
Case Report | DOI: https://doi.org/10.31579/2768-2757/069
1 Department of Plastic Surgery of Doctor Negrín University Hospital, Resident.
2 Department of Plastic Surgery of Doctor Negrín Hospital University, Attending.
3 Department of Plastic Surgery of Doctor Negrín Hospital University, Chief.
*Corresponding Author: Laura Fueyo Suárez, Hospital Universitario de Gran Canaria Doctor Negrin, Barranco de la Ballena s/n, 35010, Las Palmas de Gran Canaria, Spain.
Citation: Laura F. Suárez, Mónica F. Monasterio, Javier F. Palacios, (2023), Gorlin Syndrome: Clinical Features, Pathogenesis and Updated Treatment. A Case Reports, Journal of Clinical Surgery and Research, 4(1); DOI:10.31579/2768-2757/069
Copyright: © 2023, Laura Fueyo Suárez. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 10 March 2023 | Accepted: 17 March 2023 | Published: 27 March 2023
Keywords: gorlin syndrome; basal cell nevus syndrome; vismodegib; PTCH1
Aim: to present an updated review of the diagnosis and treatment of Gorlin Syndrome.
Methods: A bibliographical review was performed on PubMed using the keywords Gorlin syndrome, Basal cell nevus syndrome, Vismodegib, PTCH1. 24 articles out of a total of 2588 articles were fully reviewed, with 3 more being partially considered based on relevant content.
Results: Our patient was operated several times, with a total of 31 lesions being removed, all of which were confirmed pathologically as basal cell carcinomas (BCC). After several recurrences, locally advanced BCCs and multiple new lesions presenting in every visit, the case was considered not manageable through surgery alone and adjuvant Vismodegib treatment was suggested. The patient declined due to its side effects and is currently under observation.
Discussion: Gorlin syndrome is a rare entity that presents in one of every 56,000 adults. It is autosomal dominant without sex-biased prevalence. It is primarily associated to the PTCH1 tumor suppressor gene, located in chromosome 9q22.3-q31. The appearance of multiple BCCs is influenced by multiple risk factors such as solar exposure and radiotherapy, which can increase the rate of new lesions. The first treatment choice is surgery, with locally advanced or recurring carcinomas being treatable with a systemic inhibitor of the Hedgehog signaling pathway as an adjuvant trearment. The main limiting factor of the use of Vismodegib is its adverse side effects, though they are known to diminish over time. New treatments under study include intermittent Vismodegib treatment and topical use of inhibitors of the Hedgehog pathway, which could potentially reduce side effects and impact patient prognosis.
Conclusions: Treatment of patients with Gorlin Syndrome is multidisciplinary, and conditioned by the constant development of new carcinomas. This sometimes requires the use of systemic treatments, which present a high number of side effects that limit their use. In recent times, new topical drugs that inhibit the Hedgehog pathway are under study. These have a lower rate of side effects and could become an effective treatment alternative.
Gorlin syndrome, also known as Nevoid Basal Cell Carcinoma Syndrome (NBCCS), is a rare genetic disorder characterized by the development of multiple basal cell carcinomas from a young age [1]. Their clinical behavior is variable and, in some cases, locally aggressive. Other common symptoms are odontogenic keratocysts, palmar and plantar pits, skeletal malformations, and abnormalities in development, making a multidisciplinary approach necessary for this disorder [2]. NBCCS has autosomal dominant inheritance with variable expression and penetrance, and it is caused by mutations on the Sonic Hedgehog signaling pathway. The best known of these mutations is the deactivation of the PTCH1 tumor suppressor gene, located in chromosome 9q22.3-q3 [13]. The diagnosis of this syndrome is clinical and based on a set of major and minor criteria4, and it can be confirmed through direct analysis of the genetic mutation5. The gold standard treatment is the surgical resection of the BCCs, although a high number of locally aggressive or recurrent lesions warrant the use of systemic treatments, despite their adverse effects, in order to prevent the appearance of new lesions. The objective of this article is to review the bibliography of the currently published papers on Gorlin syndrome, its pathogenic development, clinical characteristics, and therapeutic management, through the study of a complex case diagnosed and treated in our department. Through this, we aim to analyze in detail the current knowledge on this infrequent entity and evaluate its current and future management alternatives.
A bibliographical search was performed in PubMed with the following keywords: Gorlin syndrome, Basal cell nevus syndrome, Vismodegib, PTCH1. 24 articles out of a total of 2588 articles were fully reviewed, with 3 more being partially considered based on relevant content. A case study, operated on by our department, is presented, along with the experience acquired through its management.
A 48-year-old male presents to our Plastic Surgery department with a history of six lesions resected by the Dermatology department throughout the past ten years, all of them with the anatomopathological result of basal cell carcinoma (BCC). The patient also had a record of several removed odontogenic keratocysts in the maxillary sinus and mandible. Palmar and plantar pits, as well as macrocephaly were observed during physical examination. The patient matched three major and one minor criteria, and thus a clinical diagnosis of Gorlin syndrome was established.
The patient was referred to our department due to a large, ulcerated, piercing lesion of pearly edges with arborizing telangiectasias, compatible with BCC, in the left orbital region, having produced ocular atrophy and blindness. An exenteration of the orbit was performed and covered with an anterolateral thigh flap (ALT). Furthermore, the patient presented multiple lesions compatible with BCC across the surface of his body. These were deferred to be removed after recovery.

Figure 1: BCC of the left orbital region

Figure 2: intraoperative orbit exenteration

Figure 3: 2 weeks follow up with ALT flap reconstruction
Six months later, the patient underwent excisional biopsy with wide margins for thirteen lesions suspected of being BCCs, the location of which is shown in the following figures. Three of the resected lesions did not respect the resection margins.
Direct closure was performed in most locations, with coverage of the left shoulder being achieved with a myocutaneous pedicled Latissimus Dorsi flap, and the right retroarticular lesion being covered with a preauricular pedicled flap.

Upon the recurrence and appearance of new lesions, and after having resected a total of twenty BCC (some locally aggressive, others recurrent), it was decided that the patient should be followed up and referred to the Medical Oncology department in our center to consider starting a systemic oral treatment with a Hedgehog pathway inhibitor, Vismodegib. After having informed the patient of the possible adverse effects of the treatment, he refused to receive it.
Three months after the previous surgery, the patient is once again operated on, with four more lesions being removed from the shoulder and dorsal region. Five months later, three more lesions were resected from the nasal dorsum, the right side of the thorax and right side of the back. Finally, in July 2021, four more lesions were removed: one in the left ear and three in the right half of the back. The anatomopathological result of all the removed lesions was BCC.
Today, after a total of thirty-one removed lesions, all of which were compatible with basal cell carcinoma, the patient is being followed up by Medical Oncology and our Plastic Surgery departments, as well as Internal Medicine after having developed constitutional syndrome.
Gorlin syndrome, also known as Nevoid Basal Cell Carcinoma Syndrome (NBCCS), is a rare entity with a prevalence that varies between 1:57,000 and 1:256,000, without distinction by sex6. Several mutations have been identified as playing a part in Gorlin syndrome, found in genes involved in the Sonic Hedgehog cell proliferation and differentiation pathway. The most common finding is the loss of heterozygosity in PTCH1, followed by PTCH2 and SUFU. The PTCH1 gene, present in chromosome 9q22.3-q31, is a suppressor of this pathway. Therefore, its alteration leads to an uncontrolled cell proliferation [6,7,8].
This syndrome predisposes to the formation of malignancies and developmental abnormalities, with the formation of multiple basal cell carcinomas being particularly notable from early ages of life. These BCCs have a histology and behavior similar to sporadic ones, but it should be noted that, due to their appearance at early ages, it is more common to find locally aggressive lesions owing to their longer evolution time. Nevertheless, it is uncommon to find carcinomas so advanced that they reach the facial bones [2]. It is also common to find odontogenic keratocysts and palmoplantar pits, as well as facial malformations such as hypertelorism, macrocephaly, and cleft lip or palate. Other malignancies also have higher prevalence rates on these patients, such as medulloblastoma, cardiac fibromas or meningiomas [4].
Diagnosis of this syndrome is essentially clinical, requiring either one major criterion plus genetic confirmation, two major criteria, or one major and two minor criteria. Genetic diagnosis would confirm this disease, but it is sometimes not available. It may also be used for genetic counseling [6]. It should be noted that in 20-40% of patients, the mutation occurs de novo without having a family history of the disease [9].
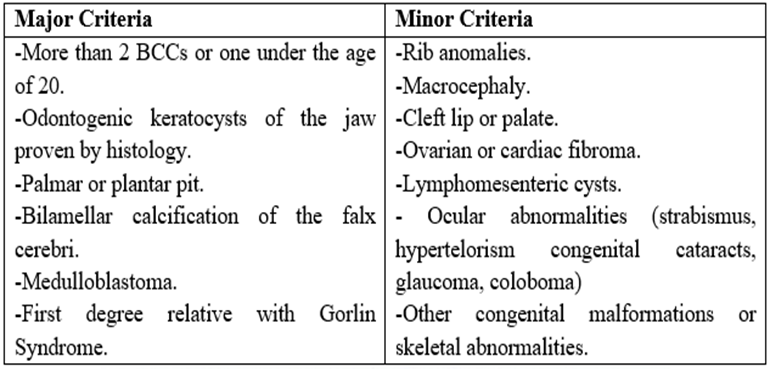
Figure 8: Diagnostic criteria for Gorlin syndrome.
It is important in these patients to avoid exposure to solar radiation and radiotherapy, as they can increase the growth of basal cell carcinomas up to years after exposure to the risk factor. This should be noted when medulloblastoma appears at an early age, as these are usually treated with radiotherapy.
Treatment must be multidisciplinary and tailored to the clinical conditions, with the treatment of choice being surgical removal of the lesions with a 4mm margin. Use of Mohs micrographic surgery is advisable for recurring tumors, or for those affecting high-risk areas such as the face. Small low-risk lesions have seen success with alternatives such as cryotherapy, curettage and electrodessication, CO2 laser, photodynamic therapy, and topical treatments such as Imiquimod cream or 5-fluorouracil cream [1,5,10].
In metastatic, locally advanced, or recurring tumors, systemic treatment with a Hedgehog pathway inhibitor, which is responsible for the pathogenesis of the disease, may be considered. For several years, Sonidegib and Vismodegib have been approved for this indication. It has been shown that oral treatment with Vismodegib 150mg/day reduces the number of new basal cell carcinomas, reduces the size of the existing ones, and reduces the need for further surgical interventions [1]. There are currently no recommendations to reduce the dosage in case of interactions, adverse side effects and intolerance. Before starting systemic treatment with Hedgehog pathway inhibitors, it is necessary to rule out pregnancy and initiate contraception [11].
The main limiting factor for the use of these treatments is their adverse side effects, which are usually moderate, but occur in most patients. Among them, muscle spasms, dysgeusia, weight loss, diarrhea, dysmenorrhea, fatigue, and alopecia stand out. Some severe side effects, present in approximately 25% of patients, are pulmonary embolisms, pneumonia, and heart failure, increasing mortality up to 11% [8,12,13]. Certain side effects can be treated or alleviated through a multidisciplinary approach involving nutritionists, rehabilitators, neurologists, dermatologists, physical therapists, and clinical pharmacologists, and can be treated with supplements, spasmolytics, and applying heat or cold. Some adverse effects are resolved several months after the start of the treatment: muscle spasms are usually decrease after 1 to 3 months of treatment, while dysgeusia and alopecia are usually resolved from half to one year later. Despite this, adverse effects are responsible for up to 70% of patients discontinuing treatment [14].
Several clinical trials have been conducted in which the effects of intermittent therapy with Vismodegib in patients with multiple basal cell carcinomas were studied, excluding locally advanced and metastatic ones not susceptible to surgical treatment or radiotherapy. This type of therapy does not interfere, according to the studies, with the efficacy of the drug, while it appears to decrease the rate of side effects and increases patient tolerance to treatment [15].
Currently, research is being conducted on topical therapy with Hedgehog pathway inhibitors. The use of LDE225 0,75% cream, in two daily topical applications, has reduced the volume of existing tumors, induced the disappearance of some and inhibiting the formation of new carcinomas, with good tolerance and fewer adverse side effects [16]. Use of topical Patidegib gel has the potential to prevent and reduce the rate of basal cell carcinomas in patients with Gorlin syndrome without causing hair loss, dysgeusia and muscle cramps [17]. Itraconazole gel 0.7% twice daily is also being studied. At this dose, this drug does not appear to have significant differences with other treatments, but it may be an effective therapy at higher doses [18].
Gorlin syndrome is a challenging. Diagnosis, management, and treatment must be included in a cohesive multidisciplinary approach. While a range of medical and surgical treatment alternatives exist for low-risk lesions, the relentless development of new tumors of poor prognosis sometimes makes systemic treatment necessary. Oral treatment with Hedgehog pathway inhibitors, which block the pathogenic source of the syndrome, allow for a new therapeutic approach, although their side effects impact their effectiveness and limit their use. Currently, new topical inhibitors of the pathway are being studied, which seem to offer a similar efficacy with fewer side effects, representing a potential new alternative for managing these patients in the near future.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
