
Case Report | DOI: https://doi.org/10.31579/2643-6612/026
1 Clinical Associate Professor, Herman Ostrow School of Dentistry of USC and Private Practice, Los Angeles, CA.
2 International Institute of Periodontology, QC, CN.
3 DDS - Private practice, Silver Spring, Maryland, USA.
4 Private Practice, Los Angeles, CA.
*Corresponding Author: Gregori M. Kurtzman, DDS - Private practice, Silver Spring, Maryland, USA.
Citation: A Aalam, M Bonner, A Krivitsky, Gregori M Kurtzman, Madison K Zusman. (2022). Gingival Parasitic Infections as a Contributor to Periodontitis: Identification and Treatment. Dentistry and Oral Maxillofacial Surgery. 5(1); DOI: 10.31579/2643-6612/026
Copyright: © 2022 Gregori M Kurtzman, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 26 October 2021 | Accepted: 27 December 2021 | Published: 05 January 2022
Keywords: gingival parasites; entamoeba gingivalis; periodontal disease; bonner method
Objectives: Parasites play a role in the pathology of periodontal disease with the protozoan Entamoeba gingivalis frequently observed when periodontal disease is present and has been ignored as a contributor to periodontal disease. Identification of the presence of periodontal parasites and how to treat them to eliminate their contribution to periodontal disease will be addressed.
Methods: The first phase of therapy is reconstituting a normal commensal biofilm with minimal supragingival calculus removal to limit potential for the parasites to invade the soft tissue lining of the pocket and potentially spread related to the bleeding capillaries. At the fourth month, a systemic antiparasitic medication (metronidazole) is added. The second phase of therapy consists of four monthly subgingival calculus removal using sonic or ultrasonic instruments. Microscopic evaluation is used to confirm the absence of parasites.
Results: The Bonner Method is nonsurgical. Pocket closure and osseous regrowth, without supplemental grafting help confirm healing and continued use of the homecare regime allow the patient to maintain gingival health long-term. Microbiota microscopic examination at every visit during active treatment confirms healing and elimination of the parasites.
Conclusions: Patient who have traditionally avoided dental treatment or have experienced traditional surgery in the past easily accept antiparasitic treatment, which is reached from clinical and microscopic co-examination. Many of these patients are seeking an alternative to traditional surgery and are more comfortable with the basics behind the protocol once they have seen their biofilm under video from their microscopic sampling.
Clinical significance: The subject of this article has clinical relevance, as parasites are an unrecognized contributor to periodontal disease that is frequently not identified or understood. This article discusses its clinical relevance, how to identify its presence and treatment to eliminate the parasite as part of periodontal treatment. The authors feel that this will have relevance to dental hygienists as they are the practitioner who would be first to identify its presence and provide treatment in the dental practice.
Parasitic infections are often overlooked with the identification of periodontal disease and may hamper effective treatment unless identified and properly treated.
Introduction
The oral cavity hosts a complex microbiome consisting of bacteria, parasites, fungi and viruses. Bacteria are the prime cause of periodontal disease as well as dental caries [1]. The oral microbiome of each person is quite distinct. Patient genetics and peripheral factors lead to variations in each patient’s own oral microbiome. Commensalism and coexistence between the host and those microorganisms form a homeostasis in their oral microbiome which is preserved under healthy conditions. Nonetheless, under some conditions, a parasitic relationship dominates the existing situation, and the rise of cariogenic microorganisms results in dental caries [2].
Parasites may play an important role in the pathology of periodontal disease. The protozoan Entamoeba gingivalis is frequently observed in periodontal pockets. (Figure 1) This species of parasite is closely related to the human pathogen Entamoeba histolytica. Although E. gingivalis is highly enriched in people with periodontitis, the potential role of this protozoan in oral infectious diseases is not well known. Inflammation is always present in periodontitis, with the recruitment of leukocytes to inflamed gingival tissue and their passage to the periodontal pocket lumen are speculated to cause both tissue destruction and the development of the flora found withian the pocket. The contribution to periodontal disease for each bacterial species is difficult to establish and the role of parasite in the disease process has been ignored [3]. The ethiology of periodontal disease has never been completely understood. However, a loss of the balance between the microbial virulence of periodontal pathogens and the hosts immune system may be considered a trigger for periodontal disease and the severity patient to patient. The immune system when activated by microbiological agents, attacks the host causing the destruction of periodontal tissue, and alveolar bone.

A analysis has been reported demonstrating an increased frequency of E. gingivalis in inflamed periodontal pockets, where it contributed the second-most abundant rRNA following human rRNA [4, 5]. They reported that with histochemical staining of gingiva that had severe chronic periodontitis, the presence of E. gingivalis in conjunction with abundant neutrophils was identified. It was shown that on disruption of the epithelial barrier, E. gingivalis was able to invade gingival tissue, where it moved and fed on host cells. Additionally, they were able to detect the parasite in 77% of inflamed periodontal sites and 22% of healthy sites, with 15% of healthy gingiva colonized by E. gingivalis. E. gingivalis strong virulence potential showed the mechanisms of tissue invasion and destruction are similar to the colonic protozoan parasite E. histolytica. The colonization of Entamoeba into the inflamed periodontal sites and the known resistance to neutrophils, antimicrobial peptides, and various antibiotics, are an underrated microbial driver of the destructive forms of periodontitis [6, 7]. However E. gingivalis is infrequently found in people without periodontal disease and there is evidence that E. gingivalis could favor the onset and progression of periodontal disease [8].
Is Periodontitis a Parasitic Infection?
Lyons reported after monitoring crevicular biofilm sulcus of his patients by microscopic observation for more than 20 years, evidence of invasion of the gingival periodontal sulcus by the parasite E. gingivalis. He further reported that parasites were found in all cases of active periodontitis. These were nourished by live white blood cell nuclei as well as red blood cells and a substantial clinical improvement was obtained by elimination of these parasites from the periodontal pockets [9, 10]. Oral parasites were found in a constant manner in active diseased sites. He concluded that despite the assumption that E. gingivalis is commensal, evidence demonstrated that this is an aggressive pathogen. The vast majority of patients affected by periodontal disease are infected with oral parasites and that removal of this protozoa is followed by “arrest of the disease and its resolution, including bone regeneration” [11]. Trichomonas tenax, although less frequently present, is associated with severity of periodontal disease and has recently been considered a pathogen similar to T. vaginalis [12]. In the same manner, Keyes reported 100% parasite presence on 7mm pocket and none in health or gingivitis in a 52 patients paper report [13].
Bonner, in the 1990s, using a clinical microscope and medical treatment began treating periodontitis in those cases that were not responding to traditional periodontal treatment. He noticed following SRP , the patient microbiome remained unaltered with parasites still present as well as many of the bacteria noting orange and red complexes of Socransky (Figure 2) [14]. Patient practicing good homecare were not able to affect the presence of the parasites present periodontally. This resulted in development of the parasite-medical protocol that change a periodontitis biofilm to a healthy biofilm. This green complex, is mainly composed of non-motile cocci and filaments without WBC. A retrospective study in 2013 of five clinics using this anti-parasitic protocol, examining 624 patients with chronic and aggressive periodontitis. Based on a 6 points survey charting per tooth where a pocket depth of 3 mm or less is considered normal, he reported a 95.7% success rate in pocket elimination after anti-parasitic periodontal treatment and microscopic monitoring [15].

It is becoming increasingly clear that periodontal disease is an infectious disease, with a primary bacterial etiology followed by an inflammatory process leading to destruction of the supporting structures of the teeth. Recent study using PCR to detect E. gingivalis in diseased gingival pockets, demonstrated an absence of the parasites in healthy gingival sites. Real-time PCR primer set detected protozoa in 69% of diseased pocket sites. Whereas, in healthy gingival pockets no E. gingivalis were detected [16].
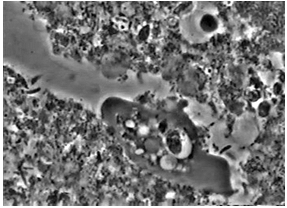
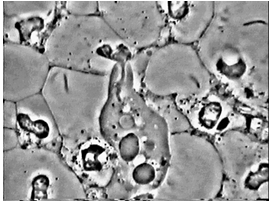
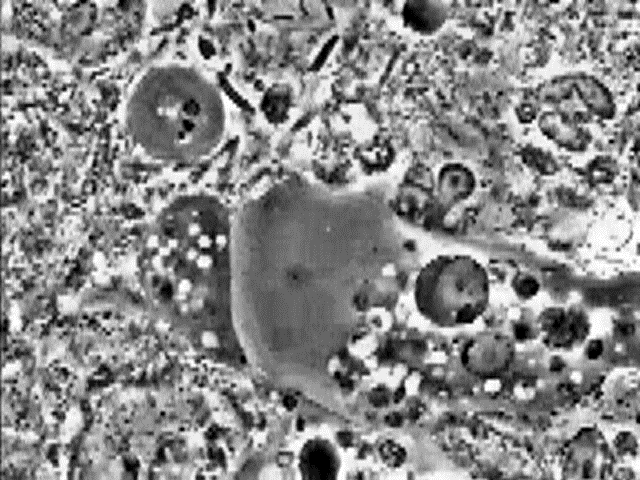
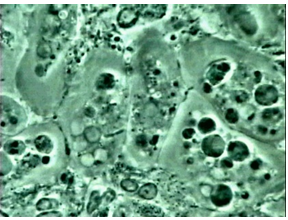
Pathogenic characteristics of E. gingivalis:
The parasite E. gingivalis shows some capping membrane phenomena (Figure 3) and directed motility (Figure 4), creating clear tubular open channels within biofilm. They phagocytize the WBC nucleus (Figure 5), a trogocythosis process termed "Exonucleophagy" and the internal portions of RBCs (Figure 6). WBC deanimation of azurophic granules by the parasite, leaves some denucleated ghost cells. Regular nesting of the parasite (Figure 7), as well as inquilinism under Actinomyces formation (Spirochete Pump) is very observed frequently. Specific scission of the parasite results in baby shaped small protozoa. Live parasites are present only with live WBCs.

The Bonner method of gingival parasite treatment:
Therapy mainly targets the elimination of all parasites from the infected pockets, with the lowering of motile bacterial activity below 1% under visual microscopy [17]. Additionally, the treatment goal is removal of all inflammatory cells including neutrophils and macrophages. Treatment is completed on a twelve month period, giving time for the patient to develop good home hygiene care and lower any invasive parasitic infections. The patient is followed up at three and six month as part of the active protocol.
The patient was placed on a home care regime with local therapy using 3% hydrogen peroxide toothpaste freshly mixed with Torrens powder, which is applied to the gingiva with a clean wet finger and left in place for 5-10 minutes then rinsed with warm water. This is repeated twice daily. Torrens powder is made by the patient in a batch that will last for several weeks or longer depending on the volume created. This is fabricated by mixing 1 part salt (Celtic or Himalayan) with 6 parts baking soda, which is placed in a blender or food processor without any liquid and ground at highspeed for 5 minutes. Allow the mixture to settle for 5 minutes then placed into a sealable jar. When ready to use a teaspoon of the powder is placed into a medicine cup and enough peroxide is added to wet the powder and is ready to be applied. Hydrogen peroxide, serves two purposes, it helps break down the oral biofilm in the pocket and changes the environment to an aerobic one versus the anaerobic environment that favor pathologic bacteria. If parasites were identified, then an additional mixture is utilized by the patient three times daily for the initial 3 month period of treatment. This is created with a tiny amount of 10% metronidazole cream combined with three finely crushed Nystatin tablets plus 2 ml oil of anise (for flavor). Clinically this is also applied in-office in the deepest pockets at the end of each appointment.
The goal of this first phase of therapy is reconstituting a normal commensal biofilm. No curettage nor root planning with sharp curettes is performed except for minimal supragingival calculus removal to limit potential for the parasites to invade the soft tissue lining of the pocket and potentially spread related to the bleeding capillaries. At the fourth month, the patient is prescribed a systemic antiparasitic medication (metronidazole) to permanently eliminate amebiasis if it was initially present and persistent at this time. Microscopy confirms commensal microbiota and the absence of inflammatory cells.
The second phase of therapy consists of four monthly subgingival calculus removals without using any sharp curettes, using sonic or ultrasonic instruments. Microscopic evaluation is used to confirm the absence of parasites. No OTC toothpaste is recommended during the eight months of active therapy and the previously described dentifrice is used. Patients, after the 8th month of treatment may return to use of a commercial toothpaste once a day along with continued use of the toothpaste created with hydrogen peroxide and Torren's powder if they so choose.
A 39 year old female patient presented for consultation following a treatment plan from her Periodontist. That treatment plan included surgical intervention to treat osseous defects and gingival issues with the possibility of extractions and grafting with implants. The patients medical history disclosed being an active smoker, fibromyalgia for 5 years and preventing her from working. She presented seeking a second opinion seeking a medical option for treatment of her periodontal disease.
Examination was performed including radiographs and periodontal charting, yielding a diagnosis of Chronic Localized Periodontitis, considered Stage III, Grade B, localized. Generalized marginal inflammation was noted with loss of the papilla between teeth #12 and 11 (US 7 and 8). (Figure 8) Periodontal charting identified two teeth (#18 and 31) having 9mm pockets with evident vertical bone resorption, three teeth (#2, 8 and 19) with 8mm pockets and four teeth #16 (US 3), 26, 27 (US 14, 15) and 34 (US 21) with 5-6mm pockets. (Figure 9) Radiographically, angular bone loss was noted on the distal of tooth #17 (US 2), mesial of tooth #11 (US 8), distal of tooth #23 (US 11), mesial of tooth #26 (US 14) and distal of teeth #27 (US 15), 37 (US 18), 36 (US 19) and 47 (US 31). Horizontal bone loss was noted in all posterior quadrants. (Figure 10) The only mobility noted was on tooth 8 which presented with a grade 1. Bleeding was noted on all teeth with greater than WNL probing. Microbiological microscopic samples were taken from the deep probing sites demonstrating white blood cells (WBCs) and Entamoeba gingivalis parasites, with elevated Orange and Red complexes.


The patient was treated with the Bonner Method for one year with no osseous grafting of the defects. At the completion of treatment, at twelve months the results demonstrated 98 % pocket elimination, resolution of all bleeding on probing. (Figure 11) The mobility that had been present on tooth 8 had resolved and no mobility was noted in the dentition. Interestingly, the Fibromyalgia completely disappeared at 4 month of active treatment. This may be related or coincidental.

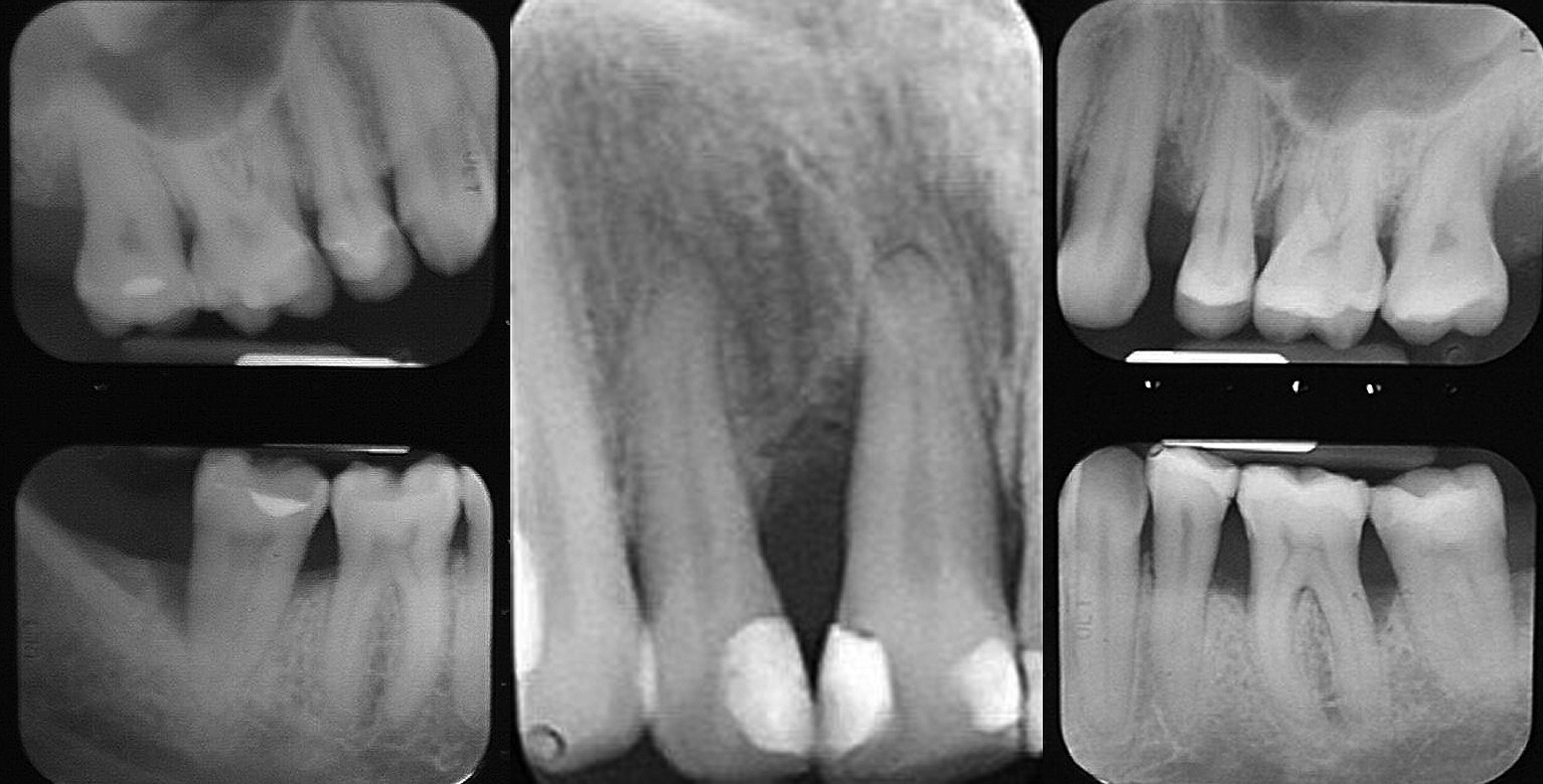
At a 10 year follow up the patient was seen with ceramic veneers present on the maxillary anterior teeth. (Figure 12) Radiographs were taken to check bone levels. (Figure 13) The angular osseous defect on the distal of tooth 8 that was initially at the apical 1/3 of the root was in a more coronal position at the middle 1/3 of the root and the tooth remained stable with no mobility. The osseous defect at the distal of tooth 23, that was at the junction of the middle and apical 1/3s initially, now was positioned in the coronal 1/3. The distal osseous defect that was on tooth 36, demonstrated bone fill as did the distal defect on tooth 47. Tooth 11, which was initially mobile and had been recommended for extraction, osseous grafting and implant placement related to the bone level, at 10 years is still present, non-mobile and stable.


Patient who have traditionally avoided dental treatment or have experienced traditional surgery in the past easily accept antiparasitic treatment, which is reached from clinical and microscopic co-examination. Many of these patients are seeking an alternative to traditional surgery and are more comfortable with the basics behind the protocol once they have seen their biofilm under video from their microscopic sampling. The most relevant point is they currently share early upfront good clinical results with their dentists objectives and are supported by a permanently improved positive change to their periodontal health. As treatment progresses, the patient sees the positive changes starting from stopping of gingival bleeding and healthier gums with less sensitivity and irritation. Microbiota microscopic examination at every monthly visit during active treatment confirms healing and elimination of the parasites. The Bonner Method is not a "cut-and-sew" procedure, tissues are not injured related to incisions associated with other periodontal surgical treatments. Pocket closure and osseous regrowth, without the need for supplemental grafting help confirm healing and with continued use of the homecare regime allow the patient to maintain gingival health long-term.
Conflict of interests:
The authors report no conflict of interests or commercial financial relationship.
Financial support:
None
Author contributions:
*Provided clinical information and technical details for the paper, reviewed article draft and provided editorial input.
**Wrote the article draft and edited based on other author feedback.
***Reviewed article draft and provided editorial input.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
