citation: Lisa K.Gröger, Felix Hahn, Beate Straub, Fabian Bartsch, Hauke Lang, (2024), Hepatocellular Carcinoma Mimicking Focal Nodular Hyperplasia, Journal of Clinical Surgery and Research, 5(3); DOI:10.31579/2768-2757/119
Copyright: © 2024, Lisa-Katharina Gröger. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 15 March 2024 | Accepted: 26 March 2024 | Published: 10 April 2024
Keywords: FNH; HCC; AFP; MRI-scan; hepato-biliary surgery; benign liver tumors; follow-up
Focal nodular hyperplasia (FNH) is a common benign liver lesion, mostly solitary, and with no evidence of malignant transformation over time. The diagnosis can usually be made by imaging modalities with distinct features in magnetic resonance imaging (MRI) and computed tomography (CT) scans. We present a case series of three patients with solitary liver tumors which were, based on radiological features, first diagnosed to be large FNH. The patients were sent to our center for second opinion and probable treatment. Indication for resection was given because of nonconclusive radiologic imaging in the first, substantial growth progression in the second and elevated alpha fetoprotein (AFP) in the third case. Histology revealed well to poor differentiated hepatocellular carcinoma (HCC). FNH tends to show a distinct pattern in imaging modalities, but HCC can mimic FNH. The MRI-scan using hepatotropic contrast agent is the most sensitive imaging modality to diagnose FNH. AFP is usually not elevated in FNH. Asymptomatic FNH does not require surgery but a reliable diagnosis is crucial. In case of an un-certain diagnosis surgery should be offered to patients. In cases with a progression in size, an elevated level of AFP should be suspicious. Generally, an over-therapy via surgery should be avoided and follow-ups of a newly diagnosed FNH including measurement of AFP are advisable to detect alterations.
AFP: alpha fetoprotein;
CT: computed tomography;
EASL: European Association for the Study of the Liver;
FNHF: ocal nodular hyperplasia;
HCC: hepatocellular carcinoma;
MRI: magnetic resonance imaging;
TACE: transarterial chemoembolization;
UICC: Union for International Cancer Control.
We report a case series of three female patients with tumors, that were found radiologically highly suspicious for a FNH that turned out to be histologically proven hepatocellular carcinoma (HCC). The patients were each primarily and externally diagnosed as FNH, based on imaging modalities with typical central scarring. All three were solitary tumors in a non-cirrhotic liver and without underlying liver disease. The patients were sent to our center for a second opinion and further treatment mainly because of the size of the tumor.
In general, focal nodular hyperplasia (FNH) is a benign, mostly solitary liver lesion originating from hepatocytes. Diagnosis is usually made by CT or MRI by distinct features including the presence of a central scar and central artery. A reliable diagnosis with exclusion of a malignant lesion is crucial as in asymptomatic patients FNH treatment is not necessary. [1]
Through this case report, we aim to emphasize the importance of accurate diagnosis and provide recommendations for the surveillance and treatment of newly diagnosed focal nodular hyperplasia (FNH).
All data from the three patients were gathered at our center and stored in an institutional database. Patients’ characteristics, surgical procedure, histological outcome, and further information are shown in Table 1
The first patient was a 41-year-old female who was referred for a second opinion after receiving the diagnosis of a large FNH of the right liver lobe externally (Figure 1). No dedicated hepatocyte-specific contrast phase had been performed. AFP was within normal range. We indicated the explorative laparotomy due to a slight washout phenomenon in the venous phase which is not entirely typical for FNH. Intraoperative frozen section confirmed a hepatocellular carcinoma and a bisegmental resection of the segments 5 and 6 (H56 according to the ‘New World’ terminology [2]) plus hilar lymphadenectomy was performed. Postoperative course was uneventful but early recurrence was diagnosed after four months and repeated resection was performed (H8’). A second recurrence led to a completion as formal right hemihepatectomy (H78) and subsequent treatment with Sorafenib. In the further course a local therapy with TACE was conducted after findings of a third recurrence. The patient passed away two years after the primary diagnosis of HCC.
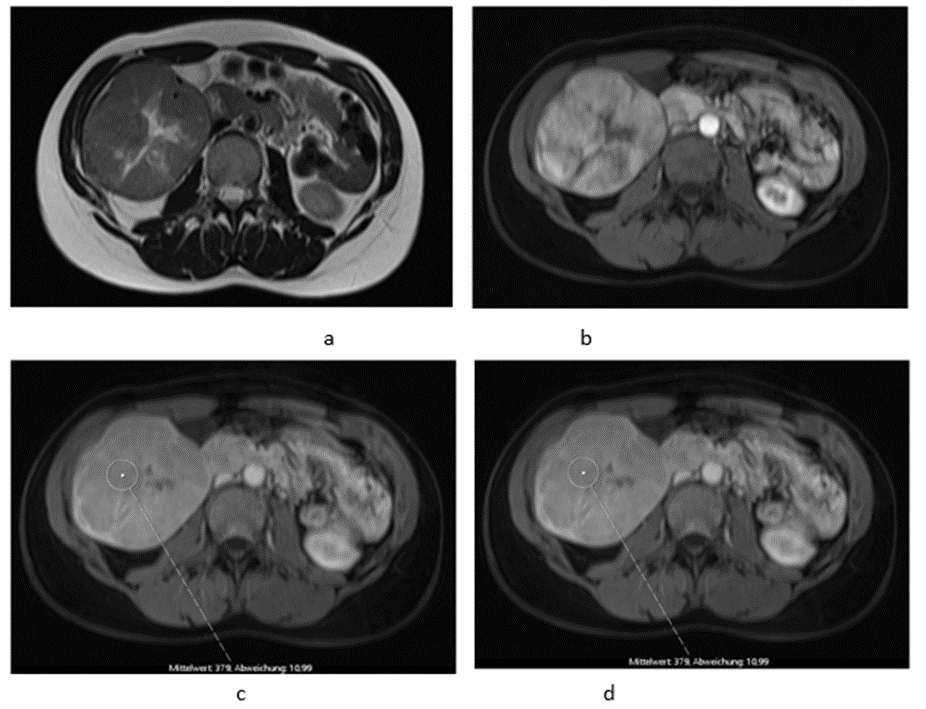
Figure 1:Pre-operative MR imaging Patient 1: (a) T2 TSE sequence depicting central scar; (b) T1 sequence with fat saturation in arterial phase depicting intense early arterial enhancement. (c/d) Slight signal drop in the tumor tissue (c) compared to healthy liver venous phase (d). No dedicated hepatobiliary imaging was performed.
The second patient was referred to our out-patient clinic with a liver lesion of the left lobe, after it had been growing constantly over 7 years. A FNH had been diagnosed at the age of 23, which had met the typical MRI-criteria including contrast retention in hepatobiliary imaging and the patient had been in regular follow-ups (Figure 2). Because of the tumor growth and inhomogeneity along the tumor capsule we performed a left hepatectomy (H234’) (Figure 2 d). The final histological findings revealed an HCC and the patient is in regular follow-ups since without evidence of recurrence for over 44 months until today.
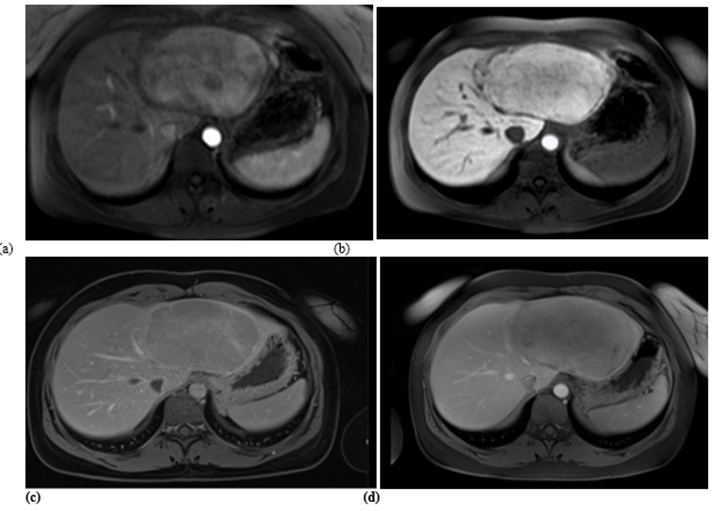
Figure 2: Pre-operative MR imaging Patient 2: (a) Arterial phase imaging depicting hyperen-hancement of liver lesion; (b) T1 sequence with fat saturation in hepatobiliary phase depicting isointensity to liver; (c) and (d) T1 sequence with fat saturation post contrast showing size pro-gression from (c) (d) in 3 years.
The third patient was 53 years old when externally a FNH was diagnosed in a MRI (Figure 3). Comparable to patient 1, no dedicated delayed hepatobiliary phase had been performed. A follow-up after 3 months was scheduled with AFP as laboratory testing this time, which turned out to be significantly increased with a value of > 400000ng/ml. Four weeks later the patient presented at our center and the AFP had risen to 980128 ng/ml. These values clearly indicated the presence of HCC and FNH as
initial misdiagnosis. We conducted a central resection of segments 4, partially 5 and 8 as well as Segment 1 (H145’8’-RHV). Resection and reconstruction of the right hepatic vein was necessary to achieve R0-status. The patient is tumor-free within follow-up for 20 months until today. In the postoperative course the AFP levels decreased to 5529 ng/ml after one month, to 4.9 ng/ml after three months, and remained below 2.5 ng/ml until seven months after resection.
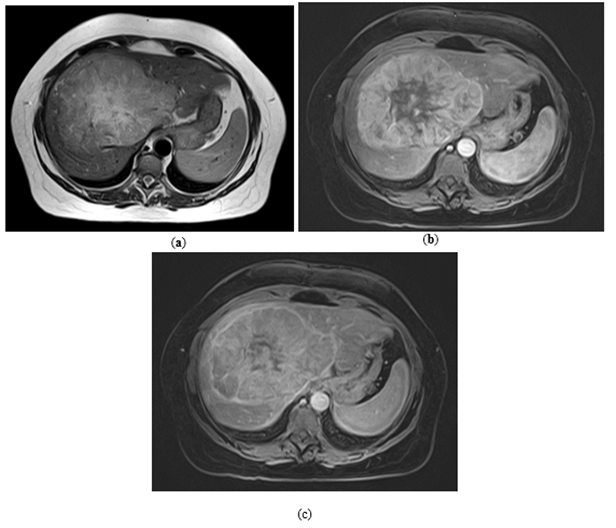
Figure 3: Pre-operative MR imaging Patient 3: (a) T2 TSE sequence depicting central scar; (b) T1 sequence with fat saturation in depicting intense early arterial enhancement; (c) Late venous phase imaging showing iso-/hyperintensity of solid components to healthy liver tissue.
We report on a series of three female patients with solitary liver tumors initially suspected to be FNH because of the arterial enhancement pattern and a supposedly central scar in a solitary tumor. All patients presented at our center for a second opinion and evaluation of further treatment with large tumors between 10 to 24 cm in diameter. None had cirrhosis or any underlying liver disease. A biopsy was not obtained in any of the three cases prior to surgery. According to the EASL Clinical Practice Guidelines on the management of benign liver tumors we would request an MRI with hepatotropic contrast agent to confirm the diagnosis of an FNH. [3] In two of the presented cases the patients were referred to our center with MRI conducted without hepatotropic contrast agent. After discussion in our interdisciplinary tumor conference with hepatobiliary surgeons, radiologists, and oncologists we indicated surgical exploration because HCC could not be ruled out. In these two cases we refrained from performing a Primovist-MRI. The surgery was performed by an experienced team of surgeons with special hepato-biliary expertise. For the classification of the resections, the “New World” terminology was used. [2] The histology revealed well to poor differentiated HCCs with an 8th edition TNM classification status varying from pT1 to pT2 [4]. One patient developed recurrence and metastatic disease and deceased in the course of time. The postoperative follow-up was performed every three months for a minimum of two years after resection. At least every six months. (Table 1)
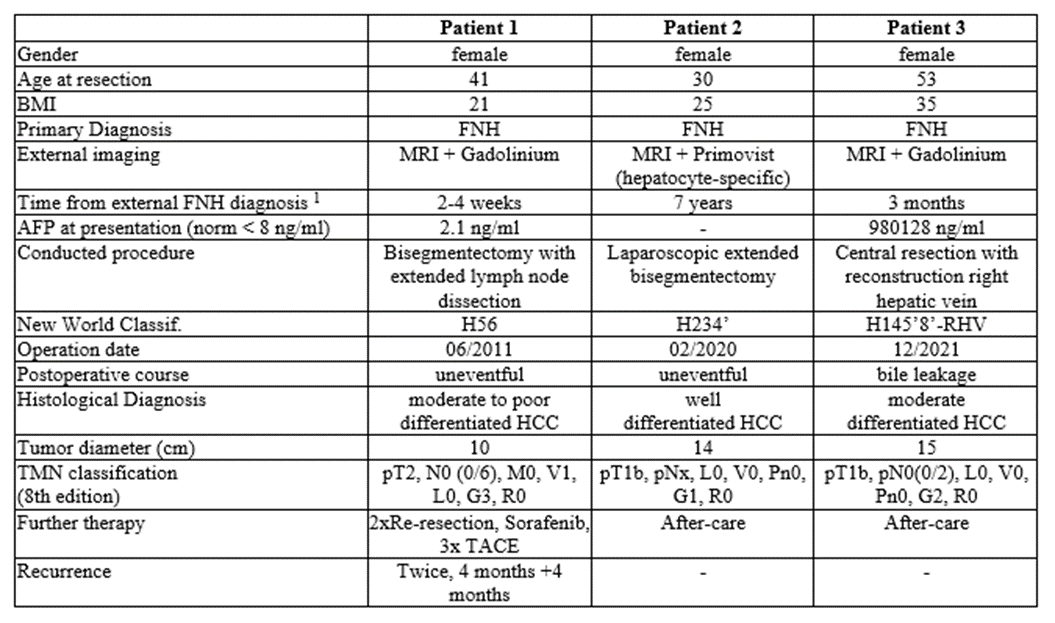
Table 1: The patient characteristics. The respective data from the three patients were collected at our center in an institutional database.
1 time period from external FNH diagnosis until presentation at our center
2 d.o.d.: died of disease
3 n.e.d.: no evidence of disease
FNH is the second most common benign liver lesion with no evidence of malignant transformation. [5, 6] The incidence has a female predominance with ratios ranging from 8:1 to 12:1.[7] The majority of FNHs are asymptomatic and found incidentally.[1] The main patient group are young females at the age of 20 to 50 years. Sporadic cases of male patients with a FNH have been described.[8] The lesions tend to grow slowly or show no growth at all. In asymptomatic patients FNH treatment is not necessary, but a reliable diagnosis is crucial. [3] We performed a comprehensive search in Pubmed to find comparable cases or case series. The findings were scarce. Langrehr and colleagues reported in 2006 a retrospective analysis of 77 patients who underwent liver resection for FNH and found two HCC (2,5%) in final histology. [9] More recently Jung and colleagues published an analysis of 48 patients who underwent biopsy after imaging diagnosis of FNH with detection of one HCC (2,1%) after histological analysis.[10] The specific features in CT- and MRI-scans often lead to the diagnosis of FNH. Presentation of the imaging to a radiologist with specific hepatobiliary expertise should be considered. The EASL Clinical Practice Guidelines on the management of benign liver tumours suggests the use of MRI with hepatotropic contrast agent to be the more sensitive imaging modality to diagnose FNH compared to a multi-phase CT-scan.[11] In our case series, only one of the three patients underwent MRI with hepatotropic contrast media. If an MRI with a hepatotropic contrast agent does not lead to a safe diagnosis, an additional contrast enhanced ultrasound is advised. Even though FNH tends to show a distinct pattern in imaging modalities, HCC can mimic a benign lesion as shown. For example, about 20% of HCC display an uptake of contrast agent in late phases.[12] But in contrast to HCC, a FNH does not show any washout appearance.[13] In CT-scans FNH show a distinct morphology with a central vascular supply.[14] In MRI it is iso- or hypointense in T1 and hyper- or isotense in T2-weighted imaging and shows a T2w-hyperintense central element/scar which enhances on delayed-phase imaging when extracellular contrast agents are used. [15] The central scar is found only in about 30-50% of FNH in MR-imaging and in literature not correlated with the size of the lesion.[16] Furthermore, in about 50% of HCC in non-cirrhotic livers a central scar is also present.[11] It appears that in larger lesions the prominent central scar with radiating fibrous septa can be less distinct due to the general mass of the lesion. Whether this observation should lead to even greater attention to the diagnostic and differential diagnosis of FNH of large lesions, is to be discussed. [17] When there are still doubts, a biopsy is recommended to secure the diagnosis. The general issue with biopsies is the concern for needle track seeding or missing malignant parts. Another problem is the difficulty to differentiate FNH-tissue from well-differentiated HCC or fibrolamellar HCC in a biopsy sample.[18] So even with a histology ruling out malignant cells in the biopsy, uncertainty remains. One of our patients had an extremely high level of AFP preoperative with explicit decrease after resection. In patient 2 the AFP unfortunately was not measured prior to the resection. An increased level of AFP is usually associated with HCC and it used widely for screening in high-risk patients and for HCC follow-ups.[19,20] AFP can be increased slightly (up to 100 ng/ml) in liver cirrhosis and in chronic hepatitis as well,[21] but also in pregnancy or teratoma.[22] AFP is typically not elevated in a FNH but some rare cases with elevated AFP in FNH have been reported in a range of 40 – 60 ng/ml.[23, 24] One assumes that in these cases AFP expression is caused by a regenerative process due to features of progenitor cells within the FNH or even in the non-lesional adjacent liver.[25] Measurement of AFP levels in every newly diagnosed liver lesion is highly recommended. A high AFP level or an increase over a short period of time would be suspicious for HCC. The numbers of resections for benign liver tumors have risen in recent years due to various reasons including a broader access to imaging modalities and the emergence of minimal invasive surgery, but generally an over-therapy via surgery should be avoided. .[26] If the diagnosis is certain and the tumor is asymptomatic then there is no indication for surgery. On contrast, if there are any indeterminate features in MRI, CT-scan, and ultrasound with respective contrast agents, or a notable elevation of AFP levels or a measurable tumor growth surgery should be offered to the patient.[19] Otherwise, a close follow-up with imaging and AFP-level control should be performed.
Hepatocellular carcinoma (HCC) can resemble focal nodular hyperplasia (FNH), potentially delaying essential treatment. FNH is a benign liver tumor that, if asymptomatic, typically does not require surgical intervention. A contrast-enhanced MRI scan is often sufficient for diagnosing FNH, and alpha-fetoprotein (AFP) levels usually remain normal. However, cases showing an increase in size, elevated AFP levels, or a further rise in AFP warrant concern. Seeking a second opinion from a hepato-biliary surgery center with experience in HCC and FNH, involving both radiologists and surgeons, is advisable. It is crucial to avoid overtreatment through surgery and to conduct follow-up examinations for newly diagnosed FNH, including AFP measurement, to monitor any changes.
To assist in the management of newly diagnosed FNH, we have developed an algorithm that offers a comprehensive approach to diagnosis, surveillance, and potential surgical interventions (refer to Figure 4).
Figure 4: diagnostic algorithm and recommendation.
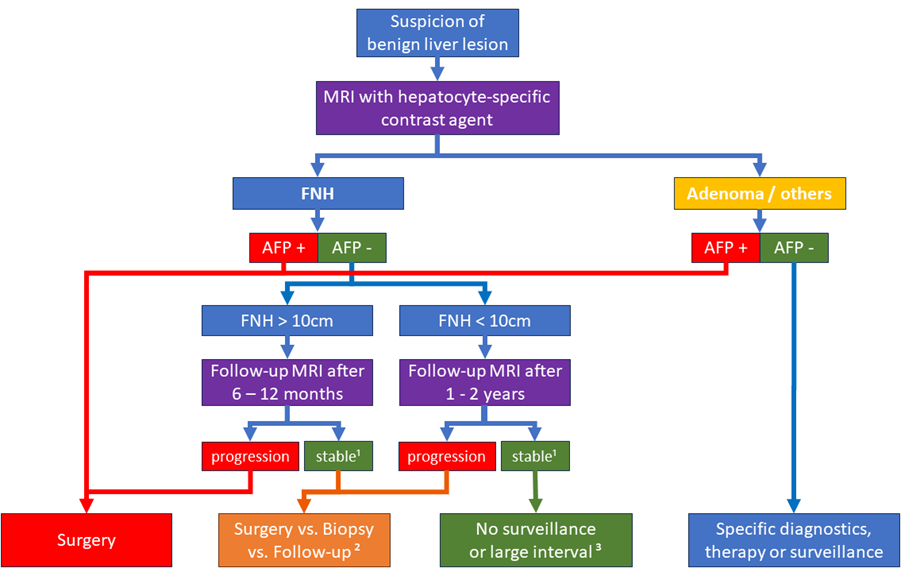
Figure 4: Flow chart of the diagnostic algorithm.
Algorithm designed to give an overview of our recommendation for surveillance and surgery. Key factors for indication for surgery are highlighted in red. This algorithm can only serve as an aid and does not assure perfect accuracy for any instance. Every patient must be studied, discussed, and advised individually.
1 stable or regression in size.
2 The further approach should be discussed in detail with the patient considering all risks and chances.
3 In these cases no surveillance is necessary. Nevertheless, an-other follow-up MRI can be performed after five years, for example. The patient’s safety need must be considered and justifies even shorter intervals.
The abstract was presented as poster presentation at EWALT Conference 2023 in Mainz. Otherwise, no publishing of the abstract or article.
This research received no external funding.
The authors have no conflict of interests related to this publication.
Conceptualization, Lisa-Katharina Gröger and Fabian Bartsch; methodology, Fabian Bartsch; ra-diological analysis, Felix Hahn; validation, Hauke Lang; formal analysis, Lisa-Katharina Gröger; investigation, Lisa-Katharina Gröger; resources, Lisa-Katharina Gröger and Beate K. Straub; data curation, Lisa-Katharina Gröger; writing—original draft preparation, Lisa-Katharina Gröger; writing—review and editing, Fabian Bartsch and Felix Hahn; visualization, Lisa-Katharina Gröger; supervision, Hauke Lang; project administration, Hauke Lang. All authors have read and agreed to the published version of the manuscript.
This study is in accordance with the regulations of the federal state law (state hospital laws §36 and §37, Rhineland-Palatinate), and no ethical approval was necessary for this study according to the independent ethics committee of Rhineland-Palatinate. An informed consent form has been signed by all patients that data and follow-up would be collected anonymously and potentially used for scientific analysis.
This publication deals with a case series. Data availability does not apply accordingly. In case of queries contact the corresponding authors.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
