
Short Review | DOI: https://doi.org/10.31579/2640-1053/027
*Corresponding Author: Saritha Garrepalli, Department of Pharmaceutical Sciences, India.
Citation: Saritha Garrepalli, Global Patterns of Lung Cancer Incidence. J Cancer Research and Cellular Therapeutics, Doi:10.31579/2640-1053/027
Copyright: © 2018 Saritha Garrepalli. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 30 March 2018 | Accepted: 15 April 2018 | Published: 24 April 2018
Keywords: lung cancer; survival rate; epidemiological pattern
Introduction
It is well known that smoking is injurious to health which causes lung cancer. Although not all smokers develop lung cancer, fraction of lifelong non-smokers will die from lung cancer. Lung cancer is a major cause of cancer related death in developed countries with extremely poor overall survival rate. In present study we set out epidemiological pattern with clinical profile of lung cancer patients in northern india population.
Aim:We evaluate the effect of smoking with age distribution on histopathology in lung cancer patients.
Material & Methods: We enrolled 218 patients after confirmation of histopathology and also collected demographic data.
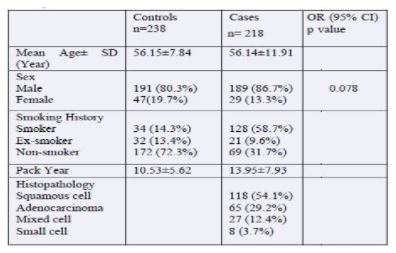
Results: Out of 218 patients of lung cancer, having median age of 56 years, we found 149 (68.3%) were smokers and 69 (31.6%) were nonsmokers. In histopathology 54.1% patients had squamous cell carcinoma, 29.2% adenocarcinoma, 12.4% Mixed cell, 3.7% Small cell. We also found 63.1% smoker to have squamous cell carcinoma and 50.7% non-smoker have adenocarcinoma.In our study middle age group patients were more frequent in smoking group. While higher age group patients has squamous cell and middle group have adenocarcinoma. Therefore patients group with high smoking are found to develop have more risk to develop small cell carcinoma rather than in case of non-smoker higher age groups have sqamous cell carcinoma type.
Conclusion: In this study we found middle age group subjects of smoker having more squamous cell and nonsmoker having adenocarcinoma.
Lung cancer mainly develops by tobacco usage and this is often viewed solely as smoker disease. However, a significant number of patients with lung cancer have no smoking history. Globally approx 1.61 million new cases of lung cancer occur per year, with 1.38 million deaths. This data on cancer patients with lung cancer is a major cause of morality in all over cancer [1]. In india, approxmately 63,000 new lung cancer cases are reported each year [2].
The major risk for developing lung cancer in tobacco use and this disease is often viewed solely as a smoker disease.although multiple risk factors, including environmental,hormonal, genetic and viral have been implicated in the pathogenesis of lung cancer in never-smokers, no distinct eiological factor has emerged that can explain the relatively high incidence of lung cancer in never smokers and the marked geographic difference in gender proportions. Molecular studies, in particular of the TP53, KRAS, and epidermal growth factor receptor (EGFR), GST genes, demonstrate strikingly different mutation pattern and frequencies in lung cancer patients in non-smoker and smokers [3]. In our study, we set to find out clinically meaningful difference between smoker and non smokers, in relation with lung cancer development
It is an observational study, in which we collect data through screening of patients from OPD through diagnosis of lung cancer patients, discussed in the thoracic oncology multidisciplinary meeting at a tertiary care hospital in Lucknow, India, during a 2 year period. The survey was conducted by trained clinical research coordinators under the supervision of physicians using a detailed questionnaire. Patients were interviewed regarding their history of smoking, smoking pattern and use of smokeless tobacco. Following the interview, all patients underwent the routine work-up for lung cancer, including imaging (computed tomography (CT) scan of the thorax and upper abdomen) and pathologic confirmation of the diagnosis. The final therapy plan was noted. Data was entered and analyzed using SPSS software (SPSS for Windows, Version 15).
In the present study 218 patients diagnosed according to histopathology between November 2007 and November 2009. A summary of the patient data is provided in [Table 1].
Smoking status
Out of 218 patients, 128 patients (58.7%) have smoked, 21 (9.6%) ex-smoker and 69 (31.7%) non-smokers. Patients had smoked both cigarettes and beedis. Pack Year 13.95 ± 7.93 Years.
Sex
Out of 218 patients, there were 189 (86.7%) males and 29 (13.3%) females i.e. a male: female ratio of approximately 8.6:1.4.
Risk analysis of carcinogen eOut of 218 patients, Smokers have 63.1 % smokers squamous cell, 20.1
Age
The median age of the patients in our study was 56 years (S.D=11.91) with a range from 30-80 years. The median age of non-smokers were significantly lower than that of smokers (53 versus 59 years, P<0>
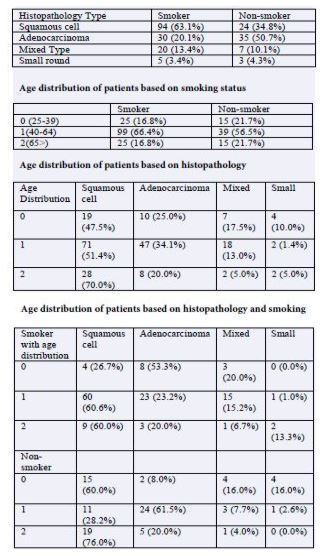
Age distribution of patients based on histopathology and smoking
small round, In age group (40-64), 60.6% squaomas cell, 23.2
Relating to measured time in cancer histology are often difficult to study because changes in diagnosis or classification may mimic true changes in disease occurrence [4,5]. In a study from Singapore, 32.5% of lung cancer patients has been never-smokers, [6] while in the United States, approximately 10% of lung cancer cases occur in non-smokers [7].
Over the earlier periods distribution of NSCLC pathology has been modified. Squamous-cell carcinoma was the most common histological type of NSCLC, however, since about 1975, there has been a dramatic increase in the incidence of adenocarcinoma, making it the predominant histological subtype of NSCLC [8]. Thus far, not much information was available as to the distribution of the histological subtypes in India. Squamous-cell carcinoma was still the predominant histological subtype of NSCLC [9]. In our study we found that squamous cell carcinoma accounts for (54.1%) of NSCLC, while only (29.2%) are adenocarcinoma.
Conventionally, Squamous-cell carcinoma of the lung was thought to be smoking-related, rather than adenocarcinoma. The increase in the incidence of adenocarcinoma was thought to be mainly attributable to a change in smoking pattern and an increased preference for filter cigarettes that have low tar, but high nitrate content [10]. Earlier studies reported that the increased incidence of adenocarcinoma was confined to smokers [11,12]. In contrast, we found a statistically higher occurrence of adenocarcinoma in non-smokers as compared to smokers. This is supported by other studies in the literature [13-16]. Thus, our study and other recent studies suggest that the increase in adenocarcinoma is not solely due to a change in pattern of cigarette smoking, but must be due to non-smoking-related factors, since the increase is demonstrated in non-smokers as well.
Bidi are more carcinogenic than cigarettes [17], however, it is not known if bidi smoking preferentially causes a particular cancer subtype or if there are any clinical or pathological features that are different in a lung cancer caused by bidi smoking as compared to that caused by regular cigarette-smoking. Among our patients with a history of smoking, the proportion bidi smokers (25.4%) were higher than the so-called "safe" cigarettes (19.4%). Given the wide prevalence of bidi smoking in our country, this may be an important factor to consider while evaluating the Indian epidemiologic profile. Whether there were any significant differences between cancers in bidi smokers compared to that in cigarette smokers is beyond the scope of this study.
In this we found that squamous cell carcinoma is higher in in northern Indian population rather than adenocarcinoma, and it also confirmatory statement that smoker having more squamouse cell and nonsmoker having adenocarcinoma in the middle age group.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
