
Case Report | DOI: https://doi.org/10.31579/2643-6612/028
* Clinical Professor Master of Periodontology Universitat International the Catalunya, Barcelona, Spain. Private Practice, Catania, Italy.
*Corresponding Author: Francesco Amato, Clinical Professor Master of Periodontology Universitat International the Catalunya, Barcelona, Spain. Private Practice, Catania, Italy; Viale A. De Gasperi 187, Catania, Italy.
Citation: F Amato. (2022). Guided Tissue Regeneration on a Mandibular Molar with a “Beyond the Apex”Periodontal Defect. Dentistry and Oral Maxillofacial Surgery. 5(2); DOI: 10.31579/2643-6612/028
Copyright: © 2022 Francesco Amato, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 01 December 2021 | Accepted: 21 January 2022 | Published: 01 February 2022
Keywords: guided tissue regeneration; apex; alloplastic graft; resorbable membrane
This case report clinically shows complete regeneration on a perio-endo lesion that caused a crater-like defect extending beyond the apex on a mesial root of a mandibular left first molar. The regeneration was obtained using a collagen membrane (Bioguide) in combination with an alloplastic bone graft (Endobone3i Biomet).
The Patient presented a 13 mm periodontal pocket mesially and buccally and a grade III furcation involvement on tooth # 36, which was the distal abutment of a three-unit bridge.
After raising a flap and performing a thorough debridement of the defect, clinical observation revealed a crater-like defect 15 mm deep that involved the mesial root and extended beyond the apex. Alloplastic bone particles were used to fill the defect and recreate the original bone architecture. The graft was then covered with a resorbable membrane shaped to be adapted to the mesial area buccally as well as lingually, then the flap was sutured.
A 5-year follow-up radiograph shows the complete defect fill, a pocket depth reduction to 2 mm and stable tissue conditions.
This case clinically shows the possibility to regenerate periodontal tissues on a defect that extended beyond the apex of a molar root.
Periodontally compromised teeth can be treated predictably with different modalities and long term results have been well documented [1]. When the periodontal disease involves a molar, the dentist has to face a greater challenge because of the furcation [2]. In fact thorough instrumentation of the area is difficult for the operator as well as oral hygiene for the patient [3-4]. Furthermore molars with furcations involvement are treated according to the amount of horizontal and vertical defect [5].
For this reason various classifications have been proposed based on the horizontal and vertical size and shape of the lesion [6-5].
It has been proven that molars with Grade I and II furcation involvement can be successfully treated with GTR [7-8].
For molars with grade III and IV, although some reports have shown tissue regeneration, resective surgery appears to be more predictable, but it has unfavorable long term results [9].
So different treatment options have been proposed: root-amputation, tunneling or ultimately extraction.
Guided tissue regeneration is the ideal treatment to recreate the periodontal attachment that has been lost on a tooth due to periodontal disease, but applying a membrane to a molar defect may involve some difficulties [10-11]. In fact size and shape of the molar trunk do not always allow for good adaptation of the membrane thus resulting in post-operatory infection, premature membrane exposure and loss of the graft [12].
In this clinical case even if the size and the shape of the defect would suggest to treat the tooth with resective surgery or extraction to ensure predictable results, guided tissue regeneration has been applied successfully with stable 3-year follow-up results [13].
In January 2010 a 60 years old male presented after recurrent episodes of abscess in the left mandibular molar area. The previous dentist had treated the patient with scaling, root planing, an open flap debridement and prescribing antibiotics, but the abscess episodes were recurring and the patient had constant discomfort.
The medical history revealed that the patient was in good health and a nonsmoker.
The dental history revealed full compliance with the hygiene maintenance program.
The clinical examination showed good oral conditions, adequate plaque- control in all the mouth, tooth # 36 was the distal abutment of a three-unit bridge replacing the missing second premolar.
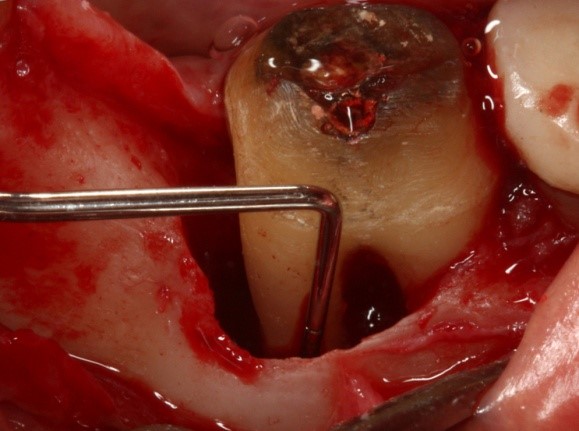
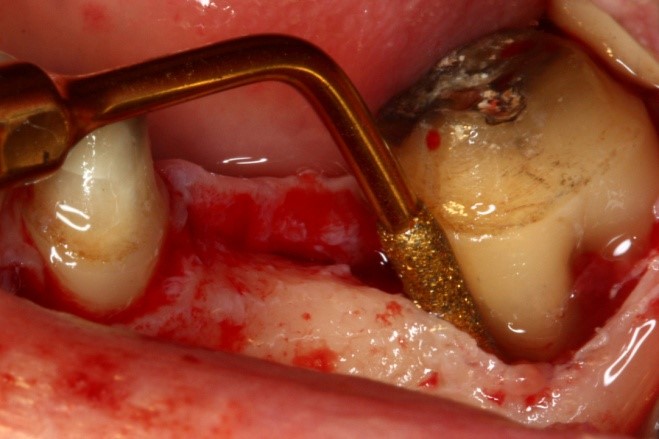
Periodontal examination revealed 13 mm probing depth mesially and buccally on tooth # 36 (see figure. 1a, b) and a grade III furcation involvement.


The X-ray examination showed severe bone loss on the mesial root that involved the mesial surface of the distal root and extended a few millimeters beyond the root apex on tooth #36 (see fig. 2).

Localized severe periodontal disease with a vertical component on the mesial root on tooth #11 was diagnosed. This was probably due to an overhanging on the margin of the crown fabricated on a tilted molar. The patient was informed of the extreme condition of the tooth and although he was informed that extraction was the most predictable way to solve the problem, he wanted to try to save the tooth anyway because it was supporting the bridge. Guided tissue regeneration periodontal surgery was proposed and an informed consent was signed by the patient.
The first procedure was to replace the old bridge with a new better fitting provisional.
72 hours before periodontal surgery, the patient underwent initial therapy and was asked to start using chlorexidine rinse three times a day to be continued for two weeks after.
Antibiotic coverage (amoxicilline 1 gr.) was prescribed for the patient to take twice a day for ten days starting 12 hours prior to surgery.
After local infiltration with Articaine 1:100.000 (Ubistesin 3M ESPE) an intrasulcular incision was carried out on the mandibolar molars buccally and lingually extending mesially up to the 1st premolar.
A full thickness mucoperiosteal flap was raised both buccally and lingually.
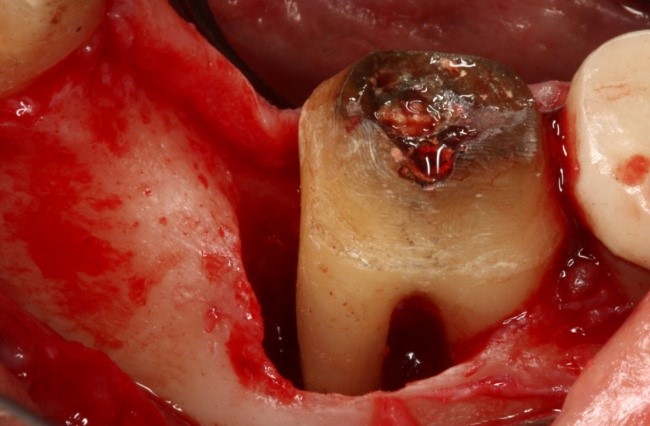
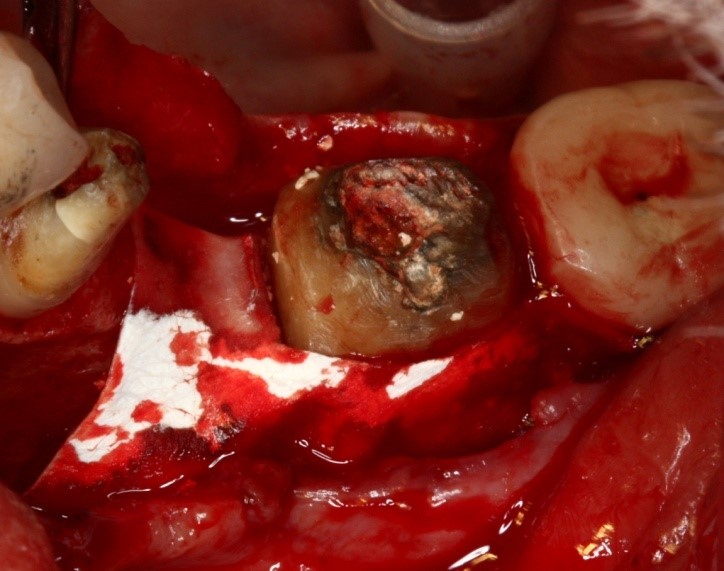
After a thorough degranulation a 15mm osseous vertical defect with a 10 mm crater-like infra-bony component was visible on the mesial and buccal aspect of the tooth with a through and through furcation involvement extending 4 mm beyond the apex of the mesial root (see figure 3) .


The flap was then closed with interrupted suture (4-0 Ethicon Johnson & Johnson). In the same visit the decay was cleaned and the root-canal therapy was completed (see figure 9).

The patient was then seen once a week for the following three weeks for suture removal and hygiene maintenance in the wound area and then once a month for recall visits.
Clinical Outcome
Five years follow-up recall visit showed stable healthy conditions.
Clinical and radiographic examination revealed complete defect filling, full graft integration (see Figure. 10), absence of inflammation and three mm probing depth mesially and buccally on tooth # 36 (see Figure 11a,b).



The possibility to regenerate periodontal tissue in the molar furcation area represents a great challenge for the periodontist, especially in grade III furcation involvement with deep lesions [14].
Deep biological knowledge, good skills and appropiate surgical tools represent the key to predictable success.
In this case all the following elements may have played a role in the clinical success: careful debridement and root planing in the inter-radicular as well as in the apex area with piezosurgical tips purposedly shaped, together with the use of a solid scaffold graft and a membrane that allowed for tissue maturation [15].
Molar lesions with furcation involvement and extending beyond the apex of one of the roots can be successfully treated with guided tissue regeneration.
More data, larger number of cases and longer-term follow-up are necessary to further validate this clinical study.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
