
Case Report | DOI: https://doi.org/10.31579/2641-0419/367
Hospital Fundacion Alcorcon, Madrid, Spain.
*Corresponding Author: Pablo González Alirangues MD, Hospital Fundacion Alcorcon, Madrid, Spain.
Citation: Pablo G. Alirangues, Carlos G. Jiménez, Elena E. Barrio, Javier B. Rodríguez, (2024), Hemodynamic features of chronic constrictive pericarditis and concomitant pleural disease: a case report, J Clinical Cardiology and Cardiovascular Interventions, 7(4); DOI: 10.31579/2641-0419/367
Copyright: © 2024, Pablo González Alirangues. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 April 2024 | Accepted: 14 May 2024 | Published: 24 May 2024
Keywords: chronic constrictive pericarditis; pericardial constriction; pleural disease; heart failure; right heart catheterization
Chronic constrictive pericarditis (CP) is an uncommon form of heart failure in which a thickened and often calcified pericardium limits diastolic filling, ultimately reducing cardiac pump performance. Diagnosis can be challenging and may require integrating clinical data with meticulous echocardiographic assessment and cross-sectional cardiac imaging. If non-invasive testing is inconclusive, right heart catheterization remains the gold standard diagnostic test. Classic hemodynamic features of constrictive pericarditis may also be seen in restrictive cardiomyopathy and are often insufficient to establish the diagnosis. Therefore, the preferred hemodynamic criteria of CP include the finding of increased ventricular interdependence and intrathoracic and intracardiac pressure dissociation. However, the presence of concomitant pleural disease may interfere with the catheterization hemodynamics and decrease the accuracy of these criteria as we present in this case report.
Chronic constrictive pericarditis is characterized by thickening, fusion, fibrosis, and calcification of the pericardial leaves, creating a rigid shell that surrounds the cardiac chambers causing restriction of cardiac filling. It is an uncommon entity whose treatment frequently requires pericardiectomy, a procedure associated with substantial morbidity and mortality. In the developed world, the most common causes of CP include prior cardiac surgery, thoracic irradiation, prior idiopathic pericarditis, connective tissue disease, malignancy and advanced renal disease (the first three being the most frequent etiologies) [1]. Recognizing this disease requires a high index of suspicion and a careful history and physical examination. Most cases are nowadays adequately diagnosed by cardiac imaging techniques, specifically 2D-echocardiography and Doppler evaluation often supplemented with cardiac magnetic resonance (CMR). Nevertheless, right heart catheterization continues to be the gold standard for the diagnosis of pericardial constriction and should be performed when the non-invasive findings are inconclusive. Classic diagnostic hemodynamic criteria include increased central venous pressure, near-equalization of right and left heart filling pressures, modest elevation in right ventricular systolic pressure and a right ventricular end-diastolic pressure that is at least one-third of the right ventricular systolic pressure. These criteria, however, have suboptimal sensitivity and specificity in the differential diagnosis with other conditions, especially restrictive cardiomyopathy [2]. Therefore, additional hemodynamic criteria, showing greater diagnostic accuracy, have been described based on the phenomena of intrathoracic and intracardiac pressure dissociation and increased ventricular interdependence [3, 4]. With this case report, we aim to show how concomitant pleural disease can decrease the clinical value of these preferred criteria and therefore should be taken into consideration when evaluating right catheterization findings in these patients.
A 54-year-old male presented to the emergency department with substernal chest pain and shortness of breath. Following clinical examination, chest X-ray, and echocardiogram evaluation he was diagnosed of effusive-constrictive pericarditis with concomitant bilateral pleural effusion in December 2020. An Echocardiogram showed mild pericardial effusion, paradoxical septal motion, and a dilated inferior vena cava with minimal inspiratory collapse. The pericardium was hyperechogenic and thick.
Treatment with non-steroidal anti-inflammatory drugs and colchicine was started as well as intravenous diuretics to alleviate systemic congestion. Due to a lack of adequate response, the patient was placed on 0.5 mg/kg of prednisone with marked improvement in laboratory and radiological parameters. A follow-up echocardiogram showed minimal pericardial effusion, 4-5mm around the right cavities, but persistent constriction signs.
Clinical evolution was unsatisfactory, with chest pain recurrence whenever steroid tapering was attempted. Sequential echocardiograms showed resolution of the pericardial effusion but persistent signs of constriction. In July 2021 a CMR exam was performed and revealed a 5 mm thickened pericardium. On follow-up chest X-ray, bilateral pleural effusion, predominantly on the right side, persisted (Figure 1). During these months, the patient presented several times to the Emergency Department due to chest pain recurrence, dyspnea, and general malaise
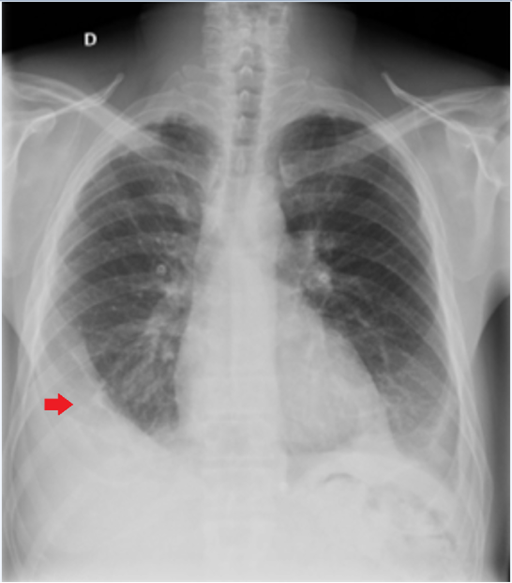
Figure 1: Chest X-ray showing chronic loculated right pleural effusion and secondary pulmonary atelectasis (red arrow).
Finally, due to persistent symptoms of chronic constrictive pericarditis refractory to medical treatment, surgical pericardiectomy was suggested.
Pre-operative coronary angiography was unremarkable. Pre-operative hemodynamics during right catheterization showed equalization of diastolic pressures in all cavities around 20 mmHg. Elevated right atrium pressure was observed, without respiratory variation and with a W morphology, although with an x wave greater than the y wave (Figures 2 and 3). Square root morphology was also observed in the left and right ventricular pressures and both chambers had equal diastolic pressures. The pulmonary arterial pressure was mildly elevated (37/19 mmHg). Left ventricular (LV) rapid filling wave >7mmHg was also observed. All these data supported the diagnosis of pericardial constriction.
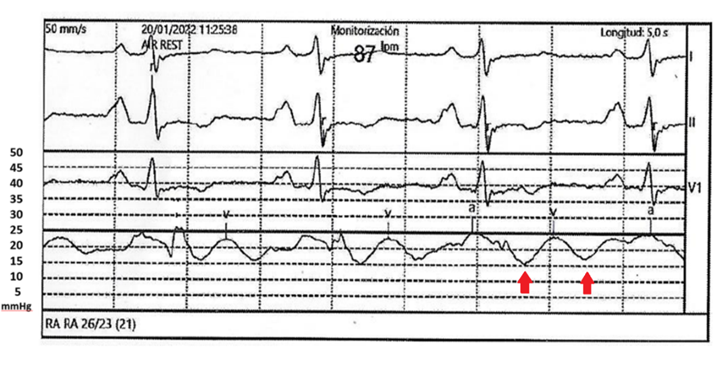
Figure 2: Right atrial tracing showing elevation of right atrial pressure. Note the increased x and y descents on RA tracing (red arrow).
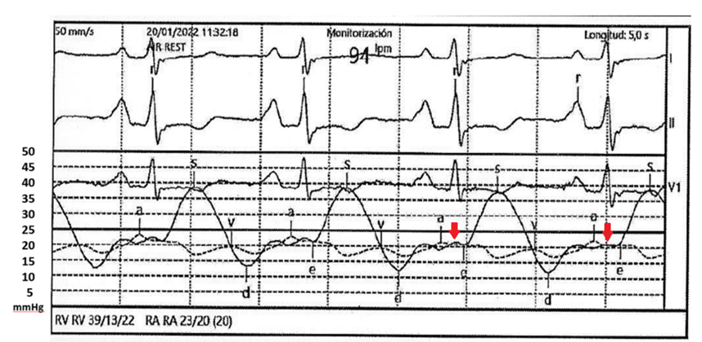
Figure 3: Right atrial (RA) and right ventricular (RV) tracings showing elevation in right filling pressures with equalization of end-diastolic pressures (red arrow).
Surprisingly however, there was no dissociation between intrathoracic and cardiac pressures or exaggeration of ventricular interdependence, as would be expected in a case of pericardial constriction (Figure 4). Intracavitary pressures did not vary with respiratory changes, a typical feature of constrictive pericarditis, but pulmonary capillary pressure (PCP) was also unaffected by respiration (Figure 5). Therefore, no variation in the PCP-LV gradient with respiration was observed, nor was there an exaggeration of ventricular interdependence.
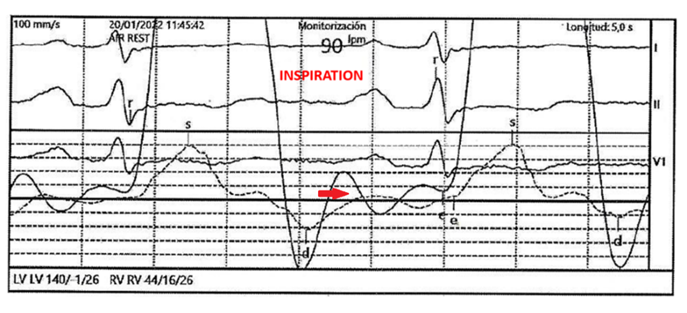
Figure 4: Left and right ventricles tracings showing equalization of end diastolic pressures. Left ventricular tracing show the square root or dip and plateau sign (red arrow). No evidence of increased ventricular interdependence was observed.
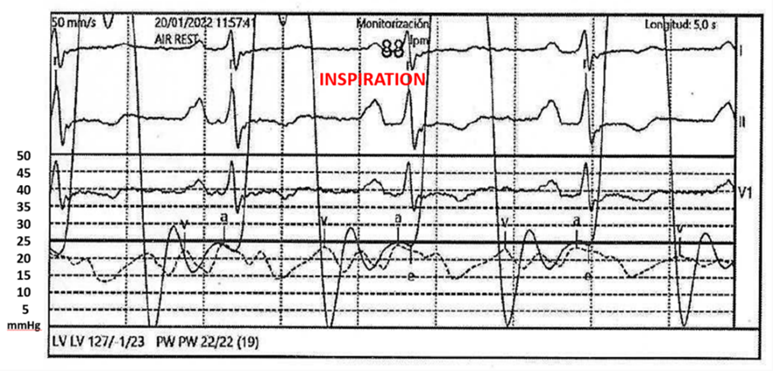
Figure 5: Simultaneous LV and pulmonary artery wedge pressure (PW) tracings. No reduction of the LV-PW diastolic gradient was observed.
Pre-operative CT scan showed a loculated pleural effusion, more severe on the right side, with linear uptake of the adjacent pleura with an inflammatory appearance and secondary pulmonary atelectasis. A diagnostic thoracentesis ruled out malignancy.
We hypothesized that the chronic right pleural effusion and secondary pulmonary atelectasis prevented the transmission of intrathoracic pressure changes during respiration to the right lung, where the Swan-Ganz catheter was placed to measure PCP.
The patient was referred to surgery and pericardiectomy was performed confirming the diagnosis of constrictive pericarditis. After surgery, the patient markedly improved and resolution of the ultrasound signs of pericardial constriction was observed.
Classic diagnostic hemodynamic criteria of pericardial constriction include elevation of central venous pressure; square root or dip and plateau sign, which translates the sudden increase in ventricular pressure after the early phase of rapid filling upon reaching the limit imposed by the constrictive pericardium; decrease in right atrial pressure of less than 5 mmHg with inspiration (equivalent to Kussmaul's sign); disproportionate elevation of end-diastolic pressure compared to RV systolic pressure and equalization of the end-diastolic pressures of both ventricles, with a pressure difference Less-than 5 mmHg (5).
All these classic criteria were present in our case. However, these criteria have been shown to have 60-90% sensitivity but only 40-60% specificity [3,6]. Additional hemodynamic criteria have been described based on the phenomenon of intrathoracic and intracardiac pressure dissociation and increased ventricular interdependence, showing greater accuracy for the differential diagnosis, with >90% sensitivity and > 80% specificity [4,7,8]. In constrictive pericarditis pressure in the pulmonary veins decreases during inspiration but remains unaltered in the LV because respiratory changes are not transmitted due to the thickened pericardium causing the dissociation of intrathoracic and intracardiac pressures. Left ventricular filling is consequently reduced allowing preferential filling of the right ventricle. In inspiration the right ventricle ejection volume is therefore larger than the LV volume, the opposite occurs during expiration, resulting in an exaggeration of the ventricular interdependence [9].
In our case, these two findings were not observed during right heart catheterization. In addition to pericardial constriction, our patient also had concomitant pleural pathology with chronic loculated right pleural effusion and secondary pulmonary atelectasis. PCP measurement was performed on the right pulmonary artery, ipsilateral to the effusion. We suspect the pleural pathology prevented the correct transmission of the inspiratory changes to the right lung, causing the lack of intrathoracic and intracardiac pressure dissociation and increased ventricular interdependence. However, since clinical suspicion was high, pericardiectomy was performed with intraoperative confirmation of the diagnosis of pericardial constriction and subsequent marked improvement of the patient's symptoms.
As we report in this case, pleural disease may alter the typical hemodynamic findings in patients with chronic constrictive pericarditis. Therefore, before performing right heart catheterization, it is important to assess the existence of pleural disease and we consider that a chest x-ray should be performed before catheterization to rule out pleural involvement. Regarding right heart catheterization, if pleural involvement is unilateral, PCP measurements should be performed in the pulmonary artery of the unaffected lung to minimize the influence of pleural pathology on the hemodynamic findings.
Chronic constrictive pericarditis diagnosis can be challenging and requires a careful medical history and physical examination supported by cardiac imaging techniques. If non-invasive testing is inconclusive, right heart catheterization remains the gold standard diagnostic test. Classic diagnostic hemodynamic criteria of pericardial constriction are useful for diagnosis but have suboptimal sensitivity and specificity and it is well established that newer hemodynamic criteria based on intrathoracic and intracardiac pressure dissociation and exaggerated ventricular interdependence confer greater accuracy for the diagnosis of constrictive pericarditis. However, as we report in this case, these criteria also have some limitations. The presence of severe concomitant pleural disease may interfere with the right catheterization hemodynamics altering the physiology and the findings and therefore should be considered when interpreting the hemodynamic study. Performing a chest x-ray before catheterization is useful to rule out pleural disease and to evaluate whether the involvement is unilateral or bilateral. If pleural involvement is unilateral PCP measurements should be performed whenever possible in the pulmonary artery on the unaffected side.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
