
Review Article | DOI: https://doi.org/10.31579/2640-1045/116
1 Endocrinology Sector, Central Laboratory of the Dr. Oscar Alende Interzonal General Acute Hospital, Mar del Plata, Bs As, Argentina.
2 Central Laboratory, Clinic and Maternity Colon, Mar del Plata, Bs As, Argentina.
3 Endocrinology Service of the Hospital General de Agudos Dr. Teodoro Álvarez, Bs As, Argentina.
*Corresponding Author: Belloni J, Endocrinology Sector, Central Laboratory of the Dr. Oscar Alende Interzonal General Acute Hospital, Clinic and Maternity Colon, Mar del Plata, Bs As, Argentina.
Citation: Belloni J and Tapper X. (2022). Glp-1 Analogs for the Treatment of Obesity and Diabetes. Endocrinology and Disorders, 6(2); DOI:10.31579/2640-1045/116
Copyright: © 2022, Belloni J. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 16 January 2022 | Accepted: 26 March 2022 | Published: 25 April 2022
Keywords: diabetes; obesity; incretins; incretin effect; GLP-1 analogs
Currently the prevalence of obesity and diabetes is increasing throughout the world. The unsatisfactory long-term results observed in the treatment of both are due to their complex pathophysiologies and the difficulties related to maintaining lifestyle changes. From the knowledge of the incretin effect and its alteration in patients with type 2 diabetes mellitus, GLP-1 receptor agonists arise, molecules with high structural homology with native GLP-1. Scientific evidence supports its use for the long-term treatment of diabetes, especially in the presence of associated cardiovascular and/or renal failure. In 2009, the use of liraglutide for patients with diabetes was approved in Europe, and in 2014 it was signed for the first time in the United States to treat obesity, since it was observed that the use of these drugs causes significant weight loss.
Diabetes is a chronic disease in continuous growth worldwide. Type 2 diabetes mellitus represents 90% of cases and its frequency is similar to that of obesity. The latter currently affects more than 600 million people worldwide and is associated with more than 45 comorbidities, in addition to the atherogenic affectation that makes up the metabolic syndrome. Obesity is one of the main causes of insulin resistance and can progress to type 2 diabetes [1,2]. Lifestyle modifications continue to be the first-line treatment for obesity, although they have been shown to only confer modest benefits [3].
Incretins are hormones secreted by enteroendocrine cells upon nutrient intake. They stimulate insulin secretion by pancreatic β cells in a glucose-dependent manner. In the search for pharmacological therapies, incretin analogs have emerged with proven benefits in improving blood glucose, weight loss, and cardiovascular outcomes [4.5].
This monograph aims to present the usefulness of GLP-1 analogs for the treatment of patients with diabetes and obesity based on the most relevant clinical trials published to date.
Intestinal hormones act on various tissues involved in the control of intestinal function, insulin secretion, nutrient assimilation and food intake [6]. In 1903 Moore et al, described the presence of “a substance of a hormonal nature or secretin, produced by the duodenal mucosal membrane that would be absent in diabetic patients”. GIP (glucose-dependent insulinotropic polypeptide), the first incretin, was found in 1973, and GLP-1 (glucagon-like peptide 1) was discovered in 1987. In 1979, Creutzfeldt defined the criteria for classifying a substance as incretin: gastrointestinal factor, involved in nutrient metabolism that should stimulate insulin secretion in a glucose-dependent manner at physiological levels. To date, GIP and GLP-1 are the only ones that meet these criteria [4].
Physiology of incretins
GIP is produced by K cells in the mucosa of the duodenum and upper jejunum. It is synthesized as a precursor propeptide (pro-GIP), which is then cleaved into GIP by post-translational processing. It not only accelerates insulin secretion under hyperglycemic conditions, but also stimulates glucagon secretion under hypoglycemic conditions. The binding of GIP to its receptor called GIP-R, with seven transmembrane domains coupled to guanine nucleotide binding protein, leads to the activation of adenylate cyclase and an increase in cyclic adenosine monophosphate (cAMP), with the consequent activation of protein kinase type A (PKA). GIP-R is expressed in pancreas, intestine, heart, adipose tissue, and brain [6].
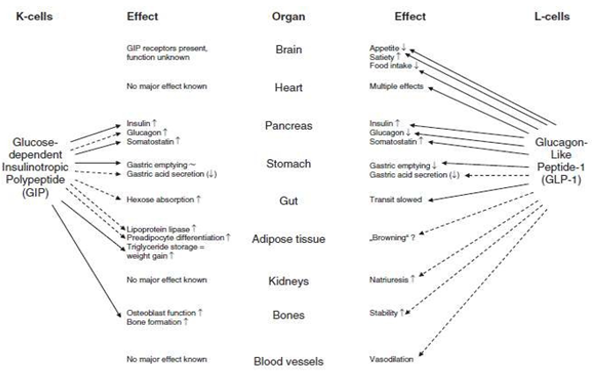
GLP-1 was identified as part of the gene sequence encoding pro-glucagon, which is expressed on L cells in the small and large intestine. Processing of pro-glucagon in intestinal L cells results in the formation of glucagon, GLP-1, and GLP-2 (an intestinal growth factor). The GLP-1 molecule is converted into an active molecule by the effect of proconvertase-1. The GLP-1 receptor is expressed in the intestine, pancreas, brainstem, hypothalamus, and vagal afferent nerves. It is also a G protein-coupled receptor that triggers the same intracellular signaling pathway as the GIP-R. The actions of GLP-1 include activation of the ileal brake, delayed gastric emptying, increased glucose-dependent insulin release, decreased glucagon secretion, and increased pancreatic β-cell growth. GLP-1 decreases food intake, possibly through direct vagal and central pathways, mediated specifically by GLP-1 receptors [5,6]. The secretion of GLP-1 occurs almost in parallel with the secretion of GIP, this indicates that there would be signals sent by the nervous system autonomic gut that trigger the release of GLP-1. It should be noted that incretins also have some other additional biological effects [7]. (Figure 1)
Endogenous GLP-1 and GIP have a short plasma half-life: 1 to 7 minutes and are rapidly metabolized and inactivated by the enzyme DPP-4 (Dipeptidyl peptidase – 4). This ubiquitous enzyme is present in the circulation and is expressed on the surface of most cell types [8].
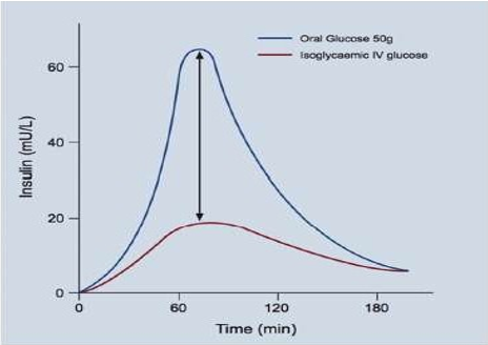
Oral glucose leads to greater stimulation of insulin secretion than intravenous infusion even when the same plasma glucose concentration profiles ("isoglycemia") are achieved. This phenomenon is called the incretin effect and is attributed to the release of GIP and GLP-1 from enteroendocrine cells in response to oral glucose intake, while intravenous glucose does not (Figure 2). The contribution of incretin hormones to insulin secretory responses after oral glucose administration depends on the dose used and can vary between 25% and 75%. These hormones increase within minutes of nutrient intake and act on the islets of Langerhans to increase insulin secretion and decrease glucagon secretion when plasma glucose concentration is greater than approximately 6 mmol/L [7,9].
Incretin effect in people with Type 2 Diabetes
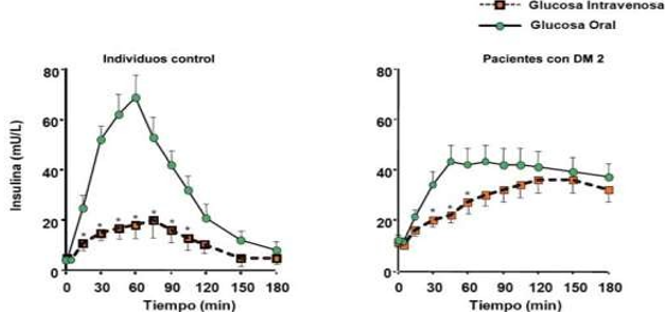
In people with type 2 diabetes, the incretin effect is greatly reduced or absent compared to healthy subjects (Figure 3). The question then arises: Does the decrease in the incretin effect precede and potentially promote the development of diabetes? Or is it a consequence of the diabetic state? Numerous studies have proposed that this defect occurs after the diagnosis of diabetes. Indeed, in patients with chronic pancreatitis, the reduced incretin effect is seen only in those who also develop diabetes and not in those who do not. Studies with intensive insulin therapy suggest that reduction of hyperglycemia would improve but not normalize the insulinotropic activity of GIP and GLP-1 in type 2 diabetes. In addition, it is believed that the inability of the endocrine pancreas to respond to GIP could contribute to the progression of diabetes. The loss of this physiological mechanism would further deteriorate glycemic control, giving rise to a vicious circle by worsening glucotoxicity that can induce a reduction in β-cell mass, the functional capacity and expression of GIP receptors, and the incretin effect [10-12].
Given the decrease in the incretin effect in type 2 diabetes, pharmacological therapies based on incretinomimetics have been developed. On the one hand, DDP-4 inhibitors that act by increasing the levels of active incretin hormones by inhibiting the enzyme that physiologically inactivates them. On the other hand, GLP-1 analogs act by stimulating GLP-1 receptors. Both are recommended as second-line treatment for type 2 diabetes [11].
Since meal-stimulated GIP concentrations were similar in people with and without type 2 diabetes while GLP-1 concentrations were reduced in type 2 diabetes, treatment strategies were targeted at GLP-1. Recent clinical studies have identified potential benefits of GIP in combination with GLP-1 [13].
Currently, the American Diabetes Association recommends the use of GLP-1R agonists in patients with type 2 diabetes at risk of atherosclerotic cardiovascular disease, heart failure, or established kidney disease [24].
Regarding obesity, randomized studies have shown that greater initial weight loss achieved with lifestyle changes associated with pharmacological strategies improves long-term weight maintenance. The relationship between energy intake and expenditure is modulated not only by environmental and behavioral factors, but also genetic and hypothalamic-regulated neuroendocrine feedback mechanisms. It integrates peripheral hormonal signals from the gastrointestinal tract (ghrelin, cholecystokinin, peptide YY, pancreatic polypeptide, GLP-1), pancreas (insulin), and adipose tissue (leptin). There are molecules that stimulate appetite (central orexigenic effect) such as neuropeptide Y (NPY) and agouti-related peptide (AgRP) and others that suppress appetite (central anorexigenic effect), for example alpha-melanocyte-stimulating hormone (α- MSH), a peptide derived from pro-opiomelanocortin (POMC) and the cocaine and amphetamine regulated transcript (CART). In animal studies, GLP-1 directly stimulates POMC/CART neurons and indirectly inhibits neurotransmission in NPY- and AgRP-expressing neurons through ϒ-aminobutyric acid (GABA)-dependent signaling. These findings indicate that GLP-1 receptors on POMC/CART-expressing arcuate nucleus neurons likely mediate weight loss induced by exogenous GLP-1 analogs [14].
DPP-4 enzyme inhibitors
DPP-4 inhibitors are orally available low molecular weight drugs that rapidly and specifically inhibit DPP-4 activity. The most commonly used are sitagliptin, vidagliptin, and saxagliptin. These have few side effects, improving active GLP-1 and GIP levels 2-3 times after a meal, and also appear to have similar glycemic efficacy: a modest (0.5-0.8%) reduction in HbA1c. The risk of hypoglycemia with DPP-4 inhibitors is low given their GLP-1 mediated glucose-dependent mechanism of action [8].
GLP-1 analogs
The GLP-1 analogs present in our country are liraglutide, semaglutide and dulaglutide. In routine clinical practice, we could classify them as those administered daily, such as liraglutide, or administered weekly, such as semaglutide and dulaglutide [8]. The most commonly used GLP-1 analogs are listed below:
Liraglutide. It shares 97% homology with native GLP-1, but unlike
the latter has a half-life of 13 hours. It was first approved for the treatment of type 2 diabetes in Europe in 2009 and it was only in December 2014 that the 3.0 mg dose of liraglutide was first signed up for the treatment of obesity in the United States of America [14,15].
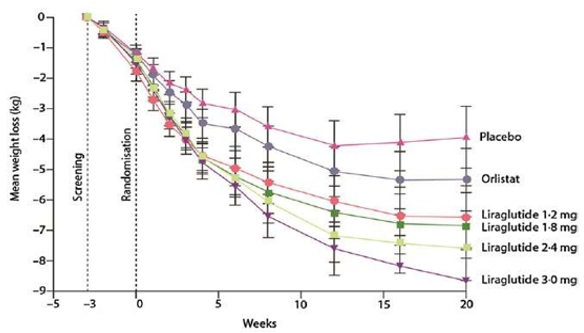
Regarding its effect on weight loss, Mancino et al. in a 20-week trial it compared liraglutide versus orlistat versus placebo. Orlistat is a potent, specific, and long-acting inhibitor of gastrointestinal lipases approved for the treatment of obesity. Patients (n = 564, BMI 30-40 kg/m2) were assigned to the following doses of liraglutide: 1.2; 1.8; 2.4 and 3.0 mg (n = 90-95) or placebo (n = 98) administered once daily subcutaneously or orlistat (n = 95) 120 mg 3 times daily orally. As shown in Figure 4, liraglutide induced significantly greater weight loss than placebo (P = 0.003 for liraglutide 1.2 mg and P < 0 xss=removed xss=removed xss=removed xss=removed>
On the other hand, human studies have shown that endogenous GLP-1 has positive effects on blood pressure (BP) and on endothelial function in patients with type 2 diabetes. These have been confirmed with GLP-1 receptor agonists (GLP-1A). They not only improve glycemic control, lipid profile, BP, and weight, but also cardiac function and ischemia, resulting in the prevention or delay of the atherosclerotic process. Although Buen et al. maintain that this atheroprotective role would be through the modulation of macrophage activity, the exact mechanisms are not yet fully elucidated [16,17].
In 2016, one of the most relevant CVOT studies (in English: Cardiovascular Outcome Trial) on the subject was published: LEADER, in which 32 countries participated. It was multicenter and randomized. It included 9340 patients with DM2 and high cardiovascular risk. Liraglutide 1.8 mg/day (or the maximum tolerated dose) was compared with placebo. Patients were followed for 3.8 years and demonstrated a 13% reduction in the risk of major adverse cardiac events (MACE), reduction in HbA1c, body weight, and hypoglycemia. There were no significant differences in hospitalization for heart failure or the development of pancreatitis. It showed a reduction in the risk of mortality from cardiovascular causes by 22% and was well tolerated, although it was associated with mild gastrointestinal disorders [18]. The most common side effects were nausea and diarrhea. These appeared in the first weeks of treatment and were related to the dose (Figure 5). To avoid them, it is recommended to start with 0.6 mg/day and increase by 0.6 mg daily each week until reaching a daily dose of 1.8 mg in people with type 2 diabetes or 3 mg/day for obesity treatment [18].

Semaglutide
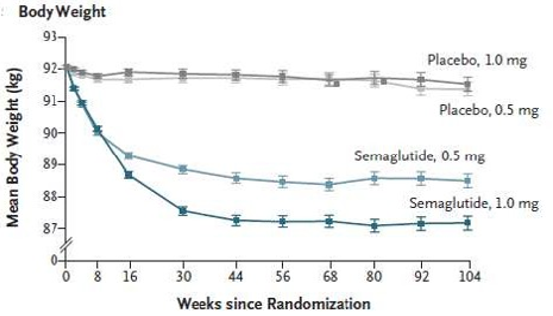
It shares 94% homology with native GLP-1. present a life longer median than liraglutide. Modifications of its chemical structure compared to endogenous GLP-1 include two amino acid substitutions at position 8 (alanine for alpha-amino isobutyric acid) and 34 (lysine for arginine), and also acylation of lysine at position 26 with a "linker" composed of a glutamic acid moiety and a C-18 fatty diacid side chain. Substitution at position 8 makes it resistant to degradation by DPP-4, and the linker promotes its binding to albumin, extending its half-life to about 1 week. In 2016, a trial was published to assess long-term cardiovascular outcomes with semaglutide in subjects with type 2 diabetes (SUSTAIN-6). 3,297 type 2 diabetic patients from 20 countries were given semaglutide once weekly (0.5 mg or 1.0 mg) versus placebo for 104 weeks [20,23]. In relation to body weight, at week 104 and compared with the placebo group, those who received 0.5 mg semaglutide presented a decrease of 2.9 kg and those who received 1 mg the decrease was 4.3 kg (Figure 6). Regarding cardiovascular outcomes, in SUSTAIN-6, semaglutide demonstrated a 26% reduction in MACE, 39% in the development of stroke, and 26% in the occurrence of cardiovascular events at 2 years, when added to standard treatment. In addition, a 36% reduction in the risk of progression or new onset of kidney disease was observed [20]. Finally, gastrointestinal disorders were more frequent in the semaglutide group. Nausea, vomiting and diarrhea were the most observed [20].
Dulaglutide
It comprises two molecules of modified GLP-1 covalently linked to a immunoglobulin G (IgG) heavy chain molecule, has a half-life of 5 days and is administered subcutaneously in weekly doses of 0.75 mg or 1.5 mg. It is currently used in several countries of the European Union and the United States [16, 21].
In 2019, the REWIND study designed to assess whether the addition of dulaglutide to the diabetes medication regimen in adults with T2DM safely reduces the incidence of cardiovascular outcomes compared to placebo was published. This trial lasted 3 years, 24 countries and 9901 patients with DM2 participated. In it, one group received a weekly injection of 1.5 mg of dulaglutide and the other group a placebo. The findings show that dulaglutide reduces cardiovascular events and this could be due to the reduction in HbA1c levels, LDL cholesterol, BP and weight. Evidence also suggests that these drugs could enhance endothelial cell responses to ischemia, attenuate the progression of atherosclerosis, vascular inflammation, and vasoconstriction [21].
REWIND demonstrated a significant reduction in MACE-3 (nonfatal acute myocardial infarction, nonfatal stroke, and cardiovascular mortality) of 12%. In REWIND only 32% of the individuals studied had established cardiovascular disease [21]. In this way, dulaglutide would be the first GLP-1 analogue to demonstrate cardiovascular benefit in a population without already established cardiovascular disease (unlike the LEADER and SUSTAIN-6 studies). From there arises the possibility of using it for primary cardiovascular prevention in type 2 diabetes. Regarding the treatment of obesity, its use has not yet been approved for it.
There is a strong association between obesity and type 2 diabetes. Establishing healthy eating habits and physical activity substantially improve short-term health, but the long-term success rate is low given the complex pathophysiology involved and the difficulty in maintaining changes in lifestyle. From the discovery of incretins and their decrease or absence in diabetic patients, therapeutic strategies arise in this area. There is extensive scientific evidence on the benefit of the use of GLP-1 analogs, mainly liraglutide, semaglutide, dulaglutide and exenatide (the latter is currently not available in Argentina) for the treatment of obesity and diabetes. CVOT multicenter studies such as LEADER, SUSTAIN-6 and REWIND, confirmed that the benefits of long-term use of these drugs are mainly at the cardiovascular and renal levels. They reduce HbA1c levels, arterial hypertension and regulate dyslipidemia. They also decrease platelet aggregation and thrombosis while increasing myocardial contractility. On the other hand, they slow gastric emptying and appetite, increase insulin sensitivity, and decrease gluconeogenesis. The American Diabetes Association (ADA) recommends the use of these GLP-1R agonists in patients with DM2 and existing cardiovascular and renal failure. Liraglutide is approved in our country for use in type 2 diabetes and obesity. Semaglutide and Dulaglutide only for type 2 diabetes, although semaglutide has recently been approved in the United States for the treatment of obesity.
Finally, it is necessary to highlight the necessary role of the clinical analysis laboratory not only in the diagnosis of diabetes, but also in the dosage of biochemical markers that allow monitoring the evolution of patients under pharmacological therapy with incretin analogs.
GIP: glucose-dependent insulinotropic polypeptide
GLP-1: Glucagon-like peptide-1
DPP-4: Dipeptidyl peptidase enzyme – 4
GIP-R: Glucose-dependent insulinotropic polypeptide receptor
GLP-1R: Glucagon-like peptide receptor-1
cAMP: Cyclic Adenosine Monophosphate PKA: Protein Kinase A
BMI: Body Mass Index BP: Blood Pressure
LDL: Low density lipoprotein
HbA1c: Hemoglobina glicosilada A1C
GLP-1A: Análogo del péptido similar al glucagón-1
DM2: DiabetesMellitus tipo 2
IgG: Inmunoglobulina G
REWIND: Researching Cardiovascular Events with a Weekly Incretin in Diabetes
EXCEL: Effectsof Once-Weekly Exenatideon Cardiovascular Outcomes in Type 2 Diabetes
HDL: High density lipoprotein
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
