
case report | DOI: https://doi.org/10.31579/2690-4861/515
1Department of Internal Medicine, Atrium Health Wake Forest Baptist Medical Center, Winston-Salem, NC,
2Section of Cardiovascular Medicine, Atrium Health Wake Forest Baptist Medical Center, Winston Salem, NC,
3Novant Health, Heart & Vascular Institute, Bolivia, NC,
4Intermountain Medical Center, Section of Heart Failure, Transplant and Artificial Heart; Salt Lake City, UT.
*Corresponding Author: Nicole I. Cillis, D.O., M.P.H. 310 Chariot Square, Winston Salem, NC.
Citation: Nicole I. Cillis, Bridget M. Rasmussen, Abigail M. Thomas, Cassidy D. Vigil, Aysha Amjad, et al, (2024), Heart Transplant Rejection in the Setting of Glyphosate Herbicide Exposure; A Case Report., International Journal of Clinical Case Reports and Reviews, 19(3); DOI:10.31579/2690-4861/515
Copyright: © 2024, Nicole I. Cillis. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 06 August 2024 | Accepted: 26 September 2024 | Published: 29 October 2024
Keywords: heart transplant; transplant rejection; glyphosate; cardiotoxicity
Glyphosate is a common herbicide utilized worldwide with known exposure related toxicities. Numerous adverse effects related to glyphosate exposure have been documented, specifically in non-human models, however literature is lacking on cardiotoxic effects specific to heart transplant patients. Rejection is the most common post-transplant complication and the diagnosis of such is vital in order to guide immediate and appropriate treatment. In addition to the endomyocardial biopsy, noninvasive genetic testing can aid in rejection diagnosis and distinguish between cell-mediated and antibody-mediated rejection. We describe a case of glyphosate exposure in a post orthotopic heart transplant and the subsequent heart transplant rejection, patient’s clinical course, treatment, and follow up.
| dd-cfDNA : Donor derived cell free DNA | OHT : Orthotopic heart transplantation |
| DSA : Donor specific antibodies | RHC : Right heart catheterization |
| ECG : Electrocardiogram | RV : Right ventricle |
| GBH : Glyphosate-based herbicide | TAC : Tacrolimus |
| HLA : Human leukocyte antigen | TTE : Transthoracic echocardiogram |
| ISHLT : International Society for Heart and Lung Transplantation | TR : Tricuspid regurgitation |
| LVEF : Left ventricular ejection fraction | QT : QT wave interval |
| MMF : Mycophenolate mofetil |
Glyphosate is the most common herbicide in the world since the 1970s.[1] It is a non- selective, broad-spectrum herbicide that inhibits the 5-enolpyruvoylshikimate-3-phosphate synthase enzyme utilized in amino acid synthesis in plants, one vertebrate species lack.[1,2] The mixture containing glyphosate and the surfactant polyoxyethyleneamine is found in commercial herbicides such as RoundUpÔ, and associated with cytotoxic, genotoxic, and teratogenic effects.[3]
Although most literature on acute glyphosate-based herbicide (GBH) toxicity has focused on non-human models, acute human toxicity of glyphosate occurs.[4] Specific to cardiotoxicity, glyphosate in both non-human and human models has caused tachycardia or bradycardia, QT wave interval (QT) prolongation, and atrioventricular block.[1,5-7] However, data is limited on cardiotoxic effects in post heart transplants recipients. Here we describe a post orthotopic heart transplant recipient with accidental glyphosate exposure resulting in allograft dysfunction.
A 64-year-old man with chronic kidney disease, rheumatoid arthritis, and recurrent deep vein thromboembolisms presented with 10 days of cough, diarrhea, dyspnea, and weight gain following inadvertent toxin exposure. He had undergone orthotopic heart transplantation (OHT) two years prior for nonischemic cardiomyopathy, likely Plaquenil-mediated, withoutsubsequent rejections or development of post transplantation antibodies. At baseline, he had New York Heart Association class 1 symptoms and walked five miles daily. Immunosuppression medications included prednisone (due to coexistent rheumatoid arthritis), mycophenolate mofetil (MMF), and tacrolimus (TAC). A transthoracic echocardiogram (TTE) nine months prior showed normal allograft function and cardiac catheterization showed minimal intimal hyperplasia of the left anterior descending artery and 10% occlusion of the mid right coronary artery.
His inhalation exposure to RoundUp resulted in immediate mucosal irritation and subsequent diarrhea, abdominal pain, cough, six-pound weight gain, and sinus congestion. He presented nine days following exposure for a previously scheduledclinic visit with new dyspnea on exertion. TTE revealed a new reduction in right ventricle (RV) function with normal left ventricular ejection fraction (LVEF) 55-60%. Poison control was contacted, who recommended observation.
On admission, he was afebrile, heart rate 101 bpm, with blood pressure 128/96. Labs significant for B natriuretic peptide 648 pg/ml, creatinine 2.01 mg/dl (baseline 1.2), alkaline phosphatase 177 IU/L (prior 66), tacrolimus level 4.3 ng/ml (at target goal), and remaining labs were unchanged. Infectious workup negative for CMV-PCR, EBV IgM, Rocky Mountain spotted fever IgM/IgG, Lyme disease, and COVID. Presenting electrocardiogram (ECG) noted sinus tachycardia, low voltage, new axis right deviation, incomplete right bundle branch block and poor R wave progression (Figure 1) compared with prior ECG (Figure 2). Physical exam revealed jugular venous distention and peripheral pitting edema.
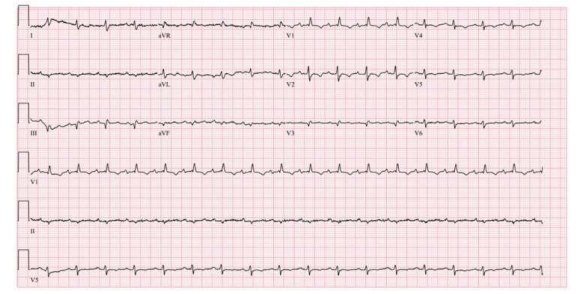
Figure 1: Presenting ECG: sinus tachycardia, incomplete right bundle branch block, low voltage QRS, poor R wave progression

Figure 2: Baseline ECG: sinus rhythm, incomplete right bundle branch block.
Transplant specific work up included elevated AlloSure Heart (cell-free DNA) at 3.5% (high: > 0.15%); elevated AlloMap (gene expression profiling) at 37 (high: >34 if > six months post-transplant). New class I and II donor specific antibodies (DSA) were identified on human leukocyte antigen (HLA) testing. Right heart catheterization (RHC) noted a right atrial pressure 16 mmHg, pulmonary artery pressure 34/18/23 mmHg, pulmonary capillary occlusive pressure of 16 mmHg with v-waves to 24, pulmonary artery saturation 61.5%, cardiac output and index by Fick 3.4 L/min and 1.7 L/min/m2. Endomyocardial biopsies noted mild acute cellular rejection with International Society for Heart and Lung Transplantation (ISHLT) grade 1R and negative C4d staining. Treatment included intravenous steroids, followed by a prednisone taper, an increase in MMF dose, and TAC continuation. He was discharged following 6L diuresis.
The patient was readmitted 2-weeks later due to tachycardia, a decline in LVEF to 35- 40%, and mild tricuspid regurgitation (TR). Repeat RHC demonstrated persistent elevated intracardiac filling pressures and reduced cardiac output. Readmission labs were similar to prior, AlloMap 39 but AlloSure Heart 0.84%. HLA testing negative for DSAs. Repeat endomyocardial biopsy was ISHLT grade 1R rejection. Pathology showed multifocal vacuolization and ballooning of myocytes concerning for ischemic injury. Coronary angiogram was unchanged.
Cardiac magnetic resonance imaging showed late gadolinium enhancement pattern suggestive of myopericarditis. Treatment included intravenous pulse-dose steroids and oral taper, administration of anti-thymocyte globulin (rabbit), with subsequent allergic reaction, causing a change to anti-thymocyte globulin (equine), increase MMF dose, continuation TAC (target trough 6-8), and intravenous diuresis. At outpatient follow up, repeat TTE noted improved LVEF of 50-55% with normal RV size, trace TR, mild mitral regurgitation, repeat AlloMap and AlloSure showed improvement at 29 and 0.51%, respectively, and RHC noted improved hemodynamics.
Heart transplantation is a common treatment for end-stage heart failure. Despite advanced immunosuppressive therapy, patients are subject to some degree of rejection, with most occurring in the first six months. After one year, the incidence of rejection significantly decreases.[8] In this case, new DSA, elevated cell free DNA, and gene expression profiling, with therapeutic FK level supported the hypothesis of GBH toxicity mediated heart transplant injury, which likely precipitated acute allograft rejection, and subsequent allograft dysfunction.
Cardiac manifestations of GBH toxicity include arrhythmias such as conduction blocks, bradycardia, and ventricular arrhythmia due to interference with calcium homeostasis.[4,5] The mechanism of toxicity is complex but felt to be largely cellular-mediated by surfactant interference that disrupts the mitochondrial wall proton gradient needed for energy production.[4] Oxidative stress and oxidative phosphorylation interruption secondary to GBH, plays a role in coronary artery disease when exposure-related oxidative stress over time induce cardiac subintimal inflammation.[9] Animal models found glyphosate increased myocardial contraction, while the surfactant in GBH decreased cardiac output, left ventricular stroke index, and mean arterial pressure.[10,11]
Heart transplant rejection can manifest as allograft failure with new heart failure, arrhythmias, or death. Invasive diagnosis is made with endomyocardial biopsy and microscopic examination. The ISHLT developed a standardized grading method to quantify rejection based on endomyocardial biopsy severity; 0R, 1R, 2R & 3R.[12] Cellular mediated rejection (CMR) is most commonly T-cell mediated and more common than antibody (B-cell) mediated rejection (AMR).[13] In AMR, antibodies can be DSA against human leukocyte antigen (HLA) class 1 or 2, non-DSA, or non-HLA. Together, both AlloMap and Allosure provide a noninvasive means to detect rejection/injury. AlloMap® Molecular Expression Testing assesses the gene expression profile of ribonucleic acid isolated from peripheral blood mononuclear cells. While AlloSure® Heart measures the amount of donor derived cell free DNA (dd-cfDNA) in the blood. A result >0.15
Here we present the first known case of GBH toxic exposuremediated heart transplant rejection. Our patient had prior OHT presented with symptomatic GBH exposure and clinical evidenceof impaired cardiacfunction with AMR, based on new DSA and a markedly elevated AlloSure. GBH cardiotoxicity is largely cell-mediated with oxidative stress manifesting in arrhythmias. Genetic testing can aid in noninvasive detection of rejection along with endomyocardial biopsy to confirm cellular and/or antibody mediated rejection leading to efficient and effective treatment.
The authors have no fundingto report.
The authorsof this manuscript have no conflicts of interest to disclose as described by the American Journal of Transplantation.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
