
Research Article | DOI: https://doi.org/10.31579/2690-4861/212
1Maxillofacial Surgery Unit, University of Naples Federico II, Via Pansini, Naples, Italy.
2Neurosurgery Department, University of Salerno, Via Giovanni Paolo II, Fisciano, SA, Italy.
*Corresponding Author: Stefania Troise, Maxillofacial Surgery Unit, University of Naples, Federico II, Naples, Italy.
Citation: Romano A, Committeri U, Troise S, Maglitto F, Dell'Aversana Orabona G, Norino G, Sani L, Arena A, Barone S, Iaconetta G, Califano L. (2022). Head and Neck Neurothekeoma: Systematic Review of Literature and Presentation of a Lower Lip Aggressive Case Reconstructed with Bengt-Johanson’s Step Technique. International Journal of Clinical Case Reports and Reviews. 11(1); DOI: 10.31579/2690-4861/212
Copyright: © 2022 Troise Stefania, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 08 March 2022 | Accepted: 16 March 2022 | Published: 21 March 2022
Keywords: facial neurothekeoma; head and neck; lower lip; Bengt-Johanson’s step technique, S-100 protein
Aim: Neurothekeoma is a benign lesion of superficial tissue mainly localized in the head-neck area. The aim of the article is to provide a systematic literature review on the tumor’s main characteristics and its correct surgical treatment. We support our theory with the report of an aggressive case of the lower lip region which required a large excision and reconstruction with local flaps.
Materials and Methods: The literature review is based on the scientific materials produced from December 1980 to March 2020 on the head and neck neurothekeomas. In total, 76 papers were included in the study. We presented a classic neurothekeoma S-100 protein positive case that required wide local excision with healthy margins and reconstruction with Bengt-Johanson’s step technique.
Results: Most of the papers were case reports (47,4 %) and reviews (19,7 %) with 721 evaluated neurothekeomas. The male to female ratio was 1:1,8 with a mean age of 26,4 years. The most frequent site of lesions was the head (36,1%), and the three subtypes were divided in cellular (65,7%) mixed (17,5%) and classic (16,8%). The classic neurothekeoma resulted more immunoreactive for S-100 Protein while cellular neurothekeomas for NKI/C3. Our case was successful without recurrence at 1 year follow-up.
Conclusion: Our review highlights that neurothekeoma mainly occurs in young women in the superficial planes of the head and neck. The most frequent type is the cellular one, but the most aggressive is the classic type due to a high local recurrence of protein S-100. A local excision is sufficient for the cellular neurothekeoma, while for the classic type a wide local excision with healthy tissue margins is necessary. The treatment of our case demonstrates that by following this guide, relapse can be avoided.
Neurothekeoma is a benign tumor first described by Harkin and Reed in 1969 and classified as “nerve sheath myxoma” [1]. The term neurothekeoma was coined in 1980 by Gallagher and Helwig in their report on 53 dermal tumors with similar features. [2] Argenyi et al [3] further classified neurothekeoma as classic, cellular and mixed type according to cellularity, mucin content, and growth pattern.
The term “classic neurothekeoma” (classic NTK) will be used henceforth when referring to a tumor also known as a nerve sheath myxoma characterized by an abundant myxoid matrix, and scattered collections of epithelioid schwann cells in corded, nested or syncytial- like patterns, and typically S-100 immunoreactive [4].
The “cellular neurothekeoma” (cellular NTK) is a tumor composed of nests and bundles of variably epithelioid-to-spindled cells often separated by dense collagen septae and classically S-100- negative but NKIC3 positive [5].
The so-called “mixed-type” of neurothekeomas shows overlapping features of both variants [6]. The tumors have been subclassified as cellular neurothekeomas when they have <10>10% and <50>50% myxoid matrix [7].
Generally, the neurothekeoma tumor manifests itself as an asymptomatic, solitary, slow-growing nodule that involves the skin and superficial subcutis of the head and neck region, or of the extremities. It usually requires surgical excision that, based on histopathological and immune histochemical features, can be less or more extended.
In this paper, an extensive review of the literature related to head and neck neurothekeomas has been conducted. Furthermore, a case of lower lip classic neurothekeoma, treated by our team, is presented. The aim of the study is to show the clinical, histopathological and immunohistochemical features of these tumors, and to offer indications for the different surgical procedures according to the characteristics of the neoplasms.
We report the case report and the literature review process.
Case Report
On February 2020, a 64 years old patient was admitted at the Maxillo-Facial Surgery Unit of Federico II University of Naples. The patient was affected by a neoplasia of the lower lip. The Magnetic resonance imaging (MRI) with contrast showed a non-homogeneous captive mass of 2 cm in diameter, hypointense in T1 and hyperintense in T2 in the lower lip that was scarcely differentiated between the skin and the deep muscle planes (Figure 1). Further histological examinations based on incisional biopsy showed a neoplasm with appreciable mitotic activity, with prevalent lobulated areas alternating with diffuse areas, composed of fascicles of fusate or epithelioid cells immersed in a myxoid matrix. The neoplasm resulted immunoreactive to S-100 protein but not to CD31, CD34, p63, CK, Mart1, and HMB45.
An elective surgery to remove the tumor and reconstruct the region was performed.

Surgical Procedure
The surgical procedure consisted of 2 steps. Firstly, the tumor removal and after the use of a stairs flap (Bengt-Johanson’s Step Flap [8]) to reconstruct the defect. Antisepsis procedures were performed with iodine-povidone solution and administration of 1g of intravenous Ceftriaxone. Local anesthesia was realized by infiltration of a 2
Study Design
The literature review on head and neck neurothekeomas was realized adhering to recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) [9].
Data Research
The data were collected from December 1980 to March 2020, and the primary source was the online database of the U. S. Library of Medicine (PubMed). The Medical Subject Headings (MeSH) used were: Neurothekeoma, Face, Head, Neck, Treatment. For the literature search, keyword Neurothekeoma was paired sequentially with the other 4 keywords, having this final formula: (neurothekeoma AND face OR facial) OR (neurothekeoma AND head) OR (neurothekeoma AND neck) OR (neurothekeoma AND therapy OR treatment OR therapeutics). To avoid the loss of interesting articles, accepted by March 2020, a second research was always carried out on Pubmed using only the keyword neurothekeoma and, later on, the results were crossed.
Eligibility Criteria
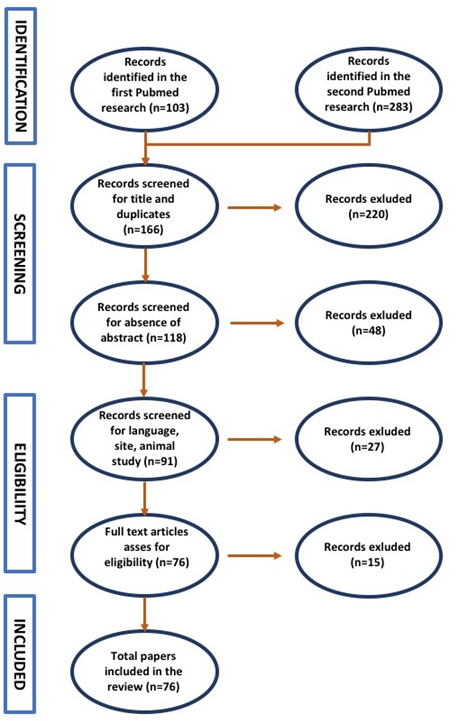
The PubMed search results were screened, and duplicate articles were eliminated. Studies conducted on humans and published in English were considered. The titles and abstracts of the records were screened by one author using the inclusion criteria. We found 103 occurrences in the first research and 283 in the second research. Then the PubMed search results were screened by a carefully reading, and 220 papers were excluded for title not inherent or the duplicates; 48 papers were excluded for the absence of abstract. Moreover, among the 118 remaining PubMed studies, 10 papers not in English, 16 not referring to head and neck, and 1 not referred to humans were excluded (elegibility criteria). At the end, among the 91 studies remaining, 10 papers were excluded because of the presence of only abstract and 5 papers were excluded after a complete reading because not interesting for the topic.
The total number of articles included in our review were 76. The selection process was summarized in Figure 6.
Data Extraction
Data extracted from each article included the type of study, total cases, sex and age of cases, sites of lesions, diameter (if reported) of lesions, invaded tissue, histological and cytological features, expressed immunohistochemical markers, type of treatment performed, subtypes of neurothekeoma. For the purposes of this study, the primary outcome was to identify the characteristics of the different neurothekeoma subtypes and to choose the correct surgical treatment according to these features.
All the 76 analyzed papers and their features are shown in Table 1.
The types of study were divided in 36 case reports (47,4 %), 15 reviews 19,7 %), 12 case series (15,8 %), 12 retrospective observational studies (15,8 %) and 1 letter to editor (1,3 %). In total, the evaluated neurothekeomas cases were 721.
| Author/ Year | Type of Study | N° Cases | Sex | Side of Lesion |
| Local Invasion | Cytological Markers | Hystological Features | Surgical Treatment | Final Diagnosis |
| Gallager 2 1980 | observational retrospective | 53 | 44 F 9 M | 15 up ext, 15 face, 1 oral cavity, 3 neck, 5 shoulder, 3 trunk, 5 lower ext , 2 back | 1 cm | 37 subcutis, 26 dermis | / | nests of spindle cells between bundles of dermal collagen with eosinophilic cytoplasm. Frequent atypical hyperchromatic nuclei and mitotic figures varying from none to 5/10 high-power fields.
| Excision | / |
| Barnhill 5 1991 | case series | 11 | 8 f 3m | 2 scalp, 2 back, 2 nose, 1 chin, 1 shoulder, 1 up extremities, 1 Forehead, 1 ear | / | dermis | S-100, Vimentin and SMA | fascicular pattern (cellular neurotek); prominent myxoid stromal change (classic neurotek) | Excision | 8 cellular 3 myxoid |
| Fetsch 7 2007 | observational retrospective | 176 | 112 F 64 M | 17 nose, 15 scalp, 31 face, 4 neck, 70 up ext, 17 trunk, 20 lower ext, 2 not reported | 1,1 cm | 120 subcutis, 5 muscles plane, 51 dermis | Vimentin, NKI/C3, MiTF, PGP9.5, CD10, NSE, CD68, CD99, alfaSMA, Collagen IV, HMB-45 | nests and bundles of epithelioid cells and spindle cells; eosinophilic cytoplasm; dense hyaline collagen. mild cytological atypia; mitotic rate 3/10 high power fields
| 133 Excision, 33 enucleoresection | 63 cellular neurotek, 66 mixed, 47 classic neurotek |
| Almeida 11 2018 | case report and review | 1 | f | multiple localized oral cavity | 2 cm | submucosal | vimentin, CD63, CD56, whereas AE1/AE3, S100, CD34, α-SMA, GFAP, EMA | spindle and epithelioid cells, forming nests and bundles, supported by fibrous stroma. Rare presence of giant cells. | Enucleoresection | classic neurotek |
| Misago 13 2004 | case report | 1 | F | scalp | 1,5 cm | subcutis | S-100A6 protein, PGP9.5, CD10, CD68 (KP1), PG-M1, Vimentin | Nests of epithelioid cells with abundant and pale eosinophilic cytoplasm, surrounded by spirally arranged stellate cells associated with a moderate amount of mucin. The mitosis rate was 2-3 / 10 high-power fields, without atypical mitotic figures The stroma was collagen and often associated with dense, sclerotic, or hyalinized collagen
| Excision | cellular neurotek |
| Maktabi 14 2019 | case report and review | 1 | m | lateral canthus | 1,5 cm | dermis | CD68, Vimentin, D2–40, SMA | nests of epitheli-oid/spindle cells separated by fibrous septae within a myxoid background | Excision | Mixed |
| Safadi 15 2010 | case report and review | 1 | F | Oral cavity | 2 cm | S-100, NSE | fusiform cells with eosinophilic cytoplasm, myxoid stroma | enucleoresection | classic neurotek | |
| Park 16 2016 | case report | 1 | f | Scalp | 6 cm | dermis | vimentin, CD68, CD10 | spindled and epithelioid cells arranged in fascicles and nodules separated by a collagen-rich stroma | Excision | cellular neurotek |
| Benbenisty 17 2006 | case report and review | 1 | F | nasal wing | 4 mm | dermis | NSE, MiTF, NKI / C3, PGP9.5, SMA, CD10 vimentin, CD68 | nests of epithelioid cells with abundant vacuolated eosinophilic cytoplasm; nuclei with moderate atypia round or ovoid. frequent mitotic figures (4/10 high power fields) but absence of atypical mitoses.
| Large enucleoresection | neurotekeoma cellulare ATIPICO |
| Campanati 18 2006 | case report and review | 1 | f | chin | 6 cm | skeletal muscle | PGP, Ki-67 | diffusely infiltrative borders, vascular invasion, high mitotic | Large Enucleoresection | Atypical neurotek |
| Wilson 19 2008 | case report | 1 | F | nasal wing | 1 cm | NKI / C3, PGP9.5. | spindle cells, focal atypia, high mitotic activity | Large enucleoresection | Atypical neurotek cellular | |
| Papadopoulos 2004 20 | case report and review | 1 | M | neck | 1 cm | dermis | Splindle in a myxoid stroma and separated by strands of collagen. Tumor cells nuclei were fused and rare mitoses were present. | Excision | neurotek mixed | |
| Hornick 21 2007 | observational retrospective | 133 | 83 F 45 M | 27 up ext, 20 face, 10 nose, 4 lip, 3 scalp, 5 neck, 23lower ext, 16 trunk, 13 shoulder, 12 back | 1.1 cm | 69 dermis, 63 subcutis, 1 not reported | NKI / C3, SMA, NSE | nests and bundles of epithelioid cells and spindle cells with pale eosinophilic cytoplasm; dense hyaline collagen. mild cytological atypia; mitotic rate 3/10 high power fields
| enucleoresection | cellular neurotek |
| Rodriguez 23 2015 | case report | 1 | F | orbit | 2 cm | CD34, S-100 protein | myxoid nodules with spindle-shaped or stellate cells; abundant myxoid matrix; no atypia were observed | enucleoresection | classic neurotek | |
| Sanchez-Orgaz 2011 24 | case report | 1 | M | orbit | 1,5 cm | S-100, vimentin, CD68, CD34 e CD10, EMA. | spindle and stellate cells; abundant myxoid matrix. Ki-67 was less than 1%.
| enucleoresection | classic neurotek | |
| Jaffer 25 2009 | observational retrospective | 43 | 24 f 19 m | 9 upper and 4 lower ext, 7 scalp, 5 face, 5 thorax, 5 shoulder, 1 back 7 not available | / | / | S- 100, Vimentin, CD68, NSE, CD56 | plexiform, multinodular, and diffuse, osteoclast-like giant cells, and little or no myxoid stroma, | Excision and Enucleoresection | 8 Myxoid, 15 Mixed, 20 Cellular |
| See 26 2019 | case series and review | 2 | 2 M | orbit | 1 cm | aSMA, MITF, CD10, CD68 | spindle cells with fusiform to oval nuclei with prominent nucleoli, rare mitotic figures; vascular channels | Excision | cellular neurotek | |
| Murphrey 27 2020 | case series and review | 7 | 4 M 3 F | 3 trunk, 3 upper ext 1 nose | / | CD68, NKI/C3 | nests of epithelioid cells with abundant eosinophilic pale colored cytoplasm, fascicular growth. The cellular stroma has been described as collagenic and dense or fibrous | Excision | cellular neurotek | |
| Barnhill 29 1990 | case series | 5 | 3 F 2 M | 5 head-neck (1 frontal, 2 scalp, 1 neck, 1 chin) | 1 cm | dermis | / | fascicles of spindle and epithelioid cells with nuclear atypia, mitotic figures (2/10 per field) and abundant eosinophilic cytoplasm, myxoid stroma and sclerotic collagen with the presence of giant cells
| Excision | cellular neurotek |
| Suh 30 1992 | case report | 1 | F | scalp | / | dermis | S-100 | fusiform and stellate cells; abundant myxoid stroma, eosinophilic cytoplasm, vacuolated nuclei
| Excision | neurotek classic |
| Tiffee 31 1996 | case report and review | 1 | F | Lower lip | / | dermis | S-100 | fusiform and stellate cells; abundant myxoid stroma
| enucleoresection | neurotek classico |
| Tomasini 32 1996 | case series | 2 | 1 F 1 M | 1 trunk, 1 frontal | / | dermis | Vimentin, actin, XIIIa Factor | epithelioid or spindle cells organized in plexuses, large vacuolated eosinophilic cytoplasm; myxoid stroma
| Excision | neurotek cellular |
| Breuer 33 1999 | case report | 1 | F | tongue | 2 cm | Muscles plan | vimentin | spindle cells with few mitoses; hyaline collagen
| enucleoresection | cellular neurotek |
| Yee Hang 34 Wong 2001 | case report | 1 | M | Maxillary and ethmoidal sinuses | / | / | S-100 | spindle cells in sclerotic stroma | enucleoresection | neurotek classic |
| Cohen 35 2004 | case report | 1 | M | Superior Alveolar crest | 3,5 cm | Maxillary bone plane | vimentin, NKIC3 | irregular cell nests in a densely fibrotic stroma; vesicular, ovoid or irregularly shaped nuclei; abundant mitotic activity, 15 mitoses for 10 high-power fields
| Excision | cellular neurotek |
| Ward 36 2005 | case series | 13 | 9 F 4 M | 3 scalp, 2 neck, 1 face, 3 up and 1 lower ext, 2 trunk, 1 not reported | 1 cm | Vimentin, actina (1 cases + S-100 like malignant tumor) | fusiform cells with eosinophilic cytoplasm, myxoid stroma
| enucleoresection | Classic neurotek | |
| Mahalingam37 2006 | case report and review | 1 | M | face | 3 cm | vimentin, NKI/C3, PGP 9.5, factor XIIIa CD68 | / | Excision | cellular neurotek | |
| lopez capeda38 2007 | case report | 1 | F | nose | 1,5 cm | vimentin, mucina, neurofilament | spindle cells arranged in nests with mitosis and collagen
| Excision | cellular neurotek | |
| Koumanis39 2007 | case report | 1 | M | nose | 1,5 cm | vimentin | / | enucleoresection | classic neurotek | |
| Mathew40 2008 | case report | 1 | M | Lower eyelid | 2 cm | S-100 | fusiform and stellate cells; myxoid stroma with collagen vortices, Schwann cells and elongated mast cells. very low mitotic activity
| enucleoresezion | classic neurotek | |
| Zedek41 2009 | observational retrospective | 12 | 9 F 3 M | 2 face, 1 scalp, 4 up and 2 lower ext, 3 trunk | 2 cm | NKI/C3, laminin, CD68, CD10 | absence of atypia, 0.67 / 10 mitosis, large vacuolated eosinophilic cytoplasm, stromal sclerosis
| Excision | neurotek cellular | |
| Wartchow42 2009 | case series | 1 | M | Mandibular gum (reg. 31) | 1.7 cm | actina, S-100 / CD1a, CD4 e CD68 | 16/10 mitosis per field, myofibroblastic characteristics, ki67 <2>
| Excision | neurotek cellular | |
| Muller43 2009 | case report | 1 | F | Medial canthus (left eye) | 1 cm | NKI / C3, SMA, S100 protein | / | Excision | Neurotek mixed | |
| vered 44 2010 | observational retrospective | 4 | 2 F 2 M | Oral cavity | 8 mm | cellular (S100A6, NSE, PGP9.5, vimentin, NKI ⁄ C3); classic (S100A6, NSE, PGP9.5, vimentin, S-100) | / | Excision | Cellular neurotek | |
| Papalas45 2010 | case series | 3 | 3 F | 2upper eyelid, 1 lower eyelid | 6 mm | 2 casi NKI.C3 CD34 positivi, 1 caso S-100, GFPA, Vimentin positivo. | / | Excision | 2 cellular neurotek, 1 classic neurotek | |
| Sheth46 2011 | observational retrospective | 14 | 11 F 3 M | face 2, art sup 7, art inf 3, tronco 2 | / | classic/myxoid: S100B, aSMA; cellular: NSE, aSMA, F13A, NKIC3, podoplanin D2-40, | / | Enucleoresection | 6 cellular neurotek, 8 classico neurotek | |
| Pan47 2011 | case report | 1 | M | Upper lip | 8 mm | NSE, alfaSMA, cd34 | hypercellular epithelioid cells with diffuse and fascicular growth patterns. Casually focal mitosis. No atypia was found.
| Excision | cellular neurotek | |
| Yamada48 2013 | letter to editor | 1 | F | nose | Vimentin, MiTF, NKI/C3, Glut-1, PGP9.5, CD10, NSE, CD68, CD99. | subcutaneous multi-lobular nodular lesion spindle cells separated by a sclerotic stroma and with eosinophilic cytoplasm, ki67 <1>
| Excision | neurotek cellular | ||
| Suarez 49 2013 | observational retrospective | 18 | 17 F 1 M | 5 nose, 4 upper and 3 lower ext 3 trunk , 2 face, 1 scalp | KBA.62, CD10 | epithelioid cells intercalated between bundles of fibrotic collagen, sclerotic large, pale and eosinophilic cytoplasm with mild pleomorphism
| Excision | 1 neurotek classic; 17 neurotek cellular | ||
| Stratton 50 2013 | observational retrospective | 37 | 21 F 16 M | 13 face, 3 scalp, 11 upper ext 4 trunk 4 shoulders 2 lower ext | NKI/C3, MiTF, CD68, CD10 | epithelioid or spindle cells; large vacuolated eosinophilic cytoplasm; myxoid stroma. 4 cases of perineural invasion. 19 cases of cytological atypia, 2/10 mitosis per field
| Excision | 33 neurotek cellulari 4 neurotek classici | ||
| yun 51 2014 | case report | 1 | F | Left eyebrow skin | CD68, Vimentin | thin spindle-shaped and stellate cells within an abundant myxoid stroma
| Excision | Neurotek mixed | ||
| Wang 52 2016 | observational retrospective | 7 | 4 M 3 F | not avaible | NKI / C3, PGP9.5, CD68 | / | nerotek cellulare | |||
| Tham 53 2016 | case report | 1 | M | Oral cavity | S-100 | fusiform and stellate cells; abundant myxoid stroma | Enucleoresection | neurotek classic | ||
| Boukovalas 54 2016 | case report | 1 | F | Nasal wing | 8 mm | subcutis | MiTF | nests and fascicles of spindle and epithelioid cells with pale eosinophilic cytoplasm and vesicular nuclei; background of dense collagen,
| Excision | cellular neurotek |
| Bartake 55 2017 | case report | 1 | F | hard palate | 1,5 cm | submucosal | S100 | myxomatous tissue, stellate and spindle-shaped cells and nerve fibers.
| Enucleoresection | classic neurotek |
| Mora-Cantallops 56 2020 | case report | 1 | M | Medial rectus muscle | 1 cm | muscolo retto mediale | S-100, CD34, CD56 | myxoid matrix with fusocellular and stellate cells. | enucleoresection | classic neurotek |
| Massimo 57 2020 | case series and review | 2 | 1 M 1 F | 1 wrist, 1 upper lip | 8 mm | dermis | CD10, CD68, SMA, and vimentin; | spindle and epithelioid cells with eosinophilic cytoplasm and mild atypia | Excision | 2 cellular neurotek |
| Aronson 58 1985 | case report | 1 | f | scalp | 2,5 cm | dermis | S 100, CEA, DAKO | Polygonal cells; elongated eytoplasmic processes | Excision | classic neurotek |
| Henmi 59 1986 | case report | 1 | f | right nostril | 1 cm | dermis | S- 100 | cell nests consisting of atypical epithelial-like cells | Enucleoresection | classic neurotek |
| Mason 60 1986 | case report | 1 | f | lip | 1 cm | dermis | / | nests and whorls of spindle-shaped cells with abundant myxoid cytoplasm | Excision | Cellular neurotek |
| Pepine 61 1992 | case report | 1 | m | nose | 1 cm | dermis | / | epithelioid and stellate cells in a myxoid stroma | Enucleoresection | classic neurotek |
| Husain 62 1994 | case report and review | 14 | 8 f 6 m | 3lower and 3 up extremities, 2 thorax, 2 scalp, 1 shoulder, 1 lip, 1 face, 1 forhead | / | dermis | S- 100, | stellate and spindle-shaped cells; Nuclear pleomorphism | Excision | 3 myxoid 11 cellular |
| Peñarrocha 63 2000 | case report | 1 | F | tongue | 3 cm | muscles plane | S-100, protein, NSE, and vimentin | fusiform cells with wavy cytoplasm, abundant capillary neovascularization; myxoid stroma | Enucleoresection | classic neurotek |
| Barrett 64 2001 | case report | 1 | m | buccal vestibular sulcus | 1 cm | submucosal | NKI/C3, NSE, SMA PGP, XIIIa, S100 | pale epitheliod cells separated by fasciles of spindle cells | Excision | nerotek cellular |
| Laskin 65 2000 | case series | 11 | 6 f 5m | 2 head, 2neck, 4 lower and 3 up extremities | / | dermis | S100, CIV, SMA, XIIIa | multinodular or lobulated architecture of spinde cells | Excision | classic neurotek |
| Schortinghuis 2001 66 | case report | 1 | m | tongue | 0.8 cm | muscles plane | S- 100, EMA | stellate and spindle-shaped cells with basophilic ovoid vesicular nuclei scattered in a myxoid and avascular stroma |
Enucleoresection | classic neurotek |
| Makino 67 2002 | case report and review | 1 | m | tongue | 1 cm | muscles plane | S100, NSE, VM | spindle- or stellate-shaped cells with a myxoid background. | Enucleoresection | classic neurotek |
| Levin 68 2002 | case report | 1 | m | nose | 4 cm | dermis | S- 100, desmin, vimentin | spindled and ovoid, cells separated by thick collagen bands. | Enucleoresection | classic neurotek |
| Page 69 2004 | case series | 11 | 8 f 3m | 5 nose, 2 neck, 2 lower and 1 upper extremities, 1 shoulder | / | dermis | Mitf, NKI/C3 | spindled and epithelioid cells, | Excision | 2 Cellular 9 Mixed |
| Kim 70 2006 | case report | 1 | f | tongue | 2 cm | muscles plane | CD56, CD68 (clone PG-M1), and desmin | lobules of well-circumscribed oval-to-spindle neoplastic cells in a poor myxoid stroma fibrous connective tissue, | Excision | cellular neurotek |
| Nishioka 71 2009 | case series | 3 | 2 f 1 m | oral cavity | 2 cm | submucosal | S-100 protein, NSE, NGFR | pindle cells admixed with varying amount of myxoid matrix | Excision | cellular neurotek |
| Plaza 72 2009 | observational retrospective | 31 | 23 f 8 m | 10 upper and 5 lower extremities, 4 nose, 4 scalp, 3 thorax, 3 face, 2 shoulder | / | dermis | S100A6, SMA | nests and bundles of epithelioid cells | Excision | cellular neurotek |
| Garcia -Gutiérrez 73 2010 | case report | 1 | m | multiple localized to the face | 2-3cm | dermis | S100A6, CD63 (NKI/C3), CD10, and PGP 9.5 (Figs. 5A–D), XIIIa and vimentin. | spindled to epithelioid cells embedded in a sclerotic stroma with focal areas of stromal hyalinization | Enucleoresection | classic neurotek |
| Kah 74 2011 | case report | 1 | f | palpebral | 1,5 cm | dermis | CD63 | spindle to polygonal cells within a myxoid stroma; eosinophilic cytoplasm | Enucleoresection | classic neurotek |
| Fox 75 2012 | case series | 14 | 6 f 8 m | 3 neck, 4 upper and 2 lower extremities, 2 back, 1 thorax, 1 scalp, 1 shoulder | / | dermis | PAX2, NKI/C3, CD10,MiTF | nests and fascicles of histiocytoid to spindled cells; of nests by collagen bands | Excision | cellular neurotek |
| Emami 76 2013 | case report | 1 | f | oral floor | 0,8 cm | submucosal | CD63, NKI-C3, XIIIa | spindle and epitheloid cells | Excision | cellular neurotek |
| Requena 77 2013 | case series | 9 | 4 f 5 m | lip | / | dermis | S100A6, MiTF, NKI/C3, PGP9.5, EMA, and NSE | plexiform pattern of nests of spindle cells embedded in a slightly myxoid stroma | Excision | cellular neurotek |
| Rozza De Menezes78 2013 | case report and review | 1 | f | right buccal mucosa | 1,5 cm | submucosal | anti-S-100, NSE, EMA | spindle and stellate cells with ovoid vesicular nuclei; myxoid stroma with sparse collagen fibers | Enucleoresection | classic neurotek |
| Bashline 79 2014 | case report and review | 1 | f | scalp | 0,5 cm | dermis | NK1C3 | spindled and epithelioid cells; fascicular growth pattern | Excision | cellular neurotek |
| Fried 80 2014 | observational retrospective | 34 | 20 f 14 m | 7 nose, 11 upper and 5 lower extremities, 3 neck, 3 face, 3 shoulder, 2 thorax, | / | dermis | SOX-10, S100, NKI/C3, SMA, MiTF | spindled and/or epithelioid cells arranged in a fascicular and/or nested pattern with sparse (cellular) or abundant (classic) myxoid component | Excision and Enucleoresection | 25 Cellular 8 mixed 1 NSM |
| Navarrete - Dechent 81 2015 | case report | 1 | m | forehead | 4 mm | dermis | CD10 | spindle cell tumor, including an eosinophilic cytoplasm with mild cellular pleomorphism and moderately dense fibrous stroma | Enucleoresection | classic neurotek |
| Bhat 82 2015 | case report | 1 | f | neck | 4 mm | dermis | S100 | stellate cells with cytoplasmic processes, round to spindle lacking the nuclear atypia and occasional giant cells | Excision | cellular neurotek |
| Gray 83 2016 | case report | 1 | m | eyelid | 4mm | dermis | PGP 9.5, CD68, XIII | nests and bundles of epithelioid to spindled cells with abundant eosinophilic cytoplasm, separated by sclerotic collagen | Excision | cellular neurotek |
| Frydrych 84 2017 | case report | 1 | f | tongue | 6 mm | muscles plane | S100, vimentin, | stellate and spindle-shaped cells. Rare Nuclear pleomorphism and mytotic figures | Enucleoresection | classic neurotek |
| Cavacchini 85 2018 | Case series | 2 | 1 f 1 m | forehead, thing | 7 mm | dermis | EMA, NKI/C3 | Spindle cells; abundant eosinophilic cytoplasm with vesicular nuclei and mild atypia | Excision | cellular neurotek |
| Gallo 86 2019 | case series | 2 | 1 f 1 m | 1 wrist, 1 upper lip | 7 mm | dermis | CD10, CD68, vimentin, and SMA | plexiform and multinodular pattern of spindle and epithelioid cells; multinucleated cells and scattered mitotic figures | Excision | cellular neurotek |
Table 1: Paper’s check list
Clinical features
In most cases the female sex was involved (462 F – 64,1%) with a male to female ratio of 1:1,8. The average age of 721 cases was 26,4 years, with the youngest case of 6 months old, and the oldest of 88 years old. 52.1% of cases were aged between 6 months and 25 years, 35.6 percentage between 26 and 50 years, 12.3 percentage between 51 and 88 years. Neurothekeomas typically presented as asymptomatic, solitary, slow-growing lesions with a mean diameter of 1,5 cm (the smaller lesion measured 0,4 cm while the larger 6 cm). The sites of lesions were: 260 head (36,1%), 187 upper extremities (25,9%), 85 trunks (11,8%), 84 lower extremities (11,6%), 36 shoulder (5%), 23 neck (3,2%) and 46 not reported (6,4%). The 260 head cases were divided in 116 face (44,6%), 59 nose (22,7%), 49 scalp (18,8%), 11 oral cavity (4,2%), 10 lip (3,9%), 7 forehead (2,7%), 6 tongue (2,3%), 2 others (1 medial rectus muscle and 1 paranasal sinuses – 0,8%).
Histological and Cytological features
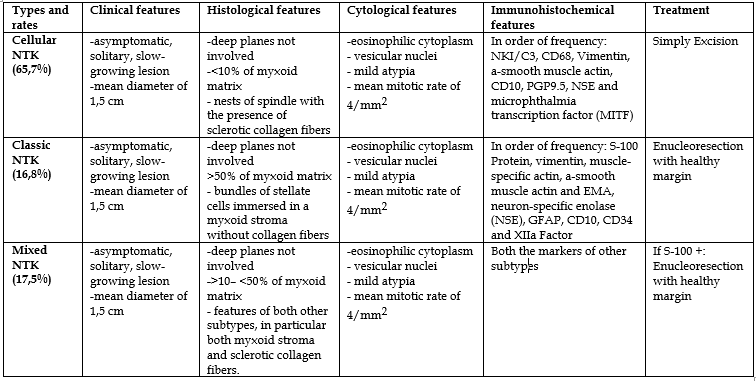
Histologically and cytologically Neurothekeomas were divided in three subtypes: cellular (65,7%) mixed (17,5%) and classic – myxoid (16,8%). All the subtypes presented as dome-shaped masses that most frequently involved the subcutaneous/submucosal plane (55,1% of the total cases) and dermas (41,5%). Skeletal muscle involvement was uncommon (2,9%) and largely restricted to the facial region (mimic muscles and rectus medial muscle). Bone plane involvement was rare (0,5%) and limited to maxillary and mandibular bones. The differences among the 3 subtypes of tumors lied in histology and cytology: 1) Cellular neurothekeoma was characterized by nests of spindle or epithelioid cells immersed in a fibrotic stroma with the presence of sclerotic collagen fibers, and non-tumor multinucleated and osteoclastic giant cells. Tumor cells had abundant eosinophilic cytoplasm with vesicular nuclei, mild atypia and low mitotic rates (ranged from 0 to 16 mitotic figures for mm2 with a mean mitotic rate of 4/mm2). Perineural invasion was uncommon, while vascular invasion was completely absent. Three cases of cellular neurothekeomas were described as atypical because of diffusely infiltrated borders, vascular invasion, severe cellular atypia, and frequent mitosis (until 15/ mm2). 2) Classic neurothekeoma was characterized by bundles of stellate cells immersed in a myxoid stroma without collagen fibers. Tumor cells had abundant eosinophilic cytoplasm with vesicular nuclei, mild atypia and low mitotic rates (mean mitotic rate of 3/mm2). 3) Mixed neurothekeoma was characterized by features of both other subtypes, in particular both myxoid stroma and sclerotic collagen fibers.
Immunohistochemical features
In order of frequency, the neoplastic cells of classic neurothekeomas were immunoreactive for S-100 Protein (86,9% of all cases), vimentin (47,8%), muscle-specific actin, a-smooth muscle actin and EMA (31,8%), neuron-specific enolase (NSE), GFAP, CD10, CD34 and XIIa Factor (18,2%) while NKI/C3 and PGP9.5 in a minor percentage of cases. In order of frequency, the neoplastic cells of cellular neurothekeomas were immunoreactive for NKI/C3 (62,1%), CD68 (55,2%), Vimentin and a-smooth muscle actin (41,4%), CD10 (37,9%), PGP9.5 (34,5%), NSE and microphthalmia transcription factor (MITF) (31,1%), S-100 Protein and XIIa Factor (20,7%) while CD99, collagen IV, HMB45, CD34, NGFR, PAX2, EMA and Podoplanin D2-40 in a minor percentage of cases. In the mixed neurothekeomas, in addition to the markers already mentioned, also CD56 and SOX10 were found.
Surgery and Follow-up
In all cases, the tumors were treated by surgery. In particular, cellular neurothekeomas were treated by a simple excision, while classic and mixed neurothekeomas as well as the atypical cellular forms were treated by enucleoresection with healthy margins and, if necessary, reconstruction.
The reported percentage of recurrence was 7,5% without cases of metastasized tumor. Main features of the three neurothekeomas types are summarized in Table 2.
Neurothekeoma is a slow-growing benign tumor that interests mainly superficial tissues and has been studied since the 1980s. The first author who coined this term was Gallager [2] who, in a retrospective observational study on 53 patients, described a benign tumor of the dermis having a neural origin and a relationship to the Schwann sheath cells of peripheral nerves. The interest in the study of this type of lesion has grown over the years, and several authors dedicated to defining the origin, the etiopathogenesis and the clinical, histological, and immunohistochemical characteristics. Thus, the data obtained from our review were compared with the international literature on this topic. [10] First of all, Neurothekeomas tends to occur in younger age, around the second or third decades with a mild female predominance [10]. Our review, according to literature analysed, highlights a male to female ratio of 1:1,8 and a mean age of 26,4 years [11]. The tumors have been classified in three subtypes based on etiopathogenetic, cyto-histological, and immunohistochemical characteristics: cellular neurothekeomas with <10>50% of myxoid matrix7. The term ‘‘cellular neurothekeoma’’ was first used by Rosati et al.in 1986 to distinguish it from the myxoid variant which was defined as “classic neurothekeoma” [12].
The cell of origin of NSM is controversial: Fetsch et al [7] postulated that SMA and EMA positivity suggests some similarity to histiocytic cells and fibroblasts, while S100 protein and NSE to Schwann cells or other perineural cells. So cellular NTK can origin by histiocytic cells and fibroblasts, while classical NTK by Schwann cells and other perineural cells. Moreover, Misago et al [13] distinguished a histiocytic origin from a fibroblastic or nervous one, based on the expression of different genes: Cellular neurothekeoma expressed genes involved in macrophage differentiation, Cell migration, cytoskeleton organization, Fibroblast growth, tissue remodeling, ECM mineralization such as ADAM12, DPT, FAP, PDPL, MMP1 and TNFAIP6. Classic neurothekeoma expressed genes involved in neural crest development, myelin and axonal growth and neuronal adhesion such as SOX10, MPZ, NTM, SOX2, PMP2, NCAM1, MBP and SORBS1. KP-1 and PG-M1 expression is associated to histiocytic differentiation [13].
Our review, according with the literature [14,15], highlights that the head and neck are the most affected sites (39,3%) with the face and the nose at the highest occurrences. Cases of the oral cavity are rare and mainly concentrated on the area of the lips (3,9%). The most common intraoral site is the tongue.
Several authors [7,14,15] reported that tumors were non-capsulated, located in dermal tissue with a subcutaneous involvement in 85% of the cases, and typically organized in multiple small nodules. Our research confirms that the involvement of the deep planes is rare (3,4%). Mean diameter was 1,5 cm, 90% of lesions between 0,4 cm and 2 cm, but tumor size of 6 cm was described and defined as atypical [16-18]. Wilson et al [19] affirmed that it is characterized by large size of up to 6 cm, penetration into subcutaneous fat or muscle, diffusely infiltrating borders, vascular invasion, a high mitotic rate, and marked cytological pleomorphism. Based on our data, the most common subtype is Cellular Neurothekeoma (65,7%). All the three subtypes of tumors were associated with some sclerotic collagen that was most present in cellular neurothekeomas and least evident in the myxoid examples. Moderate or marked collagen deposition around individual tumor nodules was noted predominantly in cellular neurothekeomas. Osteoclast giant cells are also present, but they are generally sparse and do not appear to be neoplastic [7]. They are identified predominantly in cellular neurothekeomas. The myxoid stroma is more abundant in the classical subtype [20].
In terms of cytomorphology, in accordance with literature [21] cellular neurothekeomas were composed of spindle cells (28%), of epithelioid cells (14%), and of cells with variably epithelioid to spindled features (58%). Classic neurothekeomas were composed of spindle cells (54%), of stellate shaped cells (49%) and of epithelioid cells (7%). The tumor cells contained pale vacuolized eosinophilic cytoplasm and in 70% showed mild atypia in terms of abundant vesicular, ovoid or irregularly shaped nuclei with prominent nucleoli. Cellular neurothekeomas in 10% of cases showed giant cells. The mean mitotic rate was 4 per 10 high power fields (HPF) (range, 0 to 16) for cellular neurothekeomas and 3 per 10 HPF for classic neurothekeomas. Only 4% of total tumors showed perineural invasion, and 3% showed vascular invasion.[ 3 - 7]
In terms of immunohistochemical features, our review showed that the neoplastic cells of classic neurothekeomas were mainly immunoreactive for S-100 Protein (86,9% of all cases), vimentin (47,8%), muscle-specific actin, a-smooth muscle actin and EMA (31,8%) and neuron-specific enolase (NSE), GFAP, CD10, CD34 and XIIa Factor (18,2%). The expression of these factors confirms the neuronal or perineuronal origin of the classical neurothekeoma. Moreover, the expression of the S-100 protein is connected with a high local recurrence. [3 - 7] In their observational study, Fetsch et al [22] documented 16 on 34 (47%) recurrent disease on follow-up in classic neurothekeomas S-100 protein positive locally excised. Considering a relatively high local recurrence rate, a complete local excision with a margin of healthy tissue should generally be considered an optimal treatment of the disease. Hence, as the analysis of the literature [15,23,24] revealed, classic neurothekeoma with S-100 protein positivity should be excised with safety margins to prevent local recurrences. This result justifies our aggressive surgical approach with safety margins of 1 cm of healthy tissue.
The neoplastic cells of cellular neurothekeomas were mainly immunoreactive for NKI/C3 (62,1%), CD68 (55,2%), Vimentin and a-smooth muscle actin (41,4%), CD10 (37,9%), PGP9.5 (34,5%), NSE and microphthalmia transcription factor (MITF) (31,1%) confirming the histiocytic and fibroblastic origin. [13,25] The analysis of literature [26,27] showed that in these cases the recurrence rate is low, so the chosen treatment is a local excision with a few millimeters of healthy tissue.
Our case was a classic neurothekeoma with immunoreactivity to the s-100 protein. For this reason, we opted for a surgical treatment of complete excision with margins of 1 cm of healthy tissue. Considering the position and the size of the tumor, this excision required a reconstruction with local flaps. Based on data for the selected case in the literature, the Bengt-Johanson’s step flap was considered the best option. [8,28] This technique has proved to be effective both in terms of functionality and aesthetics for our patient. Furthermore, the large excision with safety margins avoided relapses at the one-year follow-up.
Our review highlights that neurothekeoma is a benign tumor that mainly afflicts young women and mainly occurs in the superficial planes of the head and neck. Among the three types, the cellular type is the most frequent, but the most aggressive is the classic one because the expression of the S-100 protein determines a high local recurrence. For this reason, a local excision treatment is sufficient for the cellular neurothekeoma while in the classic type with the presence of this protein, a wide local excision with healthy tissue margins is required. The treatment of our case demonstrates that, by following this guide, relapse can be avoided.
Funding: Not applicable
Conflicts of interest: The authors report no conflicts of interest
Availability of data and material: Not applicable
Code availability: Not applicable
Ethics approval: Only the patient’s consent was requested.
Consent to participate: Patient’s consent was obtained.
Consent for publication: Patient’s consent was obtained.
Financial Disclosure Statement: The authors have no financial interest to declare regarding the content of this article.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
