
Case Report | DOI: https://doi.org/10.31579/2693-4779/246
1Thoracic surgeon, Institute of Thoracic Diseases of Northeastern Colombia INTÓRAX, Erasmo Meoz University Hospital, Medical Duarte Clinic. Member of the departmental committee for lung cancer in northern Santander
2General Practitioner, Medical Duarte Clinic.
3General Physician at the Institute of Thoracic Diseases of Northeastern Colombia INTÓRAX, Academic and Scientific Coordinator of oncointorax, Regional Medical Coordinator INTORAX, Member of the Departmental Committee on Lung Cancer of North Santander
*Corresponding Author: Vera Gamboa Raul, Thoracic surgeon, Institute of Thoracic Diseases of Northeastern Colombia INTÓRAX, Erasmo Meoz University Hospital.
Citation: Vera G. Raul, Luis Carlos VG, Monica Alexandra MS, Melvyn Yesid DS, (2025), Traconia (Multiplier) Fish Poisoning, Clinical Research and Clinical Trials, 12(1); DOI:10.31579/2693-4779/246
Copyright: © 2025, Vera Gamboa Raul. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 13 November 2024 | Accepted: 05 December 2024 | Published: 03 January 2025
Keywords: pleural tumor; leiomyoma; vascularized; case report
Primary lung leiomyoma is a rare benign tumor of mesodermal origin that accounts for approximately 2% of all benign lung tumors 1. Leiomyoma is a smooth muscle neoplasm that commonly occurs in the genitourinary system and gastrointestinal tract of the body. 2 Primary pulmonary leiomyoma is rarely reported in the literature. We present the case of a 47-year-old male patient with a clinical picture of approximately 6 months of evolution characterized by NYHA III dyspnea, adynamia, asthenia, and mild pain in the left costal grid. A chest CT scan was requested, which reported a solid left pulmonary mass of 24 x 13 cm that compromises 80% of the highly vascularized left hemithorax.
Primary lung leiomyoma is a rare benign tumor of mesodermal origin, accounting for approximately 2% of all benign lung tumors [1]. It develops from smooth muscle fibers of the tracheobronchial tree, blood vessels, or heterotopic embryonic muscle islets in the lung, and may be parenchymal or tracheobronchial [2]. Leiomyoma is a smooth-muscle neoplasm that commonly occurs in the genitourinary system and gastrointestinal tract of the body. Primary pulmonary leiomyoma is rarely reported in the literature. Pulmonary leiomyoma is a rare condition, with most cases being secondary to metastatic lung lesions, of primary origin usually located in the uterus in female patients. Primary pulmonary leiomyoma is rare and usually occurs in parenchymal, endotracheal, or endobronchial locations [3].
The case of a 47-year-old male patient is presented. He was admitted to the emergency room with a clinical picture of 6 months' evolution given by respiratory symptoms of NYHA III type dyspnea, adynamia, asthenia, and mild pain in the left costal grid. He did not report any important or relevant history for the case. Upon admission to the service, a chest x-ray was requested, which showed great left opacity with displacement of the trachea and cardiac silhouette; the left lung is not visualized.
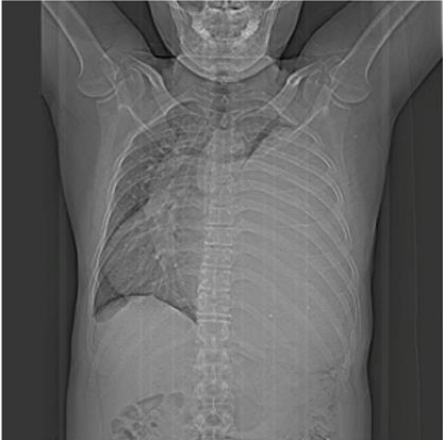
Image 1: Chest X-ray
Given the radiological findings, it was considered necessary to request a contrast- enhanced chest CT scan. which reported: a vascularized solid left pulmonary mass of 24x13 cm that compromises 80% of the left hemithorax.
An evaluation was requested by the thoracic surgery service who indicated a percutaneous biopsy and angiotac in order to assess the characteristics of the lesion along with vascular compromise. The patient required oxygen via nasal cannula at 2 L/M during his hospital stay.
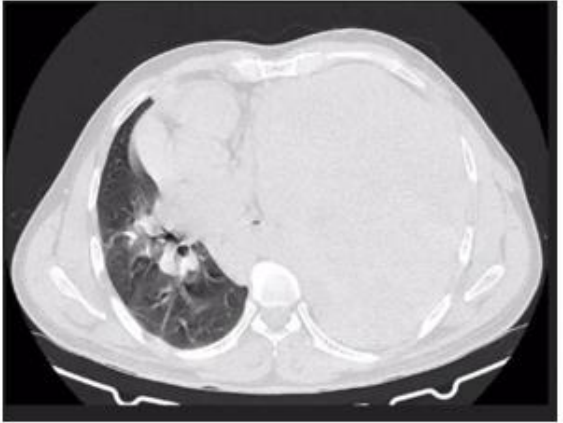
Image 2: Axial section of the pulmonary window with involvement of the left hemithorax by a tumor lesion.
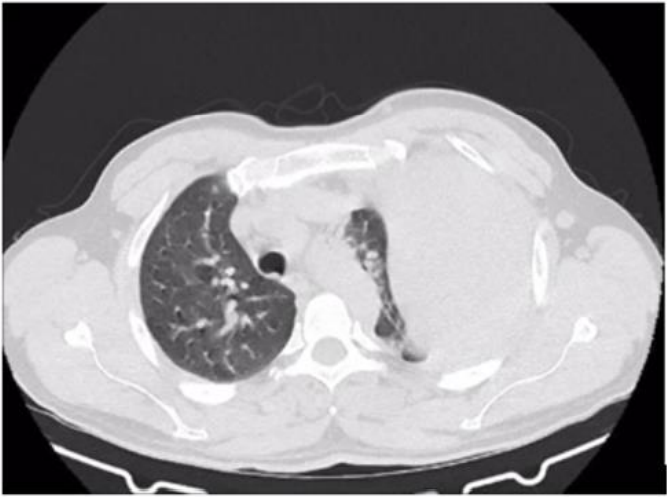
Image 3: Axial section of the pulmonary window showing displacement of the trachea and involvement of the left hemithorax due to a tumor lesion.
A percutaneous biopsy was performed with a pathological report of a lung mass with low-grade spindle cell neoplasia involving desmoid fibromatosis. Additionally, immuno-histo chemical markers were requested, which reported: solitary fibrous tumor spindle cell neoplasia vs desmoid fibromatosis. A CT angiography was performed, which showed vascularization of the lesion, predominantly of the left internal mammary artery and the ipsilateral inferior phrenic artery. The lesion is susceptible to pre-surgical embolization to reduce intraoperative bleeding. Based on the reports, an evaluation was requested by the oncology service, who
suggested surgical treatment for the T4N0M0 G1 STAGE 1B lesion, and an evaluation by interventional radiology, who performed embolization.
After each of the complementary studies, the patient was re-evaluated by thoracic surgery, who considered that the patient was a candidate for surgical management, which was performed by means of an extended posterolateral thoracotomy with open pleurec to my, which revealed a large fibrous tumor of giant left pleural origin with a vascular pedicle originating from the internal mammary artery. Ligation, mobilization of the tumor and closure by layers were performed. A large tumor lesion of approximately 6 kilos was obtained.

Image4: Resected tumor.

Image 5: Thoracotomy with tumor exposure
Following the intervention, the patient was transferred to the intensive care unit where he required management with invasive mechanical ventilation for 24 hours with subsequent extubation without complications. A control chest X-ray was taken with evidence of lung expansion and a centered trachea with no evidence of pneumothorax or hemothorax.
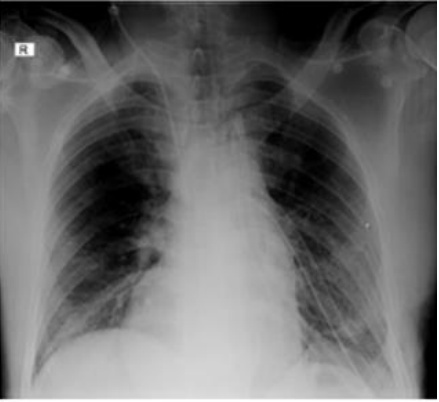
Image 6: Postoperative control chest X-ray
A pathological report of a tumor lesion was received with a description of a nodular lesion with expansive growth consisting of smooth muscle fibers, mature fibroblasts and collagen fibers, diagnosed as leiomyoma.
After a 17-day hospital stay with favorable clinical evolution, the patient was discharged with postoperative monitoring through an outpatient consultation with the thoracic surgery service.
Pulmonary leiomyoma is a rare condition, with the majority of cases occurring secondary to metastatic lung lesions, of primary origin usually located in the uterus in female patients. Primary pulmonary leiomyoma is rare and usually occurs in parenchymal, endotracheal or endobronchial locations. The nature and etiology of primary pulmonary leiomyoma are still unknown. The diagnosis of primary pulmonary leiomyoma is mainly based on radiological and pathological investigations. Immunohistochemical stains are useful to rule out other differential diagnoses; CD117 and CD34 are markers of gastrointestinal stromal tumors; HMB- 45 reactivity suggests angiomyolipoma, while S-100 usually indicates a neural origin. There are currently no guidelines for the treatment of primary pulmonary leiomyoma. The treatment strategy for pulmonary leiomyoma depends on the airway location and the size of the lesion [5].
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
