
Research Article | DOI: https://doi.org/10.31579/2639-4162/062
1 Laboratory Service, National Hospital Center of Nouakchott, Mauritania.
2 Faculty of Medicine of Nouakchott, Mauritania.
*Corresponding Author: Mohamed Lemine Ould SALEM, Laboratory Service, National Hospital Center of Nouakchott, Mauritania.
Citation: Mohamed Lemine Ould SALEM, Ahmedna Sidi Abdalla, Ghaber Sidi Mohamed (2022). Hepatitis B and Delta Co-Infection: Prevalence and Serological Characteristics in Mauritania. J. General Medicine and Clinical Practice. 5(1); DOI:10.31579/2639-4162/062
Copyright: © 2022 Mohamed Lemine Ould SALEM, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 17 May 2022 | Accepted: 26 May 2022 | Published: 31 May 2022
Keywords: HBV; HDV; co-infection; nouakchott; mauritania
Background: Hepatitis B is one of the major public health concerns worldwide. In Mauritania, its prevalence in the general population is very high. The hepatitis D virus (HDV) borrows the envelope from the hepatitis B virus (HBV) during its infectious cycle. We thus observe co-infections during which the two viruses are acquired simultaneously and superinfections by HDV in patients who are already chronic carriers of the B virus.
Objective: to assess the prevalence of HBV and HDV infection
Material and Methods: this is a prospective descriptive study, conducted from January 1 to November 30, 2017 in the two medical analysis laboratories in Nouakchott. Patients were included: all patients of both sexes and of all ages carrying HBsAg presenting to the two medical analysis laboratories during this period.
Results: in 12 month, 211 patients with HBsAg were notified out of a total of 1675 patients screened, i.e. a prevalence of 12.59%. HBV/HDV co-infection is 31.30%. The average age was 36 years with extremes [8 and 66]. The male/female sex ratio was 1.45. The mean HBV viral load was 2.68 ± 1.31 log IU/ml [range: 478.63 IU/ml ± 20.41]. The majority (94.9%) of patients were HBeAg negative.
Conclusion: HBV/HDV co-infection remains very high in our country. This study indicates that the significant morbidity of the two viruses associated with limited knowledge of the mode of transmission, constitute factors of vulnerability.
Hepatitis B virus (HBV) infection remains a national and global public health problem. A ubiquitous disease, according to the World Health Organization (WHO), two billion people worldwide are infected with the hepatitis B virus (HBV), of which 370 to 400 million are chronic carriers of the HBs antigen [1]. Of these, 15 to 25% will die prematurely from a hepatic complication, mainly cirrhosis or hepatocellular carcinoma [1-3]. In Africa the infection is endemic, an estimated 65 million chronic carriers of HBV [2].
In Mauritania, few epidemiological studies are available but it is estimated that the overall prevalence of HBsAg is greater than 10.7% [5-7]. Under the natural conditions of infection, HDV only spreads in the presence of the hepatitis B virus from which it borrows the envelope. We thus observe co-infections during which the two viruses are acquired simultaneously and superinfections by HDV in patients who are already chronic carriers of the B virus [8]. About a quarter of chronic carriers of HBsAg are co-infected with the hepatitis D virus [2, 9-12]. In developing countries, most HBV and HDV infections occur during the perinatal period (vertical transmission) in more than 90% of cases [13,14]. To our knowledge, data on the prevalence of HBV/HDV coinfection in Mauritania are rare. Therefore, it is relevant to know the prevalence of HDV in chronic carriers of HBsAg in two medical analysis laboratories in Nouakchott. This would allow us to know the impact of HBV/HDV coinfection in our context and to propose a preventive and curative strategy.
Patients and Methods:
This is a prospective, single-center observational study on the prevalence of VHD in chronic HBsAg carriers at the two medical analysis laboratories (Maurilab medical analysis laboratory and Medilab medical analysis laboratory) during the study period from January 1 to November 30, 2017.
Included in this study were all patients carrying HBsAg screened in the two medical analysis laboratories during the study period. Data collection was carried out using a previously tested questionnaire. They focused on socio-demographic attributes and medical data (age, sex, origin, reason for hospitalization, previous treatment, physical and biological signs, evolution and complications). The search for anti-HDV AC was carried out in all HBsAg positive patients. An additional assessment (hepatitis B viral load, HBeAg, anti-HBe AC, anti-HBc AC, ALT, AFP) was performed in our patients.
Data analysis was performed using SPSS Statistic 20 software.
Limitation of the study:
Absence of HDV viral load data and imaging data
During the 12-month period, 211 cases were collected, or an average of 17 cases per month. These 211 cases represented 14.96% of all screened during the same period (1410 screened)
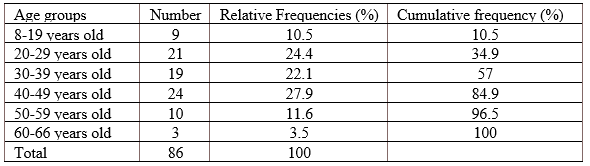
The average age of the patients was 36.3 ± 12.5 years with extremes of 8 and 66 years and years and the most affected age groups were as follows: 40-49 years (27.9% of cases), 20-29 years (24.41% of cases). The distribution of patients according to age groups is shown in Table 1
The M/F sex-ratio was 1.45 but the majority of the infection concerned men (125/211 or 59.2%).
The search for AC-anti-hepatitis Delta virus (AC HDV) was performed in all of our patients and was positive in 66 cases (31.30%) (Table 2).

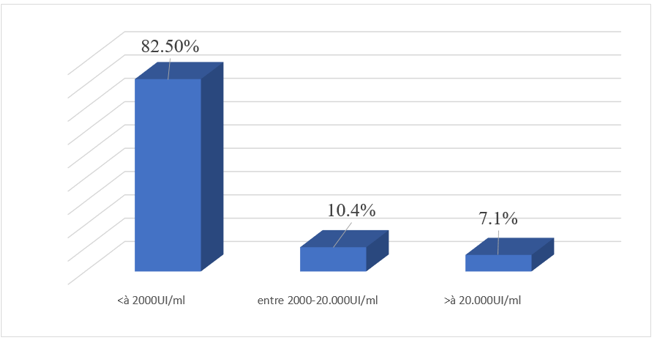
Quantitative measurement of viral DNA allowed us to individualize three groups of patients, 82.5% of them have a low viral load below 2000 IU/ml, 7.1% of patients have HBV DNA high above 20,000 IU/ml and 10.4% have an intermediate viral load between 2000 and 20,000 IU/ml.
The distribution of patients according to HBV viral load is shown in Figure 1.
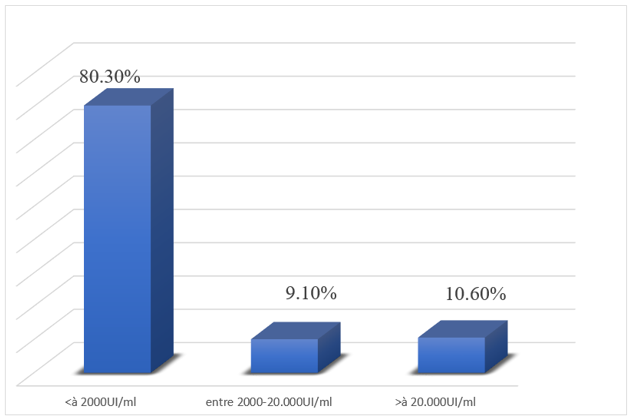
3.6. Distribution of co-infected patients according to HBV viral load:
Among the 66 AC HDV positive patients, 53 patients (80.3% of patients) had a viral load below 2000 IU/ml, 6 patients (9.1%) had an intermediate viral load between 2000 and 20,000 IU/ml. ml and 7 patients (10.6%) have a high viral load above 20,000 IU/ml. Figure 2 shows the distribution of co-infected patients according to HBV viral load.
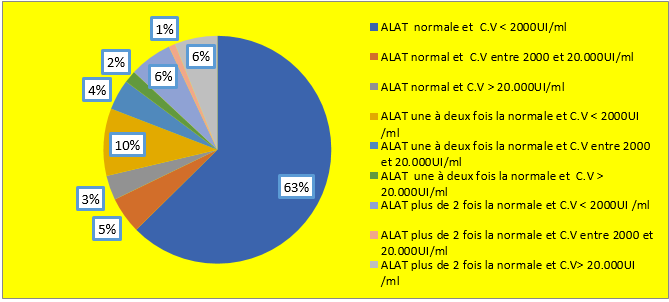
3.7. Distribution of patients according to ALT level and HBV viral load:
- 63% of patients had a normal ALT level and a viral load below 2000IU/ml;
-5% of patients had a normal ALT level and an intermediate load of between 2000 and 20,000IU/ml;
-3% of patients had a normal ALT level and a viral load above 20,000IU/ml;
-10% of patients had an ALT level one to two times normal and a viral load below 2000IU/ml;
-4% of patients had an ALT level one to twice normal and an intermediate viral load between 2000 and 20,000IU/ml;
-2% of patients had an ALT level one to two times normal and a viral load greater than 20,000IU/ml;
-6% of patients had an ALT level more than twice normal and a viral load below 2000IU/ml;
-1% of patients had an ALT level more than twice normal and an intermediate viral load between 2000 and 20,000IU/ml;
-6% of patients had an ALT level more than twice normal and a viral load greater than 20,000UI/ml.
Figure 3 shows the distribution of patients according to ALT level and HBV viral load.
3.8. Distribution of co-infected patients according to ALT level:
- 63.04% of patients had a normal ALT level;
-19.56% of patients had an ALT level one to two times normal;
-17.4% of patients had an ALT level more than twice normal.
3.9. Distribution of patients according to HBe status:
Out of 97 patients among the 211 HBV carriers, 92 HBeAg (-) patients (i.e. 94.9% of patients) and 5 patients (i.e. 5.1%) HBeAg (+) were found (table 3).

3.10. Relationship of HBe seroconversion and HBV viral load:
Among the 92 HBeAg negative patients, 78 patients (i.e. 84.8%) have a viral load below 2000 IU/ml, 7 patients (i.e. 7.6%) have an intermediate viral load between 2000 and 20,000 IU/ml, and 7 patients (7.6%) have a high viral load above 20,000 IU/ml.
Among the 5 HBeAg positive patients, 2 patients had an intermediate viral load between 2000 and 20,000 IU/ml and 3 patients had a high viral load greater than 20,000 IU/ml (Table 4).

3.11. Relationship of HBe seroconversion and co-infection:
Among the 92 HBeAg negative patients, 29 have positive HDV AC and among the 5 HBeAg positive patients 3 have positive HDV AC.
3.12. Distribution of patients according to alpha-fetoprotein level and HBV viral load:
- 76.47% of patients had a normal AFP level and a viral load below 2000IU/ml;
-211.76% of patients had a normal AFP level and a viral load between 2000-20,000IU/ml;
-5.86% of patients had a high AFP level (380 ng/ml) and a viral load below 2000 IU/ml;
- 5.86% of patients had a high AFP level (28493ng/ml) and a viral load above 20,000IU/ml.
Chronic HBV/HDV co-infection is most often the cause of serious liver damage such as fulminant hepatitis, if compared to HBV mono-infection.
HBV/HDV superinfection is associated with chronic infection in 90% of virus carriers and rapidly progressing to cirrhosis and increased risk of hepatocellular carcinoma [11,12].
HBV and HDV co-infections are generally characterized by strong HDV replication with the coexistence of very weak HBV replication, which would be due to repression of B virus replication by Delta proteins [17].
In addition, concurrent infection with HDV complicates antiviral treatment, as HBV treatment regimens do not affect HDV replication [2]. The only treatment that has shown efficacy in chronic D infection is interferon-α. Stopping treatment at doses of 2.5 to 7.5 MU/m2 , 3 times a week for 2 to 16 weeks, is associated almost constantly with a relapse, which recommends that the dosage currently proposed is therefore 9 MU, 3 times a week for 48 weeks. At these dosages, side effects are numerous and can limit the feasibility of treatment [16].
4.1. Epidemiology:
4.1.1. Gender:
A significantly higher prevalence of HBsAg was observed in men. This could be a consequence of better shedding of infection by females, but there is currently no clear explanation for this higher rate of HBV infection in males although some behavioral aspects (e.g., the shaving, travel) may play a role [18].
In our study population of 211 patients with HBsAg, the breakdown by sex shows a male predominance with a frequency of 59.2% for men (n=125) and a frequency of 40.8% for women (n=86), i.e. a sex ratio of 1.45.
The male predominance is more evident in all studies carried out nationally and internationally.
In Mauritania, in a study of 300 patients chronically infected with HBV receiving care at the hepato-gastroenterology unit of the National Hospital of Nouakchott (CHN) between February and October 2009, reports a male predominance with a sex ratio 1.52 (184 M/116F) [19].
Among blood donors (DDS) carrying HBsAg in Mauritania, a male predominance with a sex ratio of 27 (431M/16F) [5].
In Morocco, a study carried out on 276 patients carrying HBsAg also showed a male predominance with a sex ratio M/F of 1.51 [20].
In Tunisia there is also a male predominance with a sex ratio of 1.02 [14].
The male predominance was also described in a study carried out in 2008 on 75 patients with HBV residing in northeastern Algeria with a sex ratio of 1.77 (48M/27F) [21].
In Cameroon, a study was carried out in the Gastroenterology Unit of the Yaoundé University Hospital Center, the Yaoundé General Hospital and the Cathedral Medical Center, from August 2012 to May 2013 on 128 patients chronically infected with HBV notes a male predominance of which 77 (60.16%) were men and 51 (39.84%) were women [22].
In Nigeria of 188 HBsAg positive serum specimens from outpatients recruited from four tertiary hospitals in southwestern Nigeria, 82 (43.6%) were female and 106 (56.4%) male [12].
Epidemiological data in France also show a predominant male representation of 51% [23].
4.1.2. Age:
The average age of our patients is 36 years old with extremes of 8 and 66 years old and the most represented age groups are 40-49 years old (27.90%) followed by 20-29 years old (24.41%) with no significant difference between the two sexes (p=0.5).
The young age of our patients could be explained by the fact that most patients are infected with hepatitis B at a young age (newborns: mother-child transmission which seems to play an important role in the maintenance of the virus in our country, grandchildren…); the complications that could constitute the reason for consultation generally appear late, and the screening of children is rarely carried out.
The young age of Mauritanian patients is also found in the Mauritanian studies cited above; Lunel-Fabiani F et al [19] found an average age of 36 years in patients chronically infected with HBV receiving care at the hepato-gastroenterology unit of the National Hospital of Nouakchott; Mansour W et al [7] also described an average age of 36 years among consulting patients, while Mansour W et al [5] found an average age of 31 years among blood donors; a lower age (26 years) has been described by Mansour W et al [7] in pregnant women.
Our results concerning age were compared with those of African countries: The average age of Algerian patients is similar to that of our patients, 35 years [21], 39 years in Moroccans [20], 28 years in Tunisians [14], 33 years among Cameroonians [22] and 32 years among Nigerians [12]. The average age of our patients is consistent with that found in France, 36 years [23].
In our series, the mean age in AC HDV positive patients is 37.2 ± 12.3 and in AC HDV negative patients is 35.4 ± 12.4 with a non-significant difference (p=0. 8), which is consistent with the results from Cameroon (p>0.05) [22] and the results from Tunisia, the mean age in AC HDV positive patients is 43 years and in AC HDV negative patients is aged 41 with a non-significant difference (p=0.12) [14].
However, these results are not consistent with the results obtained in blood donors in Mauritania, which shows that the average age was significantly higher in AC HDV positive donors compared to AC HDV negative donors (34.28 years ± 9.18 against 30.52 years ± 8.63, P = 0.001)[5] and are not consistent with the results of patients chronically infected with HBV followed at the National Hospital Center of Nouakchott (CHN) which shows that AC HDV positive patients were significantly older than AC HDV negative patients (41 ± 12 versus 33 ± 11 years, p < 0>
The mean age of HDV positive subjects was approximately five years older than that of the general HBsAg positive population in the different cohorts studied in Mauritania (p<0>
4.1.3. Prevalence of HBV/HDV co-infection:
In our series, the prevalence of HBV/HDV co-infection is 31.30%.
In Mauritania, according to a study carried out from July 2008 to July 2009 involving 1020 pregnant women and 946 consulting patients, CA HDV was found in 19% of HBs+ Ag consultants and in 14.7% of HBs+ Ag pregnant women [7].
In Mauritania, a study was conducted from October 2008 to December 2009 on 11,000 blood donors, 1,700 of whom were HBsAg positive, 90 donors were found to be AC HDV positive (ie 19.78% of patients) [5]. AC HDV was also sought in the 300 patients followed at the CHN and 98 (33.3%) were found to be AC HDV positive [19].
In Tunisia out of 1615 HBsAg positive patients, only 33 patients (i.e. 2%) had positive HDV AC [14].
In Algeria, the prevalence of HBV/HDV co-infection is 1.28% (1/78) [24].
In Senegal, the prevalence of CA HDV among asymptomatic HBsAg-positive subjects ranged from 4% in the north to 13% in Dakar and 44% in Pikine [25].
In Cameroon out of 128 patients chronically infected with HBV, 29 patients had positive HDV AC representing 22.66% [22].
In Nigeria, HDV AC was found in 12.5% of 96 HBsAg+ patients [26].
In 2009, an HDV CA rate of 66.7% was reported in Gabon [27].
Our results concerning the prevalence of HBV/HDV co-infection were compared with those of Western countries:
In France, among a total of 4492 DDS positive for HBsAg, 89 (1.98%) were AC HDV positive [10].
The seroprevalence of patients co-infected with HBV and HDV in Belgium is 5.5% (44/800) [28].
In Italy out of 488 subjects who tested positive for HBsAg, 24 were AC HDV positive (4.9%) [11].
The prevalence of HBV/HDV co-infection in the United States is 8% [29].
In Iran, the prevalence of HBV/HDV co-infection is 2.2% [9].
Overall, the prevalence of co-infection in our series is comparable to that of African countries but much higher than that described in developed countries (Europe and the United States).
Table 5 compares the prevalence of co-infection between our series and data from the literature

4.2. HBV viral load:
In our series, the quantification of the mean HBV viral load calculated is 2.68 ± 1.31 log IU/ml (i.e. 478.63 IU/ml ± 20.41). This quantitative measurement of viral DNA allowed us to individualize our patients into three groups; 82.5% of them have a low viral load of less than 2000 IU/ml; 7.1% have a high viral load greater than 20,000 IU/ml and 10.4% have an intermediate viral load between 2000 and 20,000 IU/ml. These results are comparable with the results found in DDS by Mansour W et al. [5] who showed that the average viral load was 2.0 ± 1.65 log IU/ml (i.e. 100 ± 44.7 IU/ml) and 7.9% of patients had an intermediate viral load between 2000 and 20,000 IU/ml/ and 9.8% were above 20,000 IU/ml.
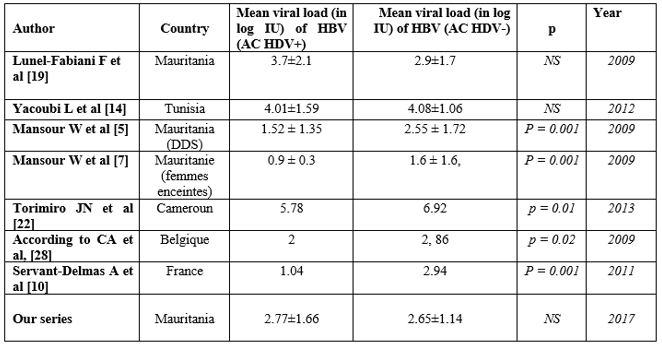
In our series, the HBV viral load was not significantly different between AC HDV positive patients and AC HDV negative patients (2.77±1.66 versus
2.65±1.14, p=0.8), Meaning that Delta virus infection did not decrease HBV replication; this finding is consistent with the results found by Mansour W et al [7] in outpatients and those found by Yacoubi L et al [14] (Tunisia) which showed that the viral load of HBV was not significantly different in patients AC HDV Positive versus AC HDV Negative patients (4.08±1.06 vs 4.01±1.59, p=0.79).
On the other hand, the results found by Mansour W et al [5] in DDS showed that the viral load of HBV was significantly higher in DDS AC HDV negative than in DDS AC HDV positive (2.55 ± 1.72 vs. 1.52 ± 1.35, P = 0.001), as well as in pregnant women where the HBV viral load was significantly higher in AC HDV negative pregnant women than in AC HDV positive pregnant women (1.6 ± 1. 6 versus 0.9 ± 0.3, p = 0.001) [7].
In Belgium and France, the viral load of hepatitis B was significantly higher in patients mono-infected with HBV compared to co-infected patients with a significant difference respectively: p=0.02, p=0.001 [28 ,10].
The comparison of the HBV viral load of mono-infected patients to co-infected patients in our series with data from the literature is shown in Table 6.
In Cameroon, patients with a low viral load < 2000> 20,000 IU/ml represented 17.19% and the hepatitis B viral load was significantly higher
(p=0.01) in mono-infected patients (8383192UI/ml or 6.92 log) than in co-infected patients. infected (608813UI/ml or 5.78 log) [22].
The comparison of HBV viral load in mono-infected patients between our series and literature data is shown in Table 7.

Overall, co-infected patients have a lower B viral load than those co-infected with the Delta virus. Indeed, it is classic to note that infection with the hepatitis D virus inhibits the replication of the hepatitis B virus. This inhibition was studied by WU et al [30] who showed that the co-transfection of HBV DNA with HDV cDNA reduced by a factor of 10 the expression of the majority HBV RNAs (3.5 and 2.1 Kb). This action seems to be linked to the small HD protein (195 amino acids). Indeed, the co-transfection of the same cells with HBV DNA and an expression plasmid coding for the small HD protein also decreases the expression of the majority HBV RNAs.
HDV infection does not appear to decrease HBV replication in our study. The fact that a significant proportion of patients mono-infected with HBV were inactive carriers of HBV (62.6% having normal ALT levels and 82.5% having a low viral load below 2000 IU/ml) could be an explanation.
Note that the contagiousness of patients is proportional to their viral loads, whether acute or chronic infection.
4.3. HBe status:
Out of 97 patients among the 211 HBV carriers, 92 HBeAg (-) patients (i.e. 94.9% of patients) and 5 HBeAg (+) patients (i.e. 5.1%) were found. This is close to the results of Lunel - Fabiani F [19] who showed that 7.2% of patients were HBeAg (+) and 92.8% of patients were HBeAg (-).
In Cameroon 14/128 (i.e. 10.94%) of patients have HBeAg (+), and 114/128 (i.e. 89.06%) have HBeAg (-) [22].
In Tunisia nearly 95% of patients were AgHBe (-) [14].
In our series, HBe status is strongly correlated with HBV viral load (p=0.00). All HBeAg positive patients (5 patients) had a viral load ≥ 2000 IU/ml, of which 2 patients had an intermediate viral load between 2000 and 20,000 IU/ml and 3 patients had a high viral load greater than 20,000 IU/ml. In fact, HBeAg, alongside DNA, is a marker of viral replication.
Among the 92 HBeAg (-) patients, 7 patients (i.e. 7.6%) have an intermediate viral load between 2000 and 20,000 IU/ml, and 7 patients (i.e. 7.6%) have a high viral load greater than 20,000 IU/ml which could be explained by the circulation of mutant strains (pre-core mutants) in our country.
In Cameroon, all HBe Ag (+) patients had HBV DNA levels above 20,000 IU/ml while 7 patients (i.e. 6.14%) had HBV DNA levels above 20,000 IU/ml in Cameroon. HBe Ag (-) patients [22].
In our series, we noticed that co-infection has no influence on HBe status (p=0.22), which is consistent with the study by Torimiro JN et al [22] in Cameroon (p= 0.43).
4.4. Other biological parameters:
These parameters are very little studied in the literature that we consulted.
In our series, the ALT level was not significantly different between AC HDV positive patients and AC HDV negative patients (p = 0.27). was found in 13.04% of mono-infected patients and 17.39% of co-infected patients, which is comparable to the results of Yacoubi L et al [14] (Tunisia) which showed that the ALT level did not was not significantly different from AC HDV positive patients compared to AC HDV negative patients (p = 0.5) and also comparable to the results of Keshvari M et al [9] (Iran) which showed that the ALT level was not not significantly different from AC HDV positive patients compared to AC HDV negative patients (p=0.3).
On the other hand, in the study by Lunel-Fabiani F et al [19], AC HDV positive patients had higher ALT levels with a significant difference (p<0>
In Belgium, the ALT level more than twice the normal is found in 13.66% of patients mono-infected with HBV, 34.48% of co-infected patients and co-infected patients had values of ALAT significantly higher (p=0.002) [28].
In our series, the ALT level was significantly higher in patients with a high viral load (p=0.00), as was the AFP level (p=0.01).
This marker of cytolysis seems to be increased by Delta co-infection according to most authors, contrary to what we observed in this study.
In our series, there is no significant difference in AFP (p=0.3) in co-infected patients compared to mono-infected patients.
This prospective study carried out on 211 patients carrying HBsAg aimed to study the prevalence of HBV and HDV co-infection, the influence of co-infection on the B viral load, the relationship between HBe seroconversion and the viral HBV and the influence of HBV/HDV co-infection on HBe seroconversion, as well as the study of other biological parameters (ALAT, PT, platelets, bilirubin, AFP).
Regarding HBsAg carriage, our study shows a male predominance with a sex ratio of 1.45. It confirms the high prevalence of HBV/HDV co-infection in our country (31.3%).
The average age of our patients was 36 years old and the most affected age group is 40-49 years old (27.90%) followed by 20-29 years old (24.41%) with no significant difference between the 2 sexes.
The average HBV viral load in our series was 2.68 ± 1.31 log IU/ml (i.e. 478.63 IU/ml ± 20.41), 10.4% of our patients had an intermediate viral load between 2000 and 20,000 IU/ml and 7.1% of the patients had a high viral load above 20,000 IU/ml and there is no significant difference between the viral load of AC HDV positive patients and AC HDV negative patients.
In our series, HBe status is strongly correlated with HBV viral load and all HBe Ag (+) patients had a viral load greater than 2000 IU/ml. However, no relationship has been established between HBe status and HBV/HDV co-infection.
ALT and AFP levels were not significantly not different from co-infected patients compared to mono-infected patients.
HBV/HDV superinfection is associated with rapid progression to cirrhosis and an increased risk of hepatocellular carcinoma, which prompted us to make this
Study which is very limited by the number of staff and the absence of imaging or pathology data that could demonstrate complications of hepatitis B virus infection or HBV / HDV coinfection, the burden viral Delta could not also be carried out, it shows a high prevalence of co-infection by the delta virus in carriers of the hepatitis B virus, which is alarming in our context where the prevalence of hepatitis B is very high.
Conflict of interest: none
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
