
Review Article | DOI: https://doi.org/10.31579/2690-1897/166
*Corresponding Author: Rehan Haider, Riggs pharmaceutical Department of Pharmacy University of Karachi Pakistan.
Citation: Rehan Haider. (2023), Hemorrhoids the Clinical Practice, J, Surgical Case Reports and Images 6(6); DOI:10.31579/2690-1897/166
Copyright: © 2023, Rehan Haider. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 October 2023 | Accepted: 24 October 2023 | Published: 29 October 2023
Keywords: hemorrhoids; piles; anal canal; swollen; inflamed; vascular structures; etiology; intra-abdominal pressure; constipation; pregnancy; rectal bleeding; anal itching; pain; prolapse; internal hemorrhoids; external hemorrhoids; anoscopy; sigmoidoscopy
Hemorrhoids, commonly referred to as piles, constitute an everyday medical condition characterized by swollen and inflamed vascular systems in the anal canal. This discomfort is a source of pain for numerous individuals worldwide, affecting their satisfaction with their lives. The etiology of hemorrhoids encompasses various factors, including improved intra-stomach stress, persistent constipation, extended sitting, and pregnancy. In addition to being frequently benign, hemorrhoids can cause signs and symptoms including rectal bleeding, anal itching, pain, and prolapse.
This summary explores the modern-day understanding of hemorrhoids, emphasizing their classification into internal and external types, based on their anatomical location and signs. Inner hemorrhoids originate above the dentate line and are typically painless. However, they can also cause bleeding and prolapse. Outside hemorrhoids located under the dentate line can be painful and thrombosed. Diagnostic approaches embody scientific record evaluation, bodily examination, and every so often anoscopy or sigmoidoscopy to exclude more serious conditions.
The management of hemorrhoids consists of lifestyle modifications along with elevated dietary fiber consumption, hydration, and normal exercise to relieve constipation and decrease intra-abdominal stress. Topical treatments consisting of corticosteroids and over-the-counter ointments offer relief from signs and symptoms. For refractory cases, minimally invasive procedures such as rubber band ligation, sclerotherapy, and infrared coagulation offer powerful solutions. Surgical interventions, such as hemorrhoidectomy, are reserved for severe instances or when other treatments are ineffective.
Symptoms related to hemorrhoids are very common in Western and other industrialized societies. Although published estimates of prevalence range widely, hundreds of thousands of humans in the United States of America are affected annually [1-3], and the range of affected people who encounter this illness seems to be decreasing. Among gastrointestinal problems, hemorrhoids are identified in outpatients as frequently as diverticular sickness and are more effective than gastroesophageal reflux disorder, stomach wall herniation, and functional intestinal issues [4]. The most common complications of hemorrhoids are heavy bleeding, continual unremitting prolapse of mucosal tissue, strangulation, ulceration, and thrombosis.
Hemorrhoids are collections of submucosal, fibrovascular, and arteriovenous sinusoids, which are part of the regular anorectum [5].The reason for those “vascular cushions” is incompletely understood; however, they appear to be critical for sensing fullness and stress and for perceiving anal contents. similarly, they'll assist anal closure, facilitate continence, and assist in protecting the anal sphincter from injury during defecation [6]. Hemorrhoidal complexes are typically amassed inside the left lateral, anterolateral, and posterolateral areas of the anal canal, but may be found in other places.
Hemorrhoids were labeled as consistent with their beginning relative to the dentate line. which is typically positioned about 3–4 cm proximal to the anal verge. the line represents the website where the squamous epithelial cells are derived from the ectoderm interface with the columnar mucosa cells of the endodermal starting place. except being the foundation for categorizing Hemorrhoidal complexes as inner (if proximal to the dentate line), outside (if distal to the dentate line), or mixed (each proximal and distal), the specific embryonic origins result in exceedingly exceptional vascular drainages, epithelialization, and innervation (Fig. 1 and a couple of others). Tissues that are distal to the dentate line are innervated using somatic nerves and are more sensitive to pain and irritation than those that might be located extra-proximally, which results in sympathetic or parasympathetic visceral innervation. However, it is unclear why hemorrhoids are symptomatic. In an Austrian observational observation concerning adults who underwent routine screening colonoscopy, about 39% had visibly enlarged Hemorrhoidal complexes; however, about half of the contributors with anatomical abnormalities have been symptomatic [7]. Potential causes of signs and symptoms range from weakening of supportive tissues with prolapse of the cushions to atypical dilatation of arteriovenous anastomoses and Hemorrhoidal venous complexes. [8,9], nine With the onset of slippage, the venous return can be similarly compromised. primary to additional swelling and cyclical tissue harm. sufferers with symptomatic hemorrhoids might also have expanded anal resting pressures and improved tone, although the meaning of this However, these findings remain uncertain [10]. The risk of symptomatic disorder is multiplied
Among people with an extended venous strain and changed venous drainage (due to cirrhosis) with ascites, pregnancy, common straining, or extended standing or squatting), strange bowel function (diarrhea or constipation), collagen vascular abnormalities, clinically large pelvic floor dysfunction, or a low intake of nutritional fiber, and among those who are obese or sedentary [11-13]. although it has been suggested that the ingestion of spicy foods exacerbates hemorrhoid symptoms.During a brief period, a randomized trial confirmed no worsening of signs and symptoms in people with hemorrhoids who ingested crimson-hot chili pepper [14].
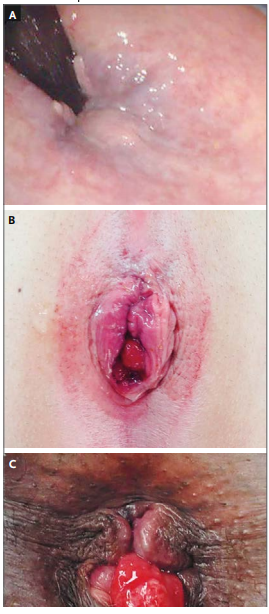
Figure 1. Hemorrhoidal Disease
Panel A shows a sigmoidoscopic retroflexed view of grade 1 hemorrhoids; the flexible sigmoidoscope is visible in the upper left. Panel B shows grade II to III hemorrhoids with a small external component. Panel C shows grade IV internal hemorrhoids with external components. Photographs courtesy of Dr. Aakash Gajjar, Department of Surgery, University of Texas Medical Branch at Galveston.
Evaluation and prognosis
The scientific manifestations of symptomatic hemorrhoids vary with the severity of the ailment. Patients who gift for prognosis and remedy typically report hematochezia (approximately 60%), itching (approximately 55%), perianal discomfort (approximately 20%), soiling (approximately 10%), or a few aggregates of these signs. Rectal bleeding commonly occurs in such patients. With or Once After Defecation. Blood may. be noticed on restroom paper, in bathroom water, or, from time to time, staining the underclothes.7 Patients must. be queried about fiber and fluid consumption, bowel styles (including stool frequency), restroom conduct (e.g., reading while seated on the toilet), the need for virtual manipulation of prolapsed tissue, and whether there may be a record of soiling or incontinence. Therefore, other disorders should also be considered.A sizeable ache is uncommon in patients with straightforward internal or external hemorrhoids. The. presence of extreme aches increases the possibility of other situations, consisting of anal fissure, peri rectal or provoking infection, abscess, and different inflammatory approaches, even though severe pain may additionally occur with hemorrhoid complications (e.g., prolapse with incarceration, ischemia, or thrombosis). Bleeding, inflammation, or pain can also arise in patients with perianal dermatitis, colorectal cancers, inflammatory bowel disease, diverticular disorder, angiodysplasia, anal warts, anal polyps, or rectal ulceration.8 cautious examination of the anus and the encircling pelvic regions is vital for accurate prognosis. The inclined jackknife position (where. The lateral decubitus position can also provide adequate visualization for sufferers who have physical boundaries. exam inside the lithotomy This is also an important function. Inspection may additionally display an anal fissure in patients who report intense pain and bleeding during defecation. A virtual rectal exam should be performed if viable. Many sufferers with symptomatic hemorrhoids have reducible venous congestion that distorts the Ordinary anorectal architecture. Those with more superior ailments might also have friability of the pores and skin overlying the venous complexes, proof of spoilage or seepage, and inflammation of the surrounding tissues. Any abnormalities discovered within the absence of Hemorrhoidal venous dilatation need to raise difficulties using different ailment methods. complete-thickness protrusion of rectal tissue with eversion and evidence of concentric mucosal folds is a feature of rectal prolapse; the prognosis of this disorder can be facilitated by asking the affected person to perform a Valsalva maneuver even as seated. All abnormalities should be defined in keeping with their location relative to the dentate line (anterior or posterior, left or proper, and proximity to everyday anatomical systems) as a substitute, relative to their role on the clock face.
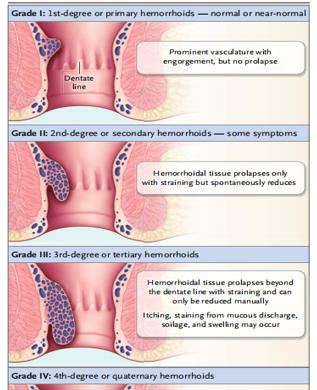
Anoscopy can detect more than 99% of anorectal illnesses and must be performed on any patient suspected of having hemorrhoids [15] The standard grading system for hemorrhoids must be used (Fig. 2). [16,17]. However, this device no longer contains other findings that can impact scientific choice-making, including size, presence or absence of soreness that notably impairs sports of daily living or severity of bleeding. Laboratory trying out isn't always important for sufferers with uncomplicated disease
Imaging and Endoscopy
Flexible endoscopy is not as successful as anoscopy for examining the anorectum.15 Rigid procotoscopy, even though it is used less typically now than previously, also allows for the visualization of structures close to the dentate line. The selection to carry out an extra tremendous colorectal evaluation has to be knowledgeable using the patient’s age, imparting signs and symptoms and their duration, and the character of bleeding. evaluation of the entire colon is indicated for patients with any of the subsequent: anemia; bleeding that isn't normal for hemorrhoids; a change in bowel styles; private records of rectal or colon polyps; my family records of inflammatory bowel ailment, colorectal cancer, or different hereditary colorectal diseases in a first-degree relative; or other suspected pathologic pelvic changes that could make contributions to the affected person’s symptoms. although sigmoidoscopy can be reasonable as a preliminary method in low-hazard sufferers with hematochezia, double-assessment barium enema, or colonoscopy is indicated in sufferers in whom the presentation or circle of relatives records raises the subject approximately proximal ailment; a colonoscopy is favored by way of many clinicians [18,19].
For symptomatic sufferers younger than 50 years of age who've no threat elements for colonic disease and no proof of other anorectal abnormalities and in whom examination confirms In the presence of clear-cut sickness, hemorrhoid remedy may be administered instead of endoscopy or imaging research. chronic bleeding or different signs and symptoms after a successful nearby treatment for hemorrhoids is a sign of similar evaluation.
Medical therapy
All sufferers should be advised to ingest a sufficient amount of insoluble fiber (typically 25 to 35 g per step per day) and water to avoid constipation and straining and to restrict the time spent on the toilet. A meta-analysis of controlled trials. showed that fiber supplementation was related to significant discounts in the chance of continual signs and the risk of rectal bleeding, even though the outcomes of fiber supplementation on mucosal prolapse, ache, and itching were no longer widespread [20]. Medical revel indicates that the use of topical glucocorticoids, vasoconstrictors (e.g.,
phenylephrine-primarily based creams or suppositories), or analgesics may also provide the temporary remedy of a few signs, however, statistics from randomized trials on long-term efficacy and facet results are lacking. Conservative approaches were initially recommended for patients with low-grade ailments. Such procedures are also desired for most patients who are pregnant, debilitated, or promised, sufferers with coagulation issues, and sufferers with Crohn’s disorder or conditions that confer a predisposition to negative recovery.
office-primarily based therapies and other Procedures Several options are available for patients with grade I to III disorders that do not respond to conservative medical management. The number one goal of office-based total strategies which are less expensive than excisional therapies, is to decrease the amount of redundant tissue, lessen Vascularity, and affix the Hemorrhoidal cushions to the rectal wall. five before such processes are achieved, it is important to inform sufferers approximately any external components to be able to not be addressed with the aid of the procedure — for instance, residual skin or skin tags so that it will no longer be excised or anal contouring is a good way to not be restored [21].
Rubber-Band Ligation, Sclerotherapy, and Infrared
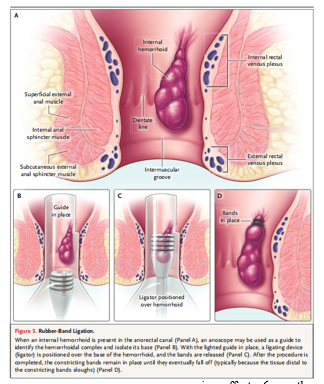
Coagulation Rubber-band ligation includes figuring out a Hemorrhoidal complicated, using forceps or suction to increase the cushions, and putting one or greater rubber bands across the base of every cushion while taking care to avoid impinging the muscle tissue (Fig. 3). The farther away the bands are from the dentate line, the lower the chance of severe pain [22.23]. Ligation of the complex eventually necroses the trapped connective tissue, and the scar is affixed to the rectal wall. No bowel practice other than simple enemas is usually recommended, and the method is most customarily finished without sedation. Narcotic analgesics are not frequently required in a while, but sufferers who have extra than two sites banded in any given consultation were much more likely to have extended discomfort. If more than one session is required, there's normally a c Language of at least 6 weeks between sessions to allow sufficient recovery to occur. Rubber-band ligation is suitable for patients with grade I or II disorders and some otherwise wholesome patients with grade III sickness who are amenable to in-office remedy and whose disorder is amenable to less invasive intervention. difficulty fees range from three to 8%,19, [24,25], with complications which include pain, urinary retention, delayed hemorrhage, Hemorrhoidal thrombosis distal to the band, and localized contamination. Systemic contamination is an unprecedented but critical hassle that needs to be taken into consideration in any affected person in whom fever develops. Sclerotherapy includes submucosal injections, which can be repeated over the years. The injections. causes local thrombosis and fibrosis, and decreases Vascularity. Sclerotherapy is the best treatment for grade I or II disorders. Post procedural bleeding is unusual because there may be no eschar creation; for that reason, this process should be taken into consideration for sufferers who have a multiplied bleeding risk, together with those receiving anticoagulants. The foremost complications are iatrogenic because they are out-of-place injections. A meta-analysis of 18 randomized trials comparing diverse remedy techniques for grades I to III hemorrhoids concluded that rubber-band ligation become more effective than sclerotherapy and that patients who underwent ligation were less likely to want the next remedy: Rubber-band ligation changed into something much less powerful than hemorrhoidectomy, however, had fewer complications and prompted less ache.26 It, therefore, is considered suitable as first-line therapy. The pronounced rate of lengthy-time period success of rubber-band ligation (with a lengthy-time period described as at least 6 months) is about 90% among sufferers with Hemorrhoidal ailments of less than grade IV, such as the 20% of patients who require repeat tactics.27 Sclerotherapy induces lengthy-time period remission in the handiest a 1/3 of sufferers. Infrared light carried out on a website proximal to the Hemorrhoidal complex induces coagulation necrosis and, in the end, scarring in patients with low-grade sickness. Case studies and randomized trials recommend that the recurrence price is appreciably higher with infrared coagulation than with rubber-band ligation, however, the former has fewer headaches and causes much less pain at once after the manner.2, [26,28].
Thrombectomy of External Hemorrhoid
Thrombectomy of external hemorrhoids is regularly performed in patients with grade III or IV disease. Sufferers with severe pain on account of a clot that presents within 72 hours after the onset of pain may advantage from incision and evacuation of the clot or excision of the entire Hemorrhoidal complicated, completed at the same time as the patient is below neighborhood anesthesia [29], Excision is not encouraged while patients gift more than 72 hours after the onset of pain because the pain associated with thrombosis usually resolves without intervention after 7 to 10 days. effective, but painful [30,31], Additional inner Hemorrhoidal tissue can also be eliminated through cautery. bipolar diathermy, ultrasonography, and unique techniques. Hemorrhoidectomy with electricity-primarily-based absolute devices may also motivate a whole lot less pain postoperatively than traditional excisional hemorrhoidectomy [32,33]. Stapled hemorrhoidectomy, a more modern technique for the treatment of patients with grade III or IV internal disease, includes using a
circular stapler to resect rectal mucosal tissue, interrupt the arterial and venous flow, and simultaneously affix the remaining tissue in situ above the dentate line. This gadget no longer particularly copes with any outside disorder manifestations. unusual however extreme headaches together with pelvic sepsis, rectal urgency, recto vaginal fistulization, and rectal structuring were described [34,35]. A evaluation of randomized trials assessing effects 6 months or more after stapled hemorrhoidopexy finished with the resource of professional surgeons showed a notable decrease recurrence fee and reduce the rate of Hemorrhoidal prolapse after hemorrhoidectomy in evaluation with the charges with conventional hemorrhoidectomy, but prices of bleeding, ache, or itching did not range substantially among the two techniques (table 1) [36]
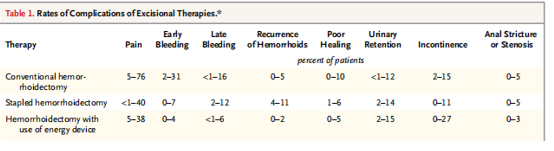
Data, reported by De la Garza and Counihan,36 are from randomized, controlled trials or meta-analyses. The duration of follow-up varied but was generally at least 6 months. Pain was defined as a requirement for ongoing analgesic medication 5 days after the procedure. Early bleeding was defined as bleeding that occurred 48 hours or less after the procedure, and late bleeding as bleeding that occurred more than 48 hours after the procedure.
Areas of Uncertainty
Bioflavonoids, which possess strong antioxidant activity in vitro, may lower infection. are administered orally to treat Hemorrhoidal signs and symptoms in a few international locations, although they have not been approved for this use in the United States. A meta-analysis of randomized trials suggests that treatment with those sellers may reduce signs and the danger of recurrence; however, the quality of the pains analyzed turned into being taken into consideration to be poor [37]. Extra observations are wanted concerning the efficacy of Doppler-guided ligation of Hemorrhoidal arteries as a non excisional treatment for sufferers with prolapsing hemorrhoids. further information is also needed to guide the peri procedural care of patients taking anticoagulants.
Guidelines
The requirements exercise venture force of the American Society of Colon and Rectal Surgeons [38], Italian Society of Colorectal Surgery,39 and the Scientific Practice Committee of the American Gastroenterological Association has published guidelines or a role statement for the treatment of Hemorrhoids. The suggestions in this evaluation are consistent with those statements.
The patient in the vignette had symptoms suggestive of hemorrhoids. The examination might be expected to reveal extra Hemorrhoidal tissue originating proximal to the dentate line and regular grade I or II sicknesses. Given the affected person’s age, a colonoscopy is warranted if it has no longer been performed. First, attention to bowel law and neighborhood hygiene is an appropriate technique. If clinical management is useless after 6 to eight weeks, the next remedy should be guided by the treating clinician’s knowledge and the patient’s choices. However, in-workplace rubber-band ligation might be an inexpensive subsequent step. Excisional treatments are commonly reserved for sufferers in whom rubber-band ligation fails and for those with grade IV sickness or headaches
The completion of this research project would not have been possible without the contributions and support of many individuals and organizations. We are deeply grateful to all those who played a role in the success of this project We would also like to thank My Mentor. Naweed Imam Syed Prof. Department of Cell Biology at the University of Calgary and Dr. Sadaf Ahmed Psychophysiology Lab University of Karachi for their invaluable input and support throughout the research. Their insights and expertise were instrumental in shaping the direction of this project
I at this moment declare that:
I have no pecuniary or other personal interest, direct or indirect, in any matter that raises or may raise a conflict with my duties as a manager of my office Management
The authors declare that they have no conflicts of interest.
Financial support and sponsorship
No Funding was received to assist with the preparation of this manuscript
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
