
Case Report | DOI: https://doi.org/10.31579/2640-1053/105
1 Head of Department of Neurosurgery Bejaia Hospital, Bejaia, Algeria.
2 Neurosurgery Department, Mustapha Pacha University Hospital, Algiers, Algeria.
*Corresponding Author: Bekralas H. Head of Department of Neurosurgery Bejaia Hospital, Bejaia, Algeria.
Citation: Bekralas H, Habchi N. (2022). Grisel Syndrome About A Case. Cancer Research and Cellular Therapeutics. 6(1); Doi:10.31579/2640-1053/105
Copyright: © 2022 Bekralas H, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 11 December 2021 | Accepted: 27 December 2021 | Published: 05 January 2022
Keywords: grisel syndrome; torticollis; nasopharyngitis; atloaxoedian dislocation
Grisel syndrome, also known as nasopharyntic torticollis is a combination of a torticollis and nasopharingitis, describes first time in 1830 by bell and taken over by grisel in 19305which descibed two observations in two children complicated renopharyngitis since this syndrome bears his name.characterized clinically by sudden probing and radiographically by an enucleation of the atlas innon traumatic dislocation- rotating position . physiopathologically is caused by the inflammatory contracture of the prevertebral muscles whose origin could be a spontaneous or post opérative infection of the NTE area.This acute febrile torticollis is a rare affection mainly affects the child with an estimated age range between 8 months to 12 years, few cases are reported by literature concerning adults.Diagnosis should be realized early in order to avoid neurological restoration which cannot be carried out with certainty that other diagnoses of febril torticollis are eliminatedThe treatment is simple, the prognosis is often favorable with an adequate and early attitude directed towards the causal agent while restoring the spinal stabilit.
Grisel syndrome, or nasopharyngeal torticollis, is a non-traumatic atloaxoid dislocation (c1-c2), it is one of the causes of acute febrile torticollis in children occurring before or after an infection of the ENT sphere. In 1930 Grisel described a torticollis that occurred suddenly in a child, characterized radiologically by an enucleation of the atlas at the origin of an atloaxoid luxation, secondary to an inflammatory contracture of the prevertebral muscles, the origin of which could be be a spontaneous or postoperative infection of the nasopharynx or retropharyngeal space.The appearance of a “spontaneous” atloaxoid subluxation after ENT surgery is rare, since certain cervical pain and stiffness are usual and anti-inflammatory treatment is often introduced early. The diagnosis of certainty is often difficult to carry, it is retained after elimination of the other causes of febrile torticollis.Treatment of febrile torticollis involves treating the infection and muscle contracture to prevent the development of a vicious attitude and hence dislocation.
Bell (1830) described a case of lethal atlooaxoid subluxation after a throat infection (syphilitic ulceration of the pharynx) in which erosion of the transverse ligament led to compression of the spinal cord. Grisel, 1930; Grisel and Bourgois, 1931, Robinson and Boer (1981) described a case of spontaneous atloaxoid subluxation in a 7-year-old child after Pharyngoplasty. Several theories on the causes of this subluxtation have been advanced, the infectious origin is the most implicated, however no specific bacterial agent has been isolated so far.Paping et al. (1985) presented Grisel's syndrome in a 4-year-old girl, secondary to bilateral fulminant otitis media, Fusobacterium necrophorum was found in blood and ear culture
We report the case of an 08-year-old girl with no medical history. Having presented otalgia 03 months before admission in a febrile context, the diagnosis of acute otitis retained and antibiotic treatment initiated. On D2 after antibiotic therapy, the earaches have totally regressed, however a febrile torticollis sets in, which has prompted numerous consultations with rehabilitation of antibiotic and anti-inflammatory treatment but without any notable improvement, which prompted a consultation in the neurosurgery emergency room. the clinical examination in the emergency room found a torticollis with contracture of the pre-vertebral muscles, without sensitivo motor deficit.

Clinical examination in the emergency ward
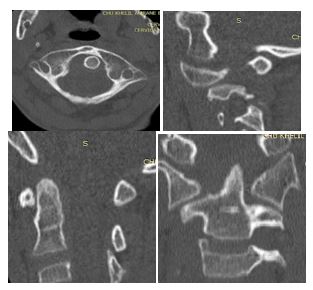
The child received, before hospitalization, a cervical CT showing atloaxoid rotatory dislocation C1-C2 classified: type IV by FIELDING and HAWKINS
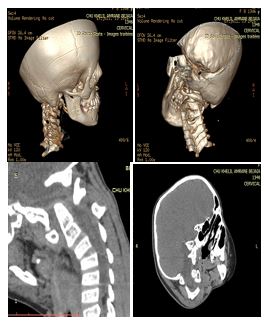
Bone and parenchyment window CT scan with 3D reconstructionAdmission is then made, transcranial traction under sedation with an initial weight of 500g was performed, then increased to 1kg the next day. a control cervical CT was performed showing a reduction in dislocation classified as type 1 of FIELDING and HAWKINS

Patient under tractionTranscranial traction was maintained for 15 days, the clinical and radiological outcome is very satisfactory with a total reduction in dislocation and disappearance of muscle contracture. the child was kept under orthopedic restraint with a philadelphia type mineral with chin support for 03 months.
Grisel syndrome is a non-traumatic torticollis developing in a feverish context, it is not uncommon, but can go unnoticed due to the initiation of antibiotic treatment of the causative agent before the onset of neurological complications. The infections of the ENT sphere are very often linked to this syndrome.The treatment of grisel syndrome is simple at the beginning, it is based on an antibiotic and anti-inflammatory treatment, the evolution is then favorable after a few days of treatments a clinical and radiological control is necessary in order to avoid the neglect of a possible atloaxoid dislocation, the treatment of which is often cumbersome and expensive.
The diagnosis of Grisel syndrome or nasopharyngeal torticollis must be made early in order to avoid the onset of neurological complications. Prevertebral muscle contracture is of inflammatory origin. Atloaxoid subluxation is not an aggravating factor for torticollis, but rather a consequence of the latter.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
