
Research Article | DOI: https://doi.org/10.31579/2642-9756/112
1 Wolaita zone health department, wolaita sodo, Ethiopia.
2 Assistance professor of obstetrics and gynecology in Wolkite University College of medicine and health sciences, Wolkite Ethiopia.
3 Anesthesia in Wolkite University College of medicine and health sciences, Wolkite Ethiopia.
4 Armauer Hansen ResearchInstitutee (AHRI), Addis Ababa, Ethiopia.
5 Assistance professor of surgery in Wolkite University College of medicine and health sciences.
6 Junior Project Manager, Active Citizenship Network, c/o Cittadinanzattiva APS, Via Cereate, 6 - 00183 Rome, Italy.
*Corresponding Author: Temesgen Tantu Arusi, Assistance professor of obstetrics and gynecology in Wolkite University College of medicine and health sciences, Wolkite Ethiopia.
Citation: Damene D. Hadaro., Temesgen Tantu, Muluken Gunta, Dereje Zewudu, et al (2022). Health Extension Postnatal Care Services Utilization and Associated Factors Among Mothers in Kindo Didaye District, Southern Ethiopia: a Community-Based Mixed-Method Study . J. Women Health Care and Issues. 5(3); DOI:10.31579/2642-9756/112
Copyright: © 2022 Temesgen Tantu Arusi, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 05 March 2022 | Accepted: 16 March 2022 | Published: 28 March 2022
Keywords: caregivers; non-communicable diseases (ncds); chronic patients; european union; patients’ rights; civic participation; patients’ advocacy groups (pags)
Background: Postnatal care is care provisions being delivered during postnatal period. Lack of care in this period may result in death or disability as well as missed opportunities to promote healthy behaviors affecting women, newborns, and children. We need to understand the level and factors affecting health extension postnatal care services utilization.
Objective: To determine the prevalence of health extension postnatal care services utilization and associated factors among mothers who gave birth in the last year in Kindo Didaye district, Southern Ethiopia, 2017.
Methodology: A community-based cross-sectional mixed-method study was conducted from March 1-30, 2017 to get the final sample size of 645 mothers. Descriptive statistics were used to describe study participants. Binary logistic regression was used to identify associated factors among the explanatory variables at P < 0.05.
Results: The prevalence of utilization of Post-natal care services is 32.8%. Having husbands attended secondary and above education, having at least one Antenatal care attendance, last delivery in the health institution, planning to utilize services, visitation, and notification of delivery by Health extension workers were factors to utilize services. The majority of Focus group discussion participants said that Health extension workers were not visiting at their homes and hence mothers might not be encouraged to attend health extension Post-natal care services. Conclusion: The prevalence of mothers who utilized health extension Post-natal care services in the district was very low. Thus, focusing on the identified factors could improve and sustain Post-natal care services from rural Health extension workers.
Postnatal care (PNC) refers to care provision given to a mother and the baby for a period of six weeks from the time of delivery. PNC is primarily comprised of physical examination, immunization, health education, and family planning services. The federal government of Ethiopia developed a health extension program which is meant to improve access and equity to preventive essential health intervention provided at kebele and HH level through a cadre of health extension workers (HEWs) who will provide basic curative and preventive health services in every rural community. [1-3] Worldwide, only 30% of the mothers are following PNC services. Analysis of demographic and health survey data from 23 Sub-Saharan African countries found that only 13% of women who delivered at home received PNC within 2 days of birth. Ethiopian demographic and health survey 2016 report indicated that 17% and 16.9% of mothers received PNC within 2 days after birth nationally and in Southern Nation respectively. [4-6, 17] Researches indicate that PNC services utilization is affected by several factors including maternal age, educational level of the women and their husband, occupational status of women and their husband, antenatal care attendance, place of delivery, mode of delivery and parity [5, 7-15] [18,19,20]. It has been estimated that if routine PNC and curative care in the postnatal period reached 90% of babies and their mothers, 10 to 27 percent of newborn deaths in Africa could be averted. In 2015, there were 2.7 million neonatal deaths globally. For too many babies, their day of birth is also their day of death. The maternal mortality rate is 19 times higher in developing countries than in developed, and children in developing countries are 8 times more likely to die before they reach five years. [4, 16].
Even though PNC services utilization plays a critical role in reducing maternal newborn mortality, little is known about the prevalence of utilization from HEWs and its determinants. Hence, if we are interested in ensuring that PNC services are used by the mothers, we need to understand the prevalence and factors affecting PNC services utilization that is critical for countries like Ethiopia with alarmingly high maternal and child mortality so that the programmatic interventions can be concentrated to increase the utilization rates.
Study setting and population
A community-based mixed method was employed among mothers who gave birth in the last year. Kindo Didaye district is located in Wolaita zone, SNNPR state, Ethiopia. The district is divided into 19 rural kebeles and 3 towns and has a projected total population of 123,348 according to the 2007 Ethiopian population and housing survey. The study was conducted from March 1-30, 2017
Sample Size Determination
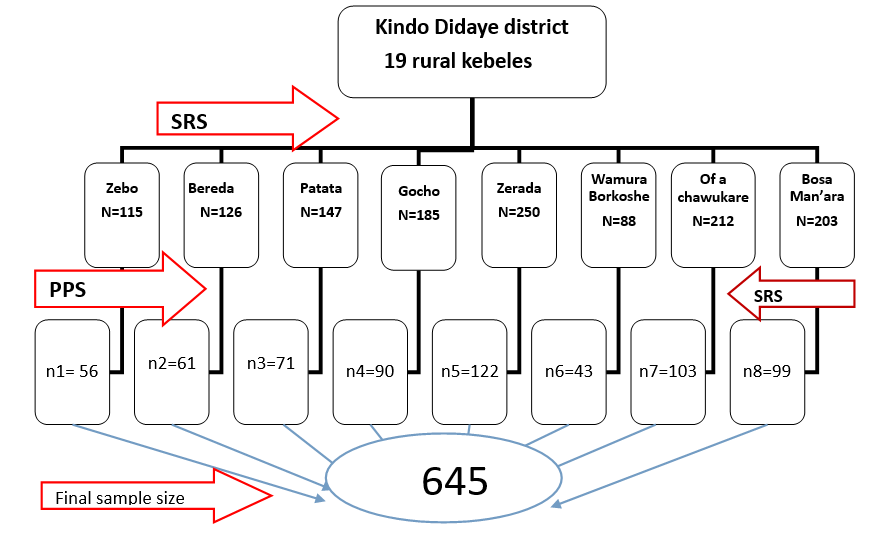
Single population proportion formula was used to determine the required sample with the prevalence of PNC utilization from the study conducted in Nepal (57%) [8] and with the assumption of 95 % CI, the margin of error = 5 % resulted in the calculated sample size was 645 mothers. A multistage sampling technique was used to select study participants. First, 8 rural ‘kebeles’ (lowest administrative unit) were selected randomly by lottery method, and the sample size was distributed proportionally to the size of mothers in these kebeles. To prepare the sampling frame, a census was conducted by HEWs of the selected kebeles to identify mothers who gave birth in the last year preceding the study. Finally, study participants in each kebele were selected by simple random sampling using computer-generated random numbers from the sampling frame (Figure 1).
Participants for FGDs were selected purposively by the principal investigator (PI) using the homogenous method to get rich information on this topic and HEWs led to getting participant mothers.
Data Collection Procedures
For the quantitative part, data were collected by trained data collectors through face-to-face interview techniques using pretested structured questionnaires adopted from reviewing different related literature. The tools consisted of Socio-demographic, economic, cultural, health institution related, reproductive and obstetrics characteristics. The questionnaire was developed in English and then translated into wolayttatto doonaa (local language), and finally, it was retranslated back to English by another language expert to check the consistency. In addition, it was pretested and revised on 5% of the sample in a similar population in one of the kebeles of Ofa district before actual data collection and modified accordingly. or qualitative data, four focus group discussions (FGDs): two FGDs with 18 mothers with similar backgrounds in two conveniently selected kebeles, one FGD with 7 HEWs, and one FGD with 7 heads of the health center and experts of district health office. An interview guide was developed in English and translated to wolayttatto doonaa and then it was checked for validity. All interviews in FGDs were audio-recorded.
Data were entered into Epi-data version 3.1 software and transferred to SPSS version 21.0 for analysis. Descriptive statistics, tables, graphs, means, and frequency distribution were used to present the information. Binary logistic regression was used to identify associated factors among the explanatory variables with P-value < 0>
5.1 Socio-demographic and Economic Characteristics of the Respondents
5.1.1 Socio-demographic and Economic Characteristics of the Respondents for Quantitative Method
Among 645 mothers planned to be interviewed, 640 mothers were interviewed with a response rate of 99.2%. The mean age of the respondents was 28.15 with a standard deviation of 4.27 years and 477 (74.5%) of the respondents were in the age range of 25-34 years.

5.1.2 Socio-demographic and Economic Characteristics of the Respondents for Qualitative Method.
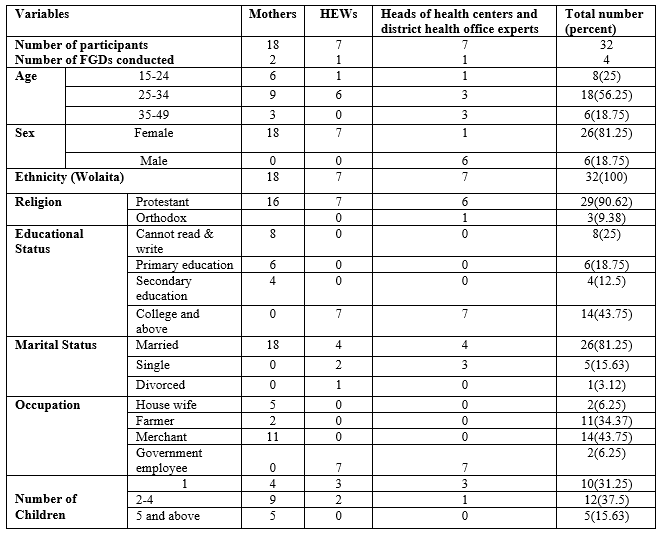
A total of 32 participants were involved in 4 FGDs. The majority (56.25%) of participants were in the age group of 25-34 years. (Error! Reference source not found.).
5.2 Health Institution Related characteristics
Two hundred twenty-five 225(35.2%), 280(43.8%) and 224(35%) of mothers participated in the plan planning HEP, implementation of HEP and construction of HP and/HEWs residence, respectively. (Table ).

5.3 Knowledge and Attitudes Related Characteristics of the Respondents
Four hundred seventeen (65.2%) of mothers had ever heard of PNC services from nearby health posts after delivery. Three hundred seventy-three (58.3%) and 282(44.1%) of the respondents had high knowledge and positive attitude towards health extension PNC service, respectively (Error! Reference source not found.).

This finding was also supported by the FGD result: “… I gave birth to 5 children still I have not utilized health extension PNC service because I am not aware to start to follow up immediately after delivery…” (35 years old mother). Only 34 (5.3%) of respondents replied that their culture has prevented them from attending health extension PNC services. Generally, it is less common to see cultural practices in recent times. “… It was our tradition and belief that postpartum mothers to hold metal or fire to go out of home otherwise she will be exposed to inflammation (“Mich”) but at this time it is seldom to see these practices…” (36 years old mother who delivered 6 times). Also, another discussant said that “…it is considered as a shame for postnatal mothers to go outside before entering church and market (“soofiyaa giyaa”) but that is also clearing out…” (26 years old HEW.)
5.4 Reproductive and Obstetric characteristics of the respondents
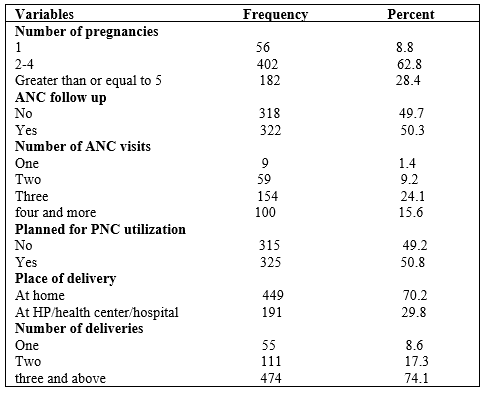
Four hundred two (62.8%) of the mother’s experience of pregnancy (gravidity) were between two to four. Regarding the birth order of the study participants, the majority of the mothers (74.1%) gave birth to three or more babies (multipara). (Error! Reference source not found.).
5.5 Health Extension Postnatal Care Services Utilization
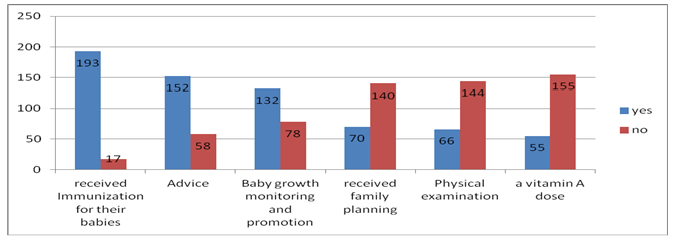
Of the total respondents, only 210 (32.8%) utilized health extension PNC services after delivery within 6 weeks of their last birth but other 21 mothers utilized PNC services from health center/hospital. Immunization service was the most common reported service that mothers received during the postnatal period (Error! Reference source not found.).
The qualitative finding also showed that: "… HEW visited my home at 6th day post-partum, gave polio vaccination to my baby ……."(32 years old mother).
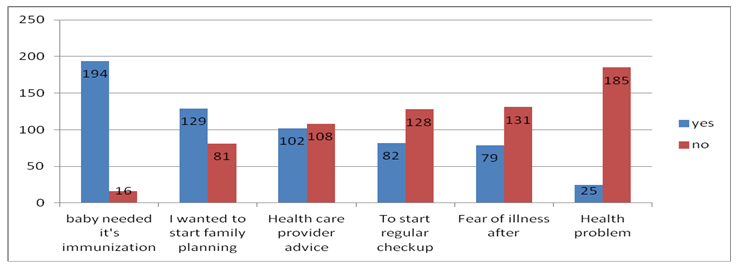
5.5.1 Reasons for utilizing health extension PNC services utilization
Among health extensionPNC services users, the majority (194) mothers used it to have their baby immunized whereas very few (25) mothers used it for they had faced health problems. (Error! Reference source not found.).
The participants in FGDs also stated that “…HEWs visit us and provide vaccination to the baby that prevents him/her from potential health problems….” (25 years old mother).
5.5.2 Reasons for not utilizing health extension PNC services
HEWs were not visiting my home 247 (57.4%) and being free from any health problem 185 (43%) were considered as the reason for not utilizing (Error! Reference source not found.).

FGD participants also mentioned it as follows: “after giving birth at the health center, I was told that the HEW will visit me……I have been waiting for her home visit but she… (name of HEW) had not visited during this time…” (26 years old mother who gave birth to 2 children). Another discussant said that “our home is far from HP; the road is not accessible and thus difficult for us to come back carrying baby …” (30 years old mother).
5.6 Factors associated with health extension PNC services utilization
Bivariate analysis of the data revealed that educational status of the mother and their husband, average monthly income, knowledge of the mother, number of pregnancies any, ANC follow up, plan for PNC services, the number of deliveries, place of delivery, model HH status, participation in planning, implementation and construction of HP/HEWs residence, distance from the nearby HP, frequency of HEWs visit during the last pregnancy and notification of birth to HEWs were the factors found to be significantly associated with the outcome variable at p < 0>
Mothers whose husband attended secondary and above education (AOR = 3.92, 95% CI = (1.77, 8.64)), who have at least one ANC attendance (AOR=2.29, 95% CI: (1.26, 4.19)), who planned to utilize PNC services (AOR=4.73, 95% CI: (2.55, 8.75)), who gave their last birth in a health institution (AOR: 8.03, 95% CI: (4.70, 13.73)), who were visited every month by HEWs (AOR=4.26, 95% CI: (2.32, 7.81)), and who notified HEWs about their birth through HDA (AOR=3.1, 95% CI: (1.52, 6.35)) are more likely to utilize health extension PNC services than their counterparts. (Table 6)
| Variables | Utilized health extension | COR (95% CI) | AOR (95% CI) | |
| Yes (%) | No (%) | |||
Maternal age at birth |
|
|
|
|
15-24 years | 70(64.2) | 39(35.8) | 1.21(0.60, 2.43) |
|
25-34 years | 323(67.7) | 154(22.3) | 1.04(0.57, 1.90) |
|
35 years and above | 37(68.5) | 17(21.5) | 1 |
|
Maternal educational status |
|
|
|
|
Cannot read and write | 326 (70.6) | 136 (29.4) | 1 |
|
Only read and write | 23 (69.7) | 10 (30.3) | 1.04(0.48, 2.25) |
|
1-8 | 72 (57.1) | 54 (42.9) | 1.80(1.20, 2.70) |
|
Grade 9 and above 9 | 9(47.4) | 10 (52.6) | 2.66(1.06, 6.70) |
|
Husband's educational status |
|
|
|
|
Cannot read and write | 199(71.6) | 79(28.4) | 1 | 1 |
Only read and write | 71(80.7) | 17(19.3) | 0.60(0.33,1.09) | 1.84(0.79,4.25) |
1-8 | 128(64.7) | 70(35.3) | 1.38(0.93, 2.04) | 1.68(0.94, 2.97) |
Grade 9 and above | 31(41.3) | 44(58.7) | 3.57(2.11, 6.06) *** | 3.92(1.77, 8.64) ** |
Occupation of mothers |
|
|
|
|
Housewife | 328(66.5) | 165(33.5) | 1 |
|
Merchant | 89(71.8) | 35(28.2) | 0.78(0.51, 1.21) |
|
Others | 13(56.5) | 10(43.5) | 1.53(0.66, 3.56) |
|
Occupation of respondent’s husband |
|
|
|
|
Farmer | 292(66.8) | 145(33.2) | 1 |
|
Merchant | 44(31.7) | 44(31.7) | 0.93(0.62, 1.40) |
|
Others | 43(67.2) | 21(32.8) | 0.98(0.56, 1.72) |
|
Marital form |
|
|
|
|
Polygamous | 21(72.4) | 8(27.6) | 1 |
|
Monogamous | 409(66.9) | 202(33.1) | 1.23(0.56, 2.30) |
|
Average monthly income |
|
|
|
|
Less than 500 | 373 (68.4) | 172(31.6) | 1 |
|
500-1000 | 46(61.3) | 29 (38.7) | 1.37(0.83, 2.25) |
|
Above 1000 | 11(55) | 9 (45) | 1.77(0.72, 4.36) |
|
Model HH status |
|
|
|
|
Did not hear about model family | 154(79.4) | 40(20.6) | 1 |
|
Heard but not at all working towards | 53 (89.8) | 6 (10.1) | 0.44(.17, 1.09) |
|
Working towards model family | 213(59.3) | 146(40.7) | 2.64(1.76, 3.96) |
|
Graduated as model family | 10 (35.7) | 18(64.3) | 6.93(2.97,16.18) |
|
Participation in planning of HES |
|
|
|
|
No | 334 (80.5) | 81 (19.5) | 1 |
|
Yes | 96 (42.7) | 129 (57.3) | 5.54(3.87, 7.93) |
|
Participation in implementation of HES |
|
|
|
|
No | 295 (81.9) | 65 (18.1) | 1 |
|
Yes | 135 (48.2) | 145 (51.8) | 4.87(3.41, 6.96) |
|
Participation in construction of HP/HEWs residence |
|
|
|
|
No | 291 (69.9) | 125 (30.1) | 1 |
|
Yes | 139 (62) | 85 (38) | 1.42(1.01, 2.00) |
|
Distance from nearby HP |
|
|
|
|
More than 10 km | 13(56.5) | 10 (43.5) | 1 |
|
Less than 5 km | 292(64.6) | 292(64.6) | 0.71(.30, 1.66) |
|
5-10 km | 125 (75.8) | 40(24.2) | 0.42(0.17, 1.02) |
|
Frequency of HEWs visits |
|
|
|
|
Not at all | 254(90.7) | 26(9.3) | 1 |
|
Every month | 154(49.8) | 155(50.2) | 9.83(6.20,15.59) *** | 4.26(2.32, 7.81) *** |
Every 3 months | 22(43.1) | 29(56.9) | 12.88(6.49,25.56) *** | 7.67(3.04, 19.37) *** |
Ways to notify HEW about birth |
|
|
|
|
Not notified at all/ i do not know | 299(86.9) | 45(13.1) | 1 |
|
Family members | 68(49.3) | 70(50.7) | 6.84(4.33, 10.81) *** | 5.00(2.69, 9.32)*** |
From health facility | 19(29.2) | 46(70.8) | 16.09(8.66, 29.89) *** | 14.15(5.99,33.44)*** |
Health development army | 44(47.3) | 49(52.7) | 7.40(4.43, 12.37) *** | 3.1(1.52, 6.35)** |
Knowledge of mothers |
|
|
|
|
Low | 222 (83.1) | 45(16.9) | 1 |
|
High | 208 (55.8) | 165(44.2) | 3.91 (2.68, 5.72) |
|
Attitude of mothers |
|
|
|
|
Negative | 241(67.3) | 117(32.7) | 1 |
|
Positive | 189(67.0) | 93(33) | 1.014(0.73, 1.41) |
|
Cultural beliefs & practices |
|
|
|
|
No | 408(67.3) | 198(32.7) | 1 |
|
Yes | 22 (64.7) | 12(35.3) | 1.12(0.54, 2.32) |
|
Number of pregnancies |
|
|
|
|
4 and above | 133(73) | 49(27) | 1 |
|
1 | 34(60.7) | 22 (39.3) | 1.76(0.94, 3.29) |
|
2-3 | 263 (65.4) | 139(34.6) | 1.43(0.97, 2.11) |
|
Number of deliveries |
|
|
|
|
4 and above | 331(69.8) | 143(30.2) | 1 |
|
One | 34(61.8) | 21(38.8) | 0.43(0.80, 2.55) |
|
2 -3 | 65(58.6) | 46(41.4) | 1.64(1.07, 2.51) |
|
Experience of neonatal and postpartum complication |
|
|
|
|
Yes | 374(67.7) | 178(32.3) | 1 |
|
No | 22(66.7) | 11(33.3) | 1.05(0.50, 2.21) |
|
ANC services utilization |
|
|
|
|
No | 276(86.8) | 42(13.2) | 1 | 1 |
Yes | 154(47.8) | 168(52.2) | 7.17(4.85, 10.60) *** | 2.29(1.26, 4.19) ** |
Planned for PNC services utilization |
|
|
|
|
No | 282(89.5) | 33(10.5) | 1 |
|
Yes | 148(45.5) | 177(54.5) | 10.22(6.70,15.58) *** | 4.73(2.55, 8.75) *** |
Place of delivery |
|
|
|
|
At home | 369(82.2) | 80(17.8) | 1 |
|
At HP/HC/hospital | 61(32) | 130(68) | 9.83(6.66, 14.5) *** | 8.03(4.70, 13.73) *** |
*p-value < 0>
Table 6: Factors associated with health extension PNC services utilization in bivariate and multivariate analysis among mothers in Kindo Didaye Woreda, Southern Ethiopia, March, 2017
The prevalence of health extension PNC services (32.8%) was in line with other community based studies conducted in Ethiopia (31.7%) [7] and (34.8%) [11]. This finding is also in line with some African studies but it is higher than EDHS 2016 report and other studies done in different parts of Ethiopia [6, 17, 18]. Moreover, it was higher than study conducted in Malawi [8] and Burkina Faso [18] which was 11% and 25%, respectively. This may be due to the involvement of HAD in service delivery in Ethiopia and in the case of Malawi, CHWs reside outside their catchment area.
However, the level of utilization found by the current study is lower than the findings in Gondar Zuria (66.8%) [10] and the Sidama zone (37.2%) [12]. A probable reason may be the difference in the level of awareness in study areas; about 84.39% of clients were aware of PNC service in Gondar; whereas, only 65.2% heard about PNC services in current cases. Evidence from FGD also supports this idea, “… we have evaluated the last 6 months performance, and PNC services were much lower than the target, unlike other MCH services that need a lot to do in future…” (One of the participants in FGD 4”).
It is also much lower than study in other parts Nepal (50%) and Bangladesh (57%) [8] and Mozambique (40%) [18]. These large differences could be explained that mothers in those countries had better economic status, educational status, antenatal care and institutional delivery service utilization.Mothers whose husbands attended secondary level and above education were more likely to utilize health Extension PNC services. This finding was in line with studies in conducted Ethiopia and other parts of world [7, 15, 19,20].
Women who utilized ANC services were more likely to use health extension PNC services. This finding is consistent with the research conducted in different parts of Ethiopia and abroad [7, 10, and 18]. Evidence gathered from the FGD participants was also in agreement with the finding. “…I had attended ANC visits during my last pregnancy... That is why I preferred to deliver my children in a health facility and I attended postnatal care at HP.…” (A 29 years-old mother, Gocho kebele).
From the result of this study, mothers who planned for PNC services, advised and got appointment for PNC service were more likely to get health extension PNC services. This finding is in line with study conducted in Addis Ababa and is also supported by the reason given by those women who didn’t utilize health extension PNC services during this study [13].
Studies undertaken in Nigeria and Haramaya found that mothers who gave their last birth in health institutions were more likely to utilize PNC service than home delivery [14, 15] . The current study showed consistent results. FGD discussants also said “If mothers deliver at health institution there is more possibility to receive PNC service from HEWs…” (A 25 years-old mother, Gocho kebele). Studies conducted in Tanzania, Malawi, Nepal and Bangladesh contradicts this finding [8,9]. Facility births were less likely to receive early postnatal care at home by HEWs. This might be due to weak linkages between facilities and CHWs; and due to having false guaranty of well beingness by mothers who gave birth at facility than home. In addition, it is affected by frequency of HEWs home visit during the last pregnancy. This was in line with study conducted in different parts of Ethiopia [10, 21], and world [8, 22].
The other major factor affecting health extension PNC services utilization was timely notification of birth to HEWs. A multi-country study conducted in Malawi, Nepal and Bangladesh witnessed that utilization of PNC services increases with timely notification of HEWs [8]. Comparable evidence was also gathered from FGD participants. “… If HEWs are not visiting our home, we do not notify because we are not informed to do so unless we face health problem…” (28 years old mother)., “… mothers are discharged with referral slips to HP to receive remaining PNC services even though not much implemented… (head of a health center), One HEW also stated that “… because mothers are identified during pregnancy through HDA, we link with health center for ANC and institutional delivery, they will inform us and if home delivery happens, development team leaders immediately notify using our mobile phone number…”.
Strength and Limitation of the study
Strength
Qualitative design was used to triangulate with the findings of the quantitative data.
Limitation
First, utilization rate presented here is self-reported from mothers so that recall bias is there then there may be over or under estimation.
The prevalence of health extension PNC services utilization by mothers in the district was very low. And health extension PNC services utilization within the most critical period (first 48 hours after delivery) was very low. This study also revealed that husband attendance of secondary and above education, ANC service utilization, plan for PNC service utilization, institutional delivery, frequent home visit by HEWs during the last pregnancy and notification of birth to HEWS by HDA were found to be significantly associated with health extension postnatal care services utilization. In general accessibility of postnatal services alone is not sufficient by itself to increase the coverage of PNC services utilization. Thus, focusing the identified factors could improve and sustain PNC services from rural health extension workers and all these factors need to be considered when designing an implementation plan for PNC services utilization.
Ethical approval
Ethical clearance was obtained from the Institutional Review Board (IRB) of college of medicine and health sciences, Jimma University, Ethiopia with ethical clearance letter no. RPGe/88/2017. The IRB has given ethical clearance for both oral and written informed consent
Consent
Informed consent was taken from a parent of the study participants after informing them the aim of the study and they have been told as they can withdraw from the study at any step if they feel so as well as confidentiality was granted.
Data availability
It is available on request from corresponding author
The authors declare that they have no competing interests.
The study data collection was funded by College of Medicine and Health Sciences, Jimma University, Ethiopia. The funding body has no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript
ANC: Ante Natal Care
CHW: Community Health Worker
EDHS: Ethiopian Demographic and Health Survey
FGD: Focused Group Discussion
HDA: Health Development Army
HEP: Health Extension Program
HES: Health Extension Service
HEWs: Health Extension Workers
HH: House Hold
HP: Health Post
PNC: Post Natal Care
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
