
Research Article | DOI: https://doi.org/10.31579/2692-9406/070
*Corresponding Author: Dr. Mohammed Ahmed Ibrahim Ahmed, Assistant professor of Microbilogy, Nile Valley University, Faculty of Medicine, Atbara, Sudan.
Citation: N K A Adam, N A M Abderahman, M A I Ahmed, I M A Eisa, Hala M Wardi, et al. (2021) Hematological Parameters in Sudanese Type-2 Diabetes Mellitus. Biomedical Research and Clinical Reviews. 4(3); DOI: 10.31579/2692-9406/070
Copyright: © 2021 Mohammed Ahmed Ibrahim Ahmed, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 07 June 2021 | Accepted: 16 July 2021 | Published: 21 July 2021
Keywords: hematological indices; type 2 diabetes mellitus; sudan
Background: Diabetes mellitus is a complex concept for a spectrum of disorders characterized by hyperglycemia and a variety of complications, comprising metabolic and cellular disturbances that lead to vascular complications. The objective of this project was to correlate type 2 diabetes patients to healthy controls in aspects of hematological indices and their association with demographic data.
Materials and Methods: From May to September 2016, a case-control analysis has been performed in Khartoum, Sudan. 154 participants were enrolled in this study. 104 participant were diabetic type 2 and 50 were apparently healthy as control group to find out any variations in hematological parameters HbA1C and CBC: (Hb, WBCs & differential, RBCs& indices and PLTs, hematocrit (HCT) among type 2 diabetic patients. Blood was gathered in EDTA containers. HbA1C measured using i-CHROMATM and complete blood count using the Sysmex® Kx21-N hematological analyzer. Before samples collection, each participant gave their informed consent, which had been approved by the Ministry of Health's ethical committee. The Statistical Package for Social Sciences (SPSS) SPSS version 20 was used. The meaning of the discrepancies was assessed using the Crosstab test. p- Value is significant at P< 0.05.
Results: T2DM patients had a statically significant in white blood cells, neutrophils, and lymphocytes as comparison to the control group P<0.05. There was no considerable difference in red blood cell count, Hb, Hct, MCV, MCH, MCHC, RDW, Platelets count, MPV, and PDW between the two classes P> 0.05.
Conclusion: T2DM patients had relatively increased levels of white blood cells, neutrophils, and lymphocytes than the control group (P<0.05).
Diabetes mellitus DM is a heterogeneous group of metabolic disorders characterized by hyperglycemia and a variety of implications, including metabolic and cellular complications that lead to micro and macro cardiovascular complications [1]. Type 2 diabetes mellitus is a long-term metabolic condition marked by elevated blood sugar, insulin resistance and/or deficiency [2]. Insulin resistance inhibits glucose release into liver and insulin dependent tissues, so, the liver releases glucose into the bloodstream in an inappropriate manner resulting in increased elevated plasma glucose or hyperglycemia which detected [3] by measuring of fasting plasma glucose level of 7.0 mmol/L (126 mg/dL) or more. Also two hours after a 75g oral glucose load plasma glucose at or above 11.1 mmol/L (200 mg/dL) is suggested as a glucose tolerance measure. Diabetes Association recommended criterion in 2010, defined hyperglycemia symptoms and blood glucose level of 11.1 mmol/L (200 mg/dL) or higher and HbA1C of 48 mmol/mol or higher (≥ 6.5 DCCT %) [4]. The American Type 2diabetes is regulated by lifestyle modifications and regular exercise [5].
T2DM prevalence rates have raised dramatically since 1960, synchronized with rising in BMI and obesity rates [6]. In 2013, approximately 368 million people were diagnosed with the disease, growing from about 30 million in 1985 [7].Type 2 diabetes is becoming more common in young adults, but it usually strikes in middle or later life [8].
HbA1C has glucose attached to terminal valine in each β chain by non-enzymatically reaction and occurs when plasma glucose is episodically elevated over time. The concentration of HbA1C depends on the concentration of glucose in the plasma and the duration of hyperglycemia and is an index of diabetic control for a period over past 12 weeks. High levels of glycated hemoglobin lead to hypertension and vascular diseases in diabetic patients because of impair endothelium mediated vasoactive responses [9]. Watala et al. attributed an increase in erythrocyte internal viscocity to glycation derived structural alterations in hemoglobin molecules [10].
Study design, period& population: From May to September 2016, a case-control evaluation was carried in the Khartoum state. The review investigated 154 participants; 104 of whom were diabetic patients in Jabir Abu Eliz Hospital patients and the other 50 were apparently healthy volunteers without a medical history of diseases enrolled as controls group to see if there was any variation in hematological parameters between groups.
Each subjects' blood samples were drawn in EDTA containers for full blood count evaluation using Sysmex® Kx21-N hematological analyzer or the direct current detection system with co-incidence correction was used to count WBCs, RBCs, and PLTs. Based on complex algorithms, automatic discriminators classify cell populations. The amplitude of each analyzed cell's electronic circuit is proportional to the cell volume. The hematocrit (HCT) is calculated directly from the red cell count and volume of each human RBC. The Sysmex® cell counters measure WBCs, RBCs, and PLTs with unrivaled precision and accuracy, even with samples at exceptionally low or extraordinarily high concentrations. Calculating of HbA1C using i-CHROMATM instrument is based onthe fluorescence immunoassay technology, specifically the competition immune-detection system.
Ethical approval, sampling &data interpretation:
This report was authorized by the Ministry of Health's ethics committee and each participant provided informed consent prior to sampling frame. Sample size determined depending in similar studies of Sudanese ethnicity. The Statistical Package for Social Sciences (SPSS) version 20 was used for statistical analysis. The meaning of the discrepancies was assessed using the Crosstab test. P< 0.05 was used to determine statistical significance.
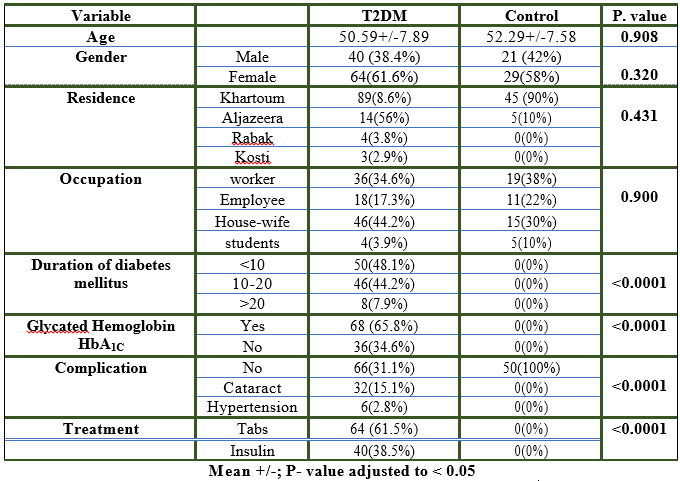
Demographic, clinical and characteristics of study participants:
In this study 104 participants were diabetic type 2 and 50 were enrolled as control group. In diabetic type 2 group 64 (61.6%) were females and 40 (38.4%) were males. For control group 29(58%) were females and 21 (42%) were males. The mean age was 50.59 years for diabetic type 2 group and 52.29 years for controls group (Table1). The duration of disease among diabetic type 2 was <10>20 years were 50(48.1%), 46(44.2%) and 8(7.9%) respectively. The resultsshowed that the mean levelof BMI, systolic and diastolic blood pressure and Hemoglobin A1C levels were significantly higher (P<0>
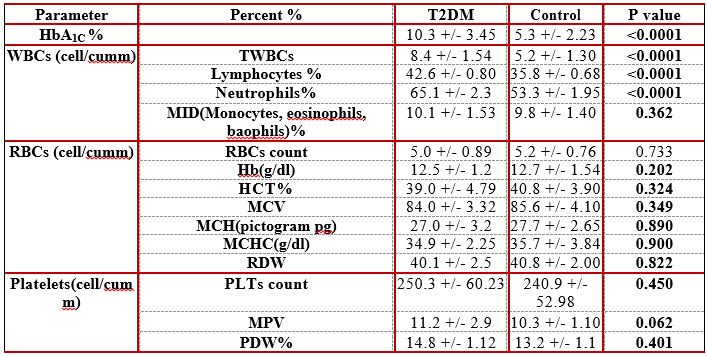
Comparison of hematological profile of study participants and control
The TWBCs mean were 8.4 Cumm in T2DM and 5.2 Cumm in control group. White cells mean were significantly higher in T2DM by (P=<0 xss=removed xss=removed>
Red blood cells count, Hb, Hct, MCV, MCH, MCHC, RDW, Platelets count, MPV and PDW showed insignificant change between two groups (P> 0.05).
There was association between some components of metabolic syndromes and leukocytes indicating association between total white blood cell count (WBC) and diabetes mellitus [11]. In this study the disparity in mean WBC count between diabetic patients and controls was statistically significant. This was consistent with findings of an Iraqi study2016 by [12]. Who noticed a substantial improvement in WBC count in diabetic patients as compared to the control group. Since the interaction between inflammatory, insulin, and human blood components formed a vital signal for disturbances caused by invading foreign agents or inflammation caused by these invaders, activation of the immune system and stimulation resulted in an increase in inflammatory symbols such as WBC and cytokines, As a result of the protection mechanism, blood parameters such as WBC, PCV, and phagocyte percentage can change [13].
Performed another study in Ethiopia in 2015 and realized the WBC indexes, statistically meaningful improvement in overall WBC (P=0.000), absolute neutrophil (P=0.012), and absolute lymphocyte (P=0.0001) counts were observed in the T2DM patients as compared to the control group. [21] Among RBC's indices. Their study is similar to our report in that there is a significant difference in white cells as compared to that of control. The platelet indices of diabetic and non-diabetic patients were also compared in this study. There was no statistically meaningful variation in platelet count between diabetic and control groups. The lack of a substantial difference (p<0>14].
The recent study showed diabetic patients with poor control of HbA1C and non-significant change in CBC. This finding was contradiction with that [15] which showed significant change in CBC indicating that the study participants were more susceptible to develop anemia.
T2DM patients had slightly higher levels of white blood cells, neutrophils, and lymphocytes than the control group (p<0>
CONFLICT OF INTEREST:
The author declares that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
LIST OF ABBREVIATIONS:
TWBCs: Total White Blood Cells Count;
RBCs: Red Blood Cells Count;
Hb: Hemoglobin;
Hct: Hematocrit;
MCV: Mean Corpuscular Volume;
MCH: Mean Corpuscular Hemoglobin;
MCHC: Mean Corpuscular Hemoglobin Concentration;
RDW: Red Cell Distribution Width;
MPV: Mean Platelets Volume;
PDW: Platelets Distribution Width.
AKNOWLEDGEMENTS:
We appreciate Jabir Abu Eliz Hospital patients' and team's collaboration during data collection for their kind treatment.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
