
Case Report | DOI: https://doi.org/10.31579/2693-4779/080
1 MDS. Reader, Department of Oral and Maxillofacial Surgery, People Dental Academy, Bhopal.
2 MDS. Professor and Head, Department of Oral and Maxillofacial Surgery, People Dental Academy, Bhopal
3 Post Graduate Student. Department of Oral and Maxillofacial Surgery, People Dental Academy, Bhopal.
4 Post Graduate Student. Department of Oral Medicine and Radiology, People Dental Academy, Bhopal.
5 MDS. Professor and Head, Department of Oral Medicine and Radiology, People Dental Academy, Bhopal.
6 MDS. Senior lecturer. Department of Oral and Maxillofacial Surgery, People Dental Academy, Bhopal.
*Corresponding Author: Neha Jain. MDS. Reader, Department of Oral and Maxillofacial Surgery, People Dental Academy, Bhopal. Received date: December 22,
Citation: N Jain, Ajay K. Pillai, N Mishra, MD Ishtiyak, G.V Reddy, S Nahar. (2022). Gorlin Goltz Syndrome: A Disease in Disguise. Clinical Research and Clinical Trials. 5(3); DOI: 10.31579/2693-4779/080
Copyright: © 2022 Neha Jain, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 22 December 2021 | Accepted: 10 January 2022 | Published: 10 February 2022
Keywords: gorlin-goltz syndrome; multiple odontogenic kertocyst; basal cell nevus syndrome; nevoid basal cell carcinoma syndrome; calcification of falx cerebri
Gorlin Goltz syndrome also known as nevoid basal cell carcinoma is an autosomal dominant inherited disorder caused due to mutation in patched (PTCH) tumor suppressor gene present in the 9q chromosome. Gorlin goltz syndrome display diversified odontogenic as well as systemic manifestations. Early diagnosis and prompt treatment is mandatory to decrease morbidity and mortality. Here we present a subtle case report of a 17-year-old boy who presented with multiple odontogenic keratocysts of the mandible and maxilla which upon further examination was diagnosed as Gorlin Goltz Syndrome.
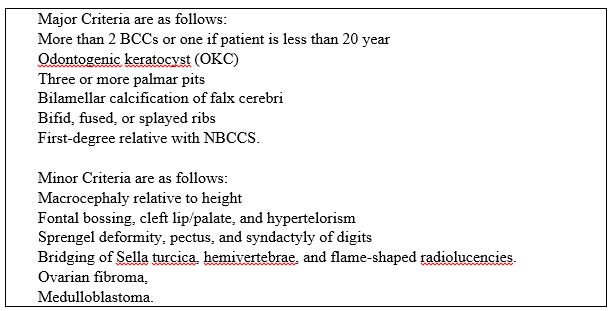
Gorlin Goltz syndrome (GGS) is an autosomal dominant disorder which was first reported by Jarish and White in 1894. [1,2] Robert J. Gorlin and Robort W. Goltz were the scientist who recognised the term Gorlin Goltz Syndrome for this disorder. The syndrome manifests with some major and minor criteria like pigmented basal cell carcinomas (BCC 50-97%), Odontogenic keratocyst (OKC 75%), palmar and/ or plantar pits (60-90%), bifid ribs (40%), ectopic calcifications of the falx cerebri (37-79%) etc [3, 4].
Gorlin goltz syndrome is caused by mutation of a tumour suppressor gene, PTCH 1 and abnormalities in the long arm of chromosome 9 (q22.3-q31) [5, 6, 7]. The gene is located on chromosome 9 (q22-q31) and its position is between D9S12 and D9S53 DNA markers. Although its incident among family members is an important diagnosing criterion, it has been found that between 20–40% of cases result from a de novo mutation of the PTCH1 gene [8].
The cause of the syndrome is a complete loss of PTCH1 gene action [9]. The protein encoded by the PTCH1 gene acts as a transmembrane receptor and contributes to the regulation of development and proliferation of stem cells in the skin, skeletal and central nervous system [9, 10]. Homozygotes to PTCH1 mutations have predispositions for such neoplasms as basal-cell carcinoma, medulloblastoma, cystic adenoidal epithelioma, esophageal and urinary bladder cancer [6, 8, 11].
The prevalence of this disorder affects all ethnic groups but occurs mostly in white patients with comparable frequency in both genders from 1/56000 [11], 1/57000 [4], 1/164000 to 1/256000 in general population. GGS is a rare condition in black people, with only 5% of the cases reported in this population [12].
This syndrome is associated with several names like basal cell nevus syndrome, nevoid basal cell carcinoma syndrome (NBCCS), multiple basal cell carcinoma (BCC) syndrome, multiple basalioma syndrome, jaw cyst basal cell tumor skeletal anomalies syndrome, jaw cyst bifid rib basal cell nevus syndrome, nevoid basalioma, odontogenic keratocysts with skeletal anomalies syndrome and fifth phacomatosis [13]. The syndrome can be diagnosed only when the first signs and symptoms appear [14]. The first and unique manifestation [6, 15] is presence of multiple odontogenic keratocysts in the jaws [16], being highly suggestive of the syndrome, even in the absence of other manifestations.
The correct diagnosis of the Gorlin-Goltz syndrome is obtained by the presence of two major criteria or two minor and one major criteria [17]. So, this study aimed to report a case with unusual clinical manifestations in a young patient with NBCCS.
Treatment for multiple cyst depends upon the size and location of the cyst. Enucleation or marsupialization of odontogenic cyst depending on the case. Follow up is mandatory for atleast 5 year.
A 17-year-old male patient reported to the department of oral and maxillofacial surgery with the chief complaint of pain and swelling in upper right and left side of the upper and lower jaws since 2- 3 months. The pain in the jaws was not continuous in nature but was aggravated on chewing. The patient had a history of visiting a government hospital 7years back with the complaint of pain and swelling in right side of face. He was examined and was found to have vestibular swelling in the posterior region of maxilla. Orthopantomogram (OPG) of the patient revealed a cystic lesion with respect to [15, 16, 17]. The provisional diagnosis of odontogenic keratocyst was made for which he got surgical enucleation of cyst present in right maxillary region.
On general physical examination, he had frontal bossing, increased fronto-occipital circumference (56 cm) [Figure 1] sparse hair at frontoparietal region, broad-square chin and multiple palmar-plantar pits were observed [Figure 2]. On extra oral examination, diffuse swelling of face was evident in maxillary region. On palpation the swelling was non tender. On intraoral examination revealed multiple missing and tilted teeth and retained deciduous tooth [Figure 3]. Bony expansion was seen from 14 to 17 region and from 24 to 26 region and in 35 to 37 region with overall poor oral hygiene and high-arched palate.



The overlying mucosa was normal without any draining sinus. The orthopantomogram (OPG) [figure 4] of the patient revealed a permanent dentition stage, multiple unilocular well defined radiolucent lesions on both sides of maxilla and mandible. Impacted teeth present on both side of maxilla and right side of mandible. Upper canine and molars were still descending toward occlusion. The computed tomography scan of skull revealed falx cerebri calcification [Figure 5]. Basal cell nevus was absent. A chest radiograph did not reveal any bifid rib.
Based on the patient’s history, clinical findings and radiological findings a provisional diagnosis of Gorlin–Goltz syndrome was made.
Differential diagnosis :-Bazex syndrome and Torre’s syndrome.


The patient later underwent marsupialization of cyst in right maxilla with extraction of 18, enucleation of cyst in left maxilla with extraction of impacted 28, cyst enucleation of cyst seen in right mandible with extraction of 48 and cyst enucleation in left mandibular premolar region. Carnoy solution was applied on enucleated cystic wall and iodoform dressing was given in marsupialized cavities which were repeated changed once in 5 days. [figure 6]. The root canal treatment was planned for tooth which were associated with the cystic lining. The enucleated cystic lining was sent for histopathological examination.

The histopathologic examination revealed a cystic lining of corrugated parakeratinized stratified squamous epithelium, basal layer showing palisading nuclie, stroma with inflammatory infiltrate containing plasma cells and eosinophils [Figures 7].

All four lesions were diagnosed as odontogenic keratocysts with parakeratotic nature. Final diagnosis of Gorlin–Goltz was confirmed based on two major (multiple OKCs and calcification of falx cerebri) and minor criteria (frontal bossing). The patient is being followed up at 3 months interval, soft-tissue healing was satisfactory, and the patient’s OPG revealed new bone formation around periphery of the cyst. [Figure 8]

The Gorlin-Goltz syndrome is an autosomal dominant inherited syndrome manifested by multiple defects involving the skin, nervous system, eyes, endocrine system, and bones [18]
Diagnosis of GGS is cumbersome as it exhibits variability and at different ages its presentation is different [19]. Early diagnosis of GGS is important as it development into malignancies such as medulloblastoma and aggressive skin cancers is high [20]. According to Kimonis, diagnosis can be established only when two major, or one major and two minor criteria are present [21].
Manfredi et al. declares that the diagnosis of the Gorlin- Goltz syndrome initially consists in the triad of basal cell carcinomas, odontogenic keratocysts, and skeletal anomalies.
Sahu et al. [22] reported familial inheritance of this disorder in mother and daughter. The GGS is an autosomal dominant disorder, so follow-up of other family members is also warranted for early detection of BCC and GGS. The aim of this study is to draw attention to the fact that OKC is the major presenting manifestation of this syndrome.
The treatment for KCOT depends on age; size, extent and location of the lesion; and possible perforation of the cortical bone lamellae or soft tissue infiltration. The treatment modality may be divided into conservative, aggressive and radical. Conservative treatment consists of enucleation of tumour when the lesion is small, it is not involving vital structures and the tumour is well within the confines of bones [23, 24]. Aggressive methods include peripheral ostectomy, chemical curettage with Carnoy’s solution and resection [25] Application of Carnoy’s solution following cyst enucleation and cryosurgery is new regime followed to destroy epithelial remnants and dental lamina within the osseous margin and thus prevent recurrences [26]. En-bloc resection of odontogenic keratocysts is advised when cyst has reoccured inspite of previous enucleation with an adjunctive procedure, multilocular cystic lesion and cysts exhibiting aggressive clinical behaviour that should require resection as the initial surgical treatment [25, 26]. According to Khaliq et al, KCOT is a frequent manifestation of GGS and can be its first sign. Among seven patients assessed from 2004 – 2015, there were 15 primary and two recurrent lesions. In children, conservative management is considered, because an aggressive modality can affect tooth eruption and development of the involved jaw [25]. Although multiple OKCs can occur as a part of some rare dermatological syndromes, such as Bazex syndrome or Torre’s syndrome, our patients had no features suggestive of these syndromes [27].
The recurrence rate after excision of KCOT is high, ranging from 12% to 62.5% owing to thin fragile lining and presence of satellite or daughter cells [28]. Regular monitoring once in a year is mandatory for all patients to check for reoccurrences.
In our case the patient reported with multiple cysts in the jaw for which enucleation was done and the specimen was sent for histopathological investigation. The histopathological confirmed OKC and the patient being under 20 years old and other clinical and radiological findings further confirmed our diagnosis. A multidisciplinary approach was planned for the definitive treatment for the patient where the multiple cysts were enucleated and involving tooth buds were removed. The teeth involved were to undergo Root canal treatment. The patient is also being kept on regular follow-up to look for any chances of recurrence of the cysts as the literature suggests the patients with GGS are more prone to such recurrences.
The presence of three major signs (multiple odontogenic keratocytes, palmer plantar pits and calcified falx cerebri) and one minor signs (frontal bossing) confirmed the diagnosis that our patient has GGS. There needs to be multidisciplinary approach in treating such cases. Intervention is required from various departments including Oral and maxillofacial surgery, endodontics, and dermatologists to ensure prompt treatment. Patients suffering from Gorlin–Goltz syndrome should not have excessive sun exposure, as it triggers the formation of basal cell carcinoma. Periodic follow‑up is important in these patients, as OKC tends to reoccur if it is parakeratotic in nature. Regular follow up at weekly intervals is mandatory followed by regular intervals of six months for 5 years to monitor recurrences and any further complications.
No Funding received
Authors have no conflicts of interest
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
